Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
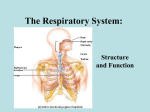
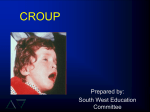
SEMIOTICS OF THE RESPIRATORY SYSTEM DISEASES. THE RESPIRATORY DISTRESS SYNDROMES AND RESPIRATORY FAILURE, GENERAL CLINICAL SYMPTOMS Acute viral infections of respiratory tracts • Acute viral infections of respiratory tracts (AVIR) are a group of diseases of the upper and medium respiratory tracts, mostly of virus (H. Influenzae, parainfluenzae, adeno- and rhino-viruses, virus-ECHO, etc), sometimes of microbial (B-hemolytic streptococcus of group A, pneumococcus) etiology. • Focal manifestations of AVIR are: rhinitis, pharyngitis, laryngitis; in most cases bronchitis in children is also considered as AVIR. Acute rhinitis • Is the inflammation of mucous membrane of the nose, mostly of viral etiology. • Clinical manifestations: • Sneezing. • Complicated nasal respiration. • The excretion of mucus from the nose (at the beginning serous, watery, then more thick). • Cough (it is caused by the irritation of the back wall of pharynx by mucus refluxing from the nose). • The general manifestations — weakness, headache, fever; at breastfeeding age — complicated process of sucking. Acute Pharyngitis • Is an inflammation of the mucous membrane of oropharynx — can be both of viral and bacterial etiology. In the latter case, it is often caused by p-hemolytic streptococcus of group A, which can be a factor of rheumatic fever, glomerulonephritis. • Clinical manifestations: • Hyperemia of the pharynx. • Increased follicle on the back wall of oropharynx— a symptom of 'cobblestone road'. • Pain at swallowing. • Coughing. • General manifestations of intoxication. • In children of early age AVIR can be complicated with otitis. Acute laryngitis • Is an inflammation of the mucous membrane of the larynx of viral or bacterial etiology. Children under 3 years of age with laryngitis have stenosis (i.e. narrowing) of the opening of larynx, which is caused by the anatomic features at this age recollect. The developing syndrome refers to 'false croup ( pseudo-croup)' and the diagnosis is constrictive laryngotracheitis. • Clinical manifestations: • 'Barking' cough. • A hoarse voice, in severe cases — aphonia. • Inspiratory dyspnea Tachycardia. • Weakness, lethargy, acute laryngitis which is often interchangeable with restlessness. • The general manifestations, characteristic for intoxication. • The development of false croup is dangerous for life of the child, the progressing stenosis can lead to asphyxia — the pathological condition menacing the life in the form of suffocation. Simultaneously, tachycardia is replaced by bradycardia, and then heart failure follows. The only way of treatment is intubation or tracheostomy. Croup • Is a common, primarily pediatric viral respiratory tract illness. As its alternative names, laryngotracheitis and laryngotracheobronchitis, indicate, croup generally affects the larynx and trachea, although this illness may also extend to the bronchi. It is the most common etiology for hoarseness, cough, and onset of acute stridor in febrile children. Symptoms of coryza may be absent, mild, or marked. The vast majority of children with croup recover without consequences or sequelae; however, it can be life-threatening. • Croup manifests as hoarseness, a seal-like barking cough, and a variable degree of respiratory distress. However, morbidity is secondary to narrowing of the larynx and trachea below the level of the glottis (subglottic region), causing the characteristicaudible inspiratory stridor. Stridoris • A common symptom in patients with croup. The acute onset of this abnormal sound alarms parents enough to prompt an urgent care or emergency department (ED) visit. Stridor is an audible harsh, highpitched, musical sound produced by turbulent airflow through a partially obstructed upper airway. This partial airway obstruction can be present at the level of the supra-glottis, glottis, sub-glottis, and/or trachea. During inspiration, areas of the airway that are easily collapsible (e.g, supra-glottic region) are suctioned closed because of negative intraluminal pressure generated during inspiration. These same areas are forced open during expiration. Depending on timing within the respiratory cycle, stridor can be heard on inspiration, expiration, or in both (biphasic; inspiratory and expiratory). Inspiratory stridor suggests a laryngeal obstruction, whereas expiratory stridor suggests tracheobronchial obstruction. Biphasic stridor indicates either a subglottic or glottic anomaly. An acute onset of marked inspiratory stridor is one of the hallmarks of croup; however, there also may be less audible expiratory stridor. Young children who present with stridor require a meticulous