Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
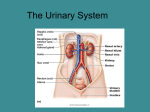
HORMONE REGULATION OF TUBULAR REABSORPTION/SECRETION Hormone What triggers it Angiotensin ↓ blood volume II ↓ BP (stims rennin-induced production of ango II. What/Where it happens Stimulates activity of Na/H+ antiporters Prosximal tubule cells Effects ↑ reabsorption of Na+, other solutes, and water, which ↑ blood volume. Aldosterone ↑ angiotensin II level and ↑ increased level of plasma K+ promote release of aldosterone by adrenal cortex. Enhances activity of Na/K+ pump in basolateral membrane and Na+ channels in apical membrane of principal cells in collecting duct. ↑ secretion of K+ and reabsoption of Na+, Cl↑ reabsorption of water which ↑ bld volume. ADH/ ↑Increased osmolarity of Stimulates insertion of water channel Vasopressin extracellular fluid or proteins (aquaporin-2) into the apical ↓ bld volume promote release of membranes of principal cells. ADH from the posterior pituitary gland. ↑ facultative reabsorption of water which ↓ osmolarity of body fluids. Atrial natriuretic peptide (ANP) ↑ excretion of Na+ in urine (natriuresis) ↑ urine output (diuresis) ↓ blood volume. Streching of atria of heart stimulates secretion of ANP Suppresses reabsorption of Na+ and water in proximal tubule and collecting duct Inhibits secretion of aldosterone and ADH RENAL CORPUSCLE GLOMERULAR FILTRATION RATE FILTERED SUBSTANCES PROXIMAL CONVOLUTED TUBULE REABSORPTION into blood of filtered Water Na+ K+ Glucose Amino acids ClHCO3Urea Ca+, Mg2+ 105-125 mL/min or fluid that is isotonic to blood Water and all solutes present in blood (except proteins) including ions, glucose, amio acids, creatinine, uric acid 65% (osmosis) 65% (Na/K pump) 65% (diffusion) 100% (symporters and facilitated diffusion) 100% (symporters and facilitated diffusion) 50% (diffusion) 80-90% (facilitated diffusion) 50% (diffusion) Variable (diffusion) SECRETION into urine of: H+ NH4+ Urea Creatinine Variable –antiporters Variable, increases in acidosis- antiporters Variable- diffusion Small amount ****At end of PC Tubule, tubular fluid is still isotonic to blood (300 mOsm/liter)**** LOOP OF HENLE REABSORPTION into blood of: Water 15% - osmosis in descending limb Na+ K+ ClHCO3Ca2+, Mg2+ 20-30% -symporters in ascending limb 20-30% -symporters in ascending limb 35% -symporters in ascending limb 10-20% -facilitated diffusion Variable –diffusion SECRETION into urine of: Urea Variable –recycling from collecting duct ****At end of loop of Henle, tubular fluid is hypotonic (100-150 mOsm/liter)**** DISTAL CONVOLUTED TUBULE REABSORPTION into blood of: Water Na+ ClCa+ 10-15% -osmosis 5% -symporters 5% -symporters Variable- stimulated by parathyroid hormone PRINCIPLE CELLS IN LATE DISTAL TUBULE AND COLLECTING DUCT REABSORPTION into bood of: Water 5-9% -insertion of water channels stimulated by ADH Na+ 1-4% - Na/K+ pump Urea Variable –recycling to loop of Henle SECRETION into urine of: K+ Variable amount to adjust for dietary intakeleakage channels ****Tubular fluid leaving the collecting duct is dilute when ADH level is low and concentrated when ADH level is high.**** INTERCALATED CELLS IN LATE DISTAL TUBULE AND COLLECTING DUCT REABSORPTION into blood of: HCO3Variable amount, depends on H+ secretion – antiporters Urea Variable – recycling to loop of Henle SECRETION into urine of: H+ Variable amounts to maintain acid-base homeostasis – H+ pumps REGULATION OF GLOMERULAR FILTERATION RATE (GFR) Type of Regulation Major stimulus Mechanism and site of action Effect on GFR RENAL AUTOREGULATION Myogenic ↑ stretching of smooth muscle Streched smooth muscle fibers contract, thereby narrowing the ↓ mechanism fibers in afferent arteriole walls lumen of the afferent arterioles due to ↑ BP Tubuloglomerular feedback ↓ release of nitric oxide (NO) by the juxtaglomerular Rapid delivery of Na+ and Cl- to apparatus causes constriction of afferent arterioles. the macula densa due to ↑ BP ↓ NEURAL REGULATION ↑ in level of activity of renal sympathetic nerves releases norepinephrine Constriction of afferent arterioles though activation of alpha1 ↓ receptors and ↑ release of renin HORMONE REGULATION ↓ blood volume or BP stimulates Constriction of both afferent and efferent arterioles. production of angiotensin II. ↓ Angiotensin II Atrial natriuretic peptide (ANP) Streching of the atria of the heart Relaxation of mesangial cells in glomerulus increases stimulates secretion of ANP capillary surface area available for filtration ↑ CHARACTERISTICS OF NORMAL URINE CHARACTERISTIC DESCRIPTION Volume Color Turbidity Odor pH Specific gravity (density) 1-2 L in 24 hrs but varies considerably Yellow or amber but varies with urine concentration and diet. Color is due to urochrome and urobilin. Concentrated urine is darker in color. Diet, medication, and certain diseases affect color. Kidney stones may produce blood in urine. Transparent when freshly voided but becomes turbid (cloudy) upon standing. Mildly aromatic but becomes ammonia-like upon standing. Some people inherit the ability to form methylmercaptan from digested asparagus that gives urine a characteristic odor. Urine of diabetics has a fruity odor due to presence of ketone bodies. 