evaluation to determine the etiology and, most importantly, to exclude rare life-threatening causes. Although croup is usually a mild, self-limited disease, upper airway obstruction may result in respiratory distress and even death. Physical Examination • The physical presentation of croup has wide variation. Most children have no more than a "croupy" cough and hoarse cry. Some may have stridor only upon activity or agitation, whereas others have audible stridor at rest and clinical evidence of respiratory distress. Paradoxically, a severely affected child may have "quiet" stridor secondary to a greater degree of airway obstruction. The child with croup typically does not appear toxic. • The child's symptoms can range from minimal inspiratory stridor to severe respiratory failure secondary to airway obstruction. In mild cases, respiratory sounds at rest are normal; however, mild expiratory wheezing may be heard. Children with more severe cases have inspiratory and expiratory stridor at rest with visible suprasternal, intercostal, and subcostal retractions. Air entry may be poor. Lethargy and agitation may be due to marked respiratory difficulty and, hence, hypoxemia and increasing hypercarbia. • Other warning signs of severe respiratory disease include tachypnea, tachycardia out of proportion to fever, and hypotonia. Children unable to maintain adequate oral intake, results in compromised hydration and can lead to dehydration. Cyanosis is a late, ominous sign. • Croup is primarily a clinical diagnosis, with the diagnostic clues based on presenting history and physical examination findings. • Laboratory test results rarely contribute to confirming this diagnosis. The complete blood cell (CBC) count is usually nonspecific, although the white blood cell (WBC) count and differential may suggest a viral cause with lymphocytosis. Identifying the specific viral etiology (eg, parainfluenza virus serotype, respiratory syncytial virus [RSV]) via nasal washings is typically not necessary but may be useful to determine isolation needs in the hospital care setting or, in the case of influenza A, to decide whether antiviral therapy should be initiated. • Pulse oximetry readings are within the normal reference range for most patients; however, this monitoring is helpful to assess for the need for supplemental oxygen support and to monitor for worsening respiratory compromise as evident with tachypnea and poor maintenance of oxygen saturations. Standardly, arterial blood gas (ABG) measurements are unnecessary and do not reveal hypoxia or hypercarbia unless respiratory fatigue ensues. • Patients who present with fevers, tachypnea, and history of decreased oral fluid intake require evaluation of their hydration status. Compromised oral intake and inability to maintain needed fluid volume may require intravenous fluid support to stabilize, support and sustain their ongoing fluid requirements. Procedures • Laryngoscopy is indicated only in unusual circumstances (e.g, the course of illness is not typical, the child has symptoms that suggest an underlying anatomic or congenital disorder). This procedure may also be required in patients with bacterial tracheitis to obtain the necessary cultures in an attempt to tailor antibiotic treatment. • Other procedures that may be indicated and may require the guidance of a pediatric otolaryngologist include the following: • Direct laryngoscopy if the child in not in acute distress • Fiberoptic laryngoscopy • Bronchoscopy (for cases of recurrent croup to rule out airway disorders) Procedures • Radiography. Plain films can verify a presumptive diagnosis or exclude other disorders causing stridor and hence mimic croup. A lateral neck radiograph can help detect clinical diagnoses such as an aspirated foreign body, esophageal foreign body, congenital subglottic stenosis, epiglottitis, retropharyngeal abscess or bacterial tracheitis (thickened trachea).Most importantly, croup is a clinical diagnosis. Radiographs can be used as a tool to help confirm this diagnosis, but they are not required in uncomplicated cases. • Concurrently, careful monitoring of the heart rate (for tachycardia), respiratory rate (for tachypnea), respiratory mechanics (for sternal wall retractions), and pulse oximetry (for hypoxia) are important. Assessment of the patient’s hydration status, given the risk of increased insensible losses from fever and tachypnea, along with a history of decreased oral intake, is also imperative. Treatment • Urgent care or emergency department treatment of croup depends on the degree of respiratory distress. In mild croup, a child may present with only a croupy cough and may require nothing more than parental reassurance, given alertness, baseline minimal respiratory distress, proper oxygenation, and stable fluid status. The caregivers may only need education regarding the course of the disease and supportive homecare guidelines. • However, any infant/child who presents with significant respiratory distress/complaints with stridor at rest must have a thorough clinical evaluation to ensure the patency of the airway and maintenance of effective oxygenation and ventilation. Keep young children as comfortable as possible, allowing him or her to remain in a parent's arms and avoiding unnecessary painful interventions that may cause agitation, respiratory distress, and lead to increased oxygen requirements. Persistent crying increases oxygen demands, and respiratory muscle fatigue can worsen the obstruction. • Concurrently, careful monitoring of the heart rate (for tachycardia), respiratory rate (for tachypnea), respiratory mechanics (for sternal wall retractions), and pulse oximetry (for hypoxia) are important. Assessment of the patient’s hydration status, given the risk of increased insensible losses from fever and tachypnea, along with a history of decreased oral intake, is also imperative. Treatment • Infants and children with severe respiratory distress or compromise may require 100% oxygenation with ventilation support, initially with a bag-valve-mask device. If the airway and breathing require further stabilization due to increasing respiratory fatigue and hence, worsening hypercarbia, (as evident by ABG) the patient should be intubated with an endotracheal tube. Intubation should be accomplished with an endotracheal tube that is 0.5-1 mm smaller than predicted. Once airway stabilization is achieved, these patients are transferred for their ongoing care to a pediatric intensive care unit. • The current cornerstones of treatment in the urgent care clinics or emergency departments are corticosteroids and nebulized epinephrine; steroids have proven beneficial in severe, moderate, and even mild croup. In the straightforward cases of croup, antibiotics are not prescribed, as the primary cause is viral. Lack of improvement or worsening of symptoms can be due to a secondary bacterial process, which would require the use of antimicrobials for treatment. Typically, these patients initially would have had moderate-to-severe croup scores, requiring inpatient care and observation. Epiglottitis • Also termed supraglottitis or epiglottiditis, is an inflammation of structures above the insertion of the glottis and is most often caused by bacterial infection. Before widespread Haemophilus influenzae type b (Hib) vaccination, H influenzae caused almost all pediatric cases of epiglottitis. • Affected structures include the epiglottis, aryepiglottic folds, arytenoid soft tissue, and, occasionally, the uvula. The epiglottis is the most common site of swelling. Acute epiglottitis and associated upper airway obstruction has significant morbidity and mortality and may cause respiratory arrest and death. • The following image illustrates the difference between a normal pediatric airway and one from a child with fatal epiglottitis. Complications • During the bacteremia phase of the disease, other foci of infection are possible. Pneumonia is the most commonly cited associated illness, followed by otitis media. Meningitis has also been reported in association with epiglottitis. • As with other causes of upper airway obstruction, pulmonary edema can be observed after the airway has been secured. Accidental extubating and respiratory arrest are the 2 most common complications, and accidental extubation can cause additional complications. Cervical adenitis, tonsillitis, and otitis media have also been documented. Complications • • • • • • • • • • • • Aspiration Endotracheal tube dislodgement Extubation Tracheal stenosis Pneumothorax or pneumomediastinum Epiglottic abscess Adenitis Cervical cellulitis Septic shock Pulmonary edema (rare) Cerebral anoxia Death from asphyxia • In classic cases involving bacteremia with Haemophilus influenzae, other structures may have concomitant infectious processes. These may include the following: • Meningitis • Pneumonia • Septicemia • Cellulitis • Septic arthritis • Otitis media • Pericarditis (rare) Physical Examination. • The child appears toxic; shock may occur early in the course of the disease. Marked restlessness, irritability, and extreme anxiety are common. The child may sit with his or her chin hyperextended and body leaning forward (ie, tripod or sniffing position) to maximize air entry and improve diaphragmatic excursion (see the following image).The mouth may be open wide and the tongue may protrude; an affected child often drools, because swallowing is difficult or painful. An erythematous and classic swollen, cherry red epiglottis can often be seen during