4.6-8.0 with an avg of 6.0. Will vary with diet; high protein increases acidity and vergitarian increases alkalinity 1.001-1.035 Ration of the weight of a volume of a substance to the weight of an equal volume of distilled water. The higher the concentration of solutes = higher the specific gravity. FACTORS THAT MAINTAIN BODY WATER BALANCE FACTOR MECHANISM Thirst center in Stimulates desire to drink fluids Hypothalamus Angiotensin II Stimulates secretion of aldosterone Aldosterone By promoting urinary reabsorption of Na+ and Cl-, increases water reabsorption via osmosis EFFECT Water gain if thirst is quenched. ↓ loss of water in urine ↓ loss of water in urine. Strial Natriuretic Peptide (ANP) Promotes natriureses, elevated urinary excretion of Na+ and Cl-, accompanied by ↑ loss of water in urine water Antidiuretic hormone (ADH)/ vasopressin Promotes insertion of water-channel proteins (aquaporin-2) into the apical membranes of principal cells in the collecting ducts of the kidneys. As a result, the water permeability of these cells increases and more water is reabsorbed ↓ loss of water in urine. ABNORMAL CONSTITUENTS IN URINE ABNORMAL SO…? CONSTITUEN T Albumin ∙Is normal in plasma. ∙Usually appears in only very sm amts in urine because it is too large to pass through capillary fenestration. ∙ALBUMINURIA- increase in permeability of filtration membrane due to injury or disease, increased BP, or irritation of kidney cells by substances such as bacterial toxins, ether, or heavy metals. Glucose ∙GLUCOSURIA- usually indicated diabetes mellitus. ∙May be caused by stress which can cause excessive amnts of epinephrine to be secreted. Epinph-stimulates the breakdown of glycogen and liberation of glucose from the liver. RBCs Ketone bodies ∙HEMATURIA-indicates a pathological condition d/t acute inflammation of the urinary organs as a result of disease of irritation from kidney stones, or tumors, trauma, and kidney disease. ∙Ketonuria- may indicate diabetes mellitus, anorexia, starvation, or too little carbs in the diet. Bilirubin ∙When RBCs are destroyed by macrophages, the globin portion of hemoglobin is split off and the heme is converted to biliverdin. Most of the biliverdin is converted to bilirubin, which fives bile its major pigmentation. ∙ An above normal level of bilirubin in urine is called BILIRUBINURIA. Urobilinogen ∙(a breakdown product of hemoglobin) ∙UROBILINOGENURIA-trace amounts are normal, but elevated urobilinogen may be due to hemolytic or pernicious anemia, infectious hepatitis, biliary obstruction, jaundice, cirrhosis, CHF, or infectious mononucleosis. Casts ∙(tiny masses of material that have hardened and assumed the shape of the lumen of the tubule in which they formed.) ∙Are named after the cells or substances that compose them or based on their appearance. Ex: WBC casts, RBC casts. Microbes ∙Most common: E. coli, Candida albicans, Trichomonas vaginalis. FACTORS THAT MAINTAIN BODY WATER BALANCE FACTOR MECHANISM Thirst center in Stimulates desire to drink fluids Hypothalamus Angiotensin II Stimulates secretion of aldosterone EFFECT Water gain if thirst is quenched. ↓ loss of water in urine ↓ loss of water in urine. Aldosterone By promoting urinary reabsorption of Na+ and Cl-, increases water reabsorption via osmosis Strial Natriuretic Peptide (ANP) Promotes natriureses, elevated urinary excretion of Na+ and Cl-, accompanied by ↑ loss of water in urine water Antidiuretic hormone (ADH)/ vasopressin ↓ loss of water in urine. Promotes insertion of water-channel proteins (aquaporin-2) into the apical membranes of principal cells in the collecting ducts of the kidneys. As a result, the water permeability of these cells increases and more water is reabsorbed WHAT MAINTAINS pH OF BODY FLUIDS MECHANISM COMMENTS BUFFER SYSTEMS ∙Most consist of a weak acid and the salt of that acid, which functions as a weak base. ∙They prevent drastic changes in body fluid pH Proteins ∙The most abundant buffers in body cells and blood ∙Hemoglobin