careful examination of the oropharynx, although this examination should not be attempted if it may compromise respiratory effort. Early on, the child may have stridulous respirations, but as the disease progresses, airway sounds may diminish. Stridor can occur with marked suprasternal, subcostal, and intercostal retractions. Anterior neck examination may reveal tender adenopathy. In the older child, pain may be noted on movement of the hyoid bone. Cyanosis, which occurs late in the course of the condition, indicates a poor prognosis. Securing an airway is the overriding priority. An expert in pediatric airway management should always perform an endotracheal intubation on any child with suspected epiglottitis before radiography or blood work is performed. Workup • Laryngoscopy is the best way to confirm the diagnosis, but it is not advised to attempt any procedures without securing the airway. Simply depressing the child's tongue with a tongue blade may visualize the epiglottitis in some situations. Some concern exists regarding the safety of such procedures, which can provoke anxiety and increased respiratory effort during examination leading to airway obstruction. • Laboratory evaluation is nonspecific in patients with epiglottitis and should be performed once the airway is secured. The white blood cell (WBC) count may be elevated from 15,000-45,000 cells/µL with a predominance of bands. Histologic examination reveals massive infiltration with polymorphonuclear leukocytes and inflammatory edema. • Classic cases of epiglottitis require no radiographic evaluation; however, radiography may be needed in some cases to confirm the diagnosis and to exclude other potential causes of acute airway obstruction. When radiography is required to exclude other diagnoses, perform portable radiography at the patient's bedside. • Recommendations for computed tomography (CT) scanning of the neck in early or unusual cases have been suggested,although great care should be used because of the positioning of the patient. • If epiglottitis is in the differential diagnosis, the child should never be left alone even if imaging studies are being obtained. The child should always be accompanied by personnel who are able to achieve rapid airway access if needed. • Fiberoptic Laryngoscopy • Laryngoscopy can help exclude other diagnoses in an older child who is cooperative. However, do not perform a laryngoscopy if the procedure might increase anxiety, which can exacerbate the airway obstruction. • The naris can be anesthetized with lidocaine jelly before inserting the fiberoptic laryngoscope. Insert the laryngoscope through the naris, advancing it slowly into the supraglottic region. The epiglottis should be easily visualized to determine the presence of swelling. • Also termed needle cricothyrotomy or translaryngeal ventilation, percutaneous transtracheal ventilation is a temporizing method used to treat cases of severe epiglottitis when the patient cannot be intubated before a formal tracheostomy. • Percutaneous transtracheal ventilation involves inserting a needle through the cricothyroid membrane, which lies inferior to the thyroid cartilage and superior to the cricoid cartilage. The cricothyroid arteries typically course through the superior portion of the membrane. • Treatment in patients with epiglottitis is directed toward relieving the airway obstruction and eradicating the infectious agent. Optimally, initial treatment is provided by a pediatric anesthesiologist and either a pediatric surgeon or a pediatric otolaryngologist. Once the airway is controlled, a pediatric intensivist is required for inpatient management. • Avoid procedures that might increase the child's anxiety until after the child's airway is secured. Procedures such as venipuncture and intravenous access, although appropriate in most cases involving children with acute epiglottitis, may heighten anxiety and precipitate airway compromise. • Do not underestimate the potential for sudden deterioration. As soon as epiglottitis is suspected, initiating and mobilizing a medical and surgical team capable of securing the airway is imperative. • Never place a child in a supine position (other than during the endotracheal intubation procedure), because immediate respiratory arrest in this position has been reported Acute bronchitis • is a clinical syndrome produced by inflammation of the trachea, bronchi, and bronchioles. In children, acute bronchitis usually occurs in association with viral respiratory tract infection. Acute bronchitis is rarely a primary bacterial infection in otherwise healthy children. • Examples of normal airway color and architecture and an airway in a patient with chronic bronchitis are shown below. • Normal airway color and architecture (in a child with mild tracheomalacia). Airway of a child with chronic bronchitis shows erythema, loss of normal architecture, and swelling. • Symptoms of acute bronchitis usually include productive cough and sometimes retrosternal pain during deep breathing or coughing. Generally, the clinical course of acute bronchitis is selflimited, with complete healing and full return to function typically seen within 10-14 days following symptom onset. • Chronic bronchitis has also been defined as a complex of symptoms that includes cough that lasts more than 1 month or recurrent productive cough that may be associated with wheezing or crackles on auscultation. Elements of these descriptors are present in the working definitions of asthma, as well. Acute Bronchitis • Treatment of chronic bronchitis in pediatric patients includes rest, use of antipyretics, adequate hydration, and avoidance of smoke. • Analgesics and antipyretics target the symptoms of pediatric bronchitis. In chronic cases, bronchodilator therapy should be considered. Oral corticosteroids should be added if cough continues and the history and physical examination findings suggest a wheezy form of bronchitis. • Acute bronchitis begins as a respiratory tract infection that manifests as the common cold. Symptoms often include coryza, malaise, chills, slight fever, sore throat, and back and muscle pain. • The cough in these children is usually accompanied by a nasal discharge. The discharge is watery at first, then after several days becomes thicker and colored or opaque. It then becomes clear again and has a mucoid watery consistency before it spontaneously resolves within 7-10 days. Purulent nasal discharge is common with viral respiratory pathogens and, by itself, does not imply bacterial infection. • Initially, the cough is dry and may be harsh or raspy sounding. The cough then loosens and becomes productive. Children younger than 5 years rarely expectorate. In this age group, sputum is usually seen in vomitus (ie, posttussive emesis). Parents frequently note a rattling sound in the chest. Hemoptysis, a burning discomfort in the chest, and dyspnea may be present. Physical Examination • Lungs may sound normal. Crackles, rhonchi, or large airway wheezing, if any, tend to be scattered and bilateral. The pharynx may be injected. • For maximal cost-effectiveness, diagnostic laboratory tests for bronchitis should be performed in a stepwise manner. Patients with uncomplicated acute respiratory illness who are cared for in an outpatient setting need little, if any, laboratory evaluation. • Testing in Hospitalized Children • For hospitalized children, serum C-reactive protein screen, respiratory culture, rapid diagnostic studies, and serum cold agglutinin testing (at the appropriate age) help to classify whether the infection is caused by bacteria, atypical pathogens (eg, Chlamydia pneumoniae, Mycoplasma pneumoniae), or viruses. Obtain a blood or sputum culture if antibiotic therapy is under consideration. Physical Examination • For the child who has been intubated, collect a specimen of deep respiratory secretions for Gram stain, chlamydial and viral antigen assays, and bacterial and viral cultures. • Chest Radiography • Chest films generally appear normal in patients with uncomplicated bronchitis. Abnormal findings are minimal and may include atelectasis, hyperinflation, and peribronchial thickening. Focal consolidation is not usually present. These findings are similar to the radiographic findings in patients with asthma. Radiographic findings may help exclude other diseases or complications, particularly when abnormalities in either vital signs or pulse oximetry findings are present. • Pulmonary Function Testing Physical Examination • For the child admitted to the hospital with a possible chlamydial, mycoplasmal, or viral lower respiratory tract infection for which specific therapy is considered, test nasopharyngeal secretions for these pathogens, using antigen or polymerase chain reaction testing for Chlamydia species and respiratory syncytial, parainfluenza, and influenza viruses or viral culture. Results will guide appropriate antimicrobial selection. • Pulmonary function tests may show airflow obstruction that is reversible with bronchodilators. Bronchial challenge, such as with exercise or with histamine or methacholine exposure, may demonstrate the airway hyperreactivity characteristic of asthma. • Bronchoscopy • On fiberoptic bronchoscopy, a diagnosis of chronic bronchitis is suggested if the airways appear erythematous and friable. Bronchoalveolar lavage may be useful in establishing an infectious cause. Bronchoalveolar lavage may reveal numerous monocytic or polymorphonuclear inflammatory cells. In children with chronic aspiration of gastric