inside RBCs in a good buffer Carbonic acid-bicarbonate ∙Important regulator of blood pH. ∙Most abundant buffers in ECF Phosphates ∙Important buffers in intracellular fluid and in urine Exhalation of CO2 Kidneys ∙↑ exhalation = of CO2, pH rises ∙↓ exhalation of CO2 = pH falls ∙Renal tubules secrete H+ into the urine and reabsorb HCO3- so it is not lost in the urine. BLOOD ELECTROLYTE IMBALANCES Deficiency ELECTROLYTE NAME/CAUSE S/S Excess NAME/CAUSE S/S Sodium HYPONATREMIA d/t Muscle wkness, dizziness, HA, HYPERNATREMIA Intense thirst, hypertension, 136-148 mEq/liter ↓ Na+ intake Hypotension, tachycardia, shock, Dehydration, water deprivation, edema, agitation, and ↑ Na+ loss through vomiting, diarrhea, mental confusion, coma excessive Na+ in diet or IV convulsions. ↓ aldosterone, diuretics, and excessive fluids water intake Causes hypertonicity of ECF, which pulls water out of body cells into ECF, causing cellular dehydration. Chloride HYPOCHLOREMIA d/t Muscle spasms, metabolic HYPERCHLOREMIA Lethargy, wknss, metabolic 95-105 excessive vomiting, over hydration, alkalosis, shallow respiration, d/t water loss, excessive chloride acidosis, and rapid deep ↓aldosterone CHF, and therapy with hypotension, and tetany intake, severe renal failure, breathing diuretics hyperaldosteronism, acidosis and certain drugs Potassium HYPOKALEMIA d/t m. fatigue, flaccid paralysis, HYPERKALEMIA Irritability, nausea, vomiting, 3.5-5.0 vomiting or diarrhea, ↓K+ intake, mental confusion,↑ urine output, d/t excessive intake, renal failure, diarrhea, m. wkness hyperaldosteronism, kidney disease, shallow respiration, and changes ↓aldosterone , crushing injuries Can cause death by inducting and diuretics in the electrocardiogram, flatting to body tissues, or transfusion of ventricular fibrillation. of T waves hemolyzed blood Calcium HYPOCALCEMIA N-T of fingers, hyperactive HYPERCALCEMIA Lethargy, wkness, anorexia, 5.9-10.5 d/t ↑ ca+ loss, reduced ca+ intake, reflexes, m. cramps, tetany, and d/t hyperparathyroidism, CA, nausea, vomiting, polyuria, ↑elevated levels of phosphate convulsions. Bone fx, spasms of excessive intake of vit. D and itching, bone pain, depression, hypoparathyroidism laryngeal muscles that cause Paget’s disease of bone. confusion, paresthesia, stupor, death by asphyxiation and coma. Phosphate HYPOPHOSPHATEMIA d/t Confusion, seizures, coma, chest, HYPERPOSPHATEMIA Anorexia, nausea,vomiting, 1.7-2.6 ↑ urinary losses, and muscle pain, numbness and d/t kidneys fail to excrete excess muscular weakness, hyperactive ↓ intestinal absorption, or ↑ utilization tingling or the fingers, ↓ phosphate (in renal failure,), also reflexes, tetany, and tachycardia. coordination, memory loss and d/t ↑ intake of phosphates or lethargy destruction of body cells which releases phosphates into the blood. Magnesium HYPOMAGNESEMIA d/t Wknss, irritability, tetany, HYPERMAGNESEMIA Hypotension, muscular 1.3-2.1 inadequate intake or excessive loss in deliruium, convulsions, d/t renal failure, ↑ intake of Mg weakness, or paralysis, nausea, urine or feces, alcoholism, confusion, anorexia, nausea, as in antacids; ↓aldosterone vomiting, and altered mental malnutrition, DM, and diuretic therapy vomiting, paresthesia, and deficiency and hypothyroidism. functioning. cardiac arrhythmias ACIDOSIS AND ALKALOSIS CONDITION DEFINITION COMMON CAUSES COMPENSATORY MECH. Respiratory ∙↑ Pco2 and Acidosis ∙↓ pH if there is no compensation Hypoventilation d/t emphysema, Renal:↑ excretion of H+ pulmonary edema, trauma to respiratory ↑ reabsorption of HCO3-. center, airway obstructions or dysfunction If compensation is complete, pH will be within of muscles of respiration the normal range but Pco2 will be high Respiratory ∙↓ HCO3- and Alkalosis ∙↓ pH if there is no compensation Hyperventilation d/t O2 defiiciency, pulmonalry disease, CVA or severe anxiety Renal: ↓ excretion of H+ ↓ reabsorption of HCO3If compensation is complete, pH will be within the normal range but Pco2 will be low. Metabolic Acidosis ∙↓ HCO3- and ∙↓ pH if there is no compensation Loss of bicarbonate ions d/t diarrhea, accumulation of acid (ketosis), renal dysfunction. Respiratory: Hyperventilation, which increases loss of CO2. If compensation is complete, pH will be within the normal range but HCO3- will be low. Metabolic Alkalosis ∙↑ HCO3- and ∙↑ pH if there is no compensation Loss of acid d/t vomiting, gastric suctioning, or use of certain diuretics; excessive intake of alkaline drugs. Respiratory: Hypoventilation, which slows loss of CO2. If compensation is complete, pH will be within the normal range but HCO3- will be high.