contents, lipids may be present within macrophages. Treatment • Emergency care for acute bronchitis or exacerbation of chronic bronchitis must focus on ensuring that the child has adequate oxygenation. Outpatient care is appropriate unless bronchitis is complicated by severe underlying disease. General measures include rest, use of antipyretics, adequate hydration, and avoidance of smoke. • Proper care of any underlying disorder is of paramount importance. Consideration of asthma and adequate therapy are critical to an early response. • Febrile patients should increase oral fluid intake. Instruct the patient to rest until the fever subsides. • Resolution of symptoms, normal findings on physical examination, and normal pulmonary function test results indicate the end of the need for acute treatment. Patients in whom asthma is diagnosed will likely require ongoing therapy for that disease. Patients with defined hypogammaglobulinemia may need periodic immunoglobulin replacement treatments. These are best coordinated with the assistance of a pediatric allergy and immunology or pulmonary specialist. • Medication Summary • In acute bronchitis, medical therapy generally targets symptoms and includes use of analgesics and antipyretics. • In chronic bronchitis, bronchodilator therapy should be considered and instituted; either a beta-adrenergic agonist, such as albuterol or metaproterenol, or theophylline may be effective. Beta-adrenergic agents are less toxic, have a more rapid onset of action than theophylline, and do not require monitoring of levels. Inhaled corticosteroids may be effective. • In the child who continues to cough despite a trial of bronchodilators and in whom the history and physical examination findings suggest a wheezy form of bronchitis, oral corticosteroids should be added. If the response is suboptimal or if fever persists, antibiotic therapy with an agent such as a macrolide or beta-lactamase–resistant antimicrobial may be considered. • Antibiotics should not be the primary therapy. They usually do not result in a cure and may delay the start of more appropriate asthma therapies. • Pneumonia • Pneumonia and other lower respiratory tract infections are the leading causes of death worldwide. Because pneumonia is common and is associated with significant morbidity and mortality, properly diagnosing pneumonia, correctly recognizing any complications or underlying conditions, and appropriately treating patients are important. Although in developed countries the diagnosis is usually made on the basis of radiographic findings, the World Health Organization (WHO) has defined pneumonia solely on the basis of clinical findings obtained by visual inspection and on timing of the respiratory rate. • Pneumonia may originate in the lung or may be a focal complication of a contiguous or systemic inflammatory process. Abnormalities of airway patency as well as alveolar ventilation and perfusion occur frequently due to various mechanisms. These derangements often significantly alter gas exchange and dependent cellular metabolism in the many tissues and organs that determine survival and contribute to quality of life. Recognition, prevention, and treatment of these problems are major factors in the care of children with pneumonia. Pneumonia • One particular form of pneumonia present in the pediatric population, congenital pneumonia, presents within the first 24 hours after birth. For more information • Other respiratory tract diseases such as croup (laryngotracheobronchitis), bronchiolitis, and bronchitis are beyond the scope of this article and are not discussed further. Diagnosis • The signs and symptoms of pneumonia are often nonspecific and widely vary based on the patient’s age and the infectious organisms involved. • Observing the child’s respiratory effort during a physical exam is an important first step in diagnosing pneumonia. The World Health Organization (WHO) respiratory rate thresholds for identifying children with pneumonia are as follows: • Children younger than 2 months: Greater than or equal to 60 breaths/min • Children aged 2-11 months: Greater than or equal to 50 breaths/min • Children aged 12-59 months: Greater than or equal to 40 breaths/min • Assessment of oxygen saturation by pulse oximetry should be performed early in the evaluation when respiratory symptoms are present. Cyanosis may be present in severe cases. Capnography may be useful in the evaluation of children with potential respiratory compromise. • Other diagnostic tests may include the following: • Auscultation by stethoscope: • The sine qua non for pneumonia has always been the presence of crackles or rales. Although often present, focal crackles as a stand-alone physical examination finding is neither sensitive nor specific for the diagnosis of pneumonia. Additionally, not all children with pneumonia have crackles. Diagnosis • Rales, rhonchi, and cough are all observed much less frequently in infants with pneumonia than in older individuals. If present, they may be caused by noninflammatory processes, such as congestive heart failure, condensation from humidified gas administered during mechanical ventilation, or endotracheal tube displacement. Although alternative explanations are possible, these findings should prompt careful consideration of pneumonia in the differential diagnosis. • Other examination findings suggestive of pneumonia include asymmetry of breath sounds in infants, such as focal wheezing or decreased breath sounds in one lung field, and asymmetry of chest excursions, which suggest air leak or emphysematous changes secondary to partial airway obstruction. Similarly, certain more diffuse lung infections (eg, viral infections) may result in generalized crackles or wheezing. • Cultures: • In general, blood culture results are positive in 10-15% of patients with pneumococcal pneumonia. The percentage is even less in patients with Staphylococcus infection. However, a blood culture is still recommended in complicated cases of pneumonia. It may be the only way to identify the pathogen and its antimicrobial susceptibility patterns. • Serology: Diagnosis • Because of the relatively low yield of cultures, more efforts are under way to develop quick and accurate serologic tests for common lung pathogens, such as M pneumoniae, Chlamydophila species, and Legionella. • Complete blood cell count (CBC): • Testing should include a CBC count with differential and evaluation of acute-phase reactants (ESR, CRP, or both) and sedimentation rate. The total white blood cell (WBC) count and differential may aid in determining if an infection is bacterial or viral, and, together with clinical symptoms, chest radiography, and ESR can be useful in monitoring the course of pneumonia. In cases of pneumococcal pneumonia, the WBC count is often elevated. Diagnosis • Chest radiography: • Chest radiography is indicated primarily in children with complications such as pleural effusions and in those in whom antibiotic treatment fails to elicit a response. Computed tomography (CT) scanning of the chest and ultrasonography are indicated in children with complications such as pleural effusions and in those in whom antibiotic treatment fails to elicit a response. • Ultrasonography • New data show that point-of-care ultrasonography accurately diagnoses most cases of pneumonia in children and young adults. Ultrasonography may eventually replace x-rays for diagnosis. Management • Initial priorities in children with pneumonia include the identification and treatment of respiratory distress, hypoxemia, and hypercarbia. Grunting, flaring, severe tachypnea, and retractions should prompt immediate respiratory support. Children who are in severe respiratory distress should undergo tracheal intubation if they are unable to maintain oxygenation or have decreasing levels of consciousness. Increased respiratory support requirements such as increased inhaled oxygen concentration, positive pressure ventilation, or CPAP are commonly required before recovery begins. • Antibiotics • The majority of children diagnosed with pneumonia in the outpatient setting are treated with oral antibiotics. High-dose amoxicillin is used as a first-line agent for children with uncomplicated community-acquired pneumonia. Second- or third-generation cephalosporins and macrolide antibiotics such as azithromycin are acceptable alternatives. Combination therapy (ampicillin and either gentamicin or cefotaxime) is typically used in the initial treatment of newborns and young infants. Management • Hospitalized patients are usually treated with an advanced-generation intravenous cephalosporin, often in combination with a macrolide. Children who are toxic appearing should receive antibiotic therapy that includes vancomycin (particularly in areas where penicillin-resistant pneumococci and methicillin-resistant S aureus [MRSA] are prevalent) along with a second- or third-generation cephalosporin. • Vaccines • Aside from avoiding infectious contacts (difficult for many families who use daycare facilities), vaccination is the primary mode of prevention. Influenza vaccine is recommended for children aged 6 months and older. The pneumococcal conjugate vaccine (PCV13) is recommended for all children younger than 59 months old. The 23-valent polysaccharide vaccine (PPVSV) is recommended for children 24 months or older who are at high risk of pneumococcal disease. Pediatric Airway Foreign Body Background • The human body has numerous defense mechanisms to keep the airway free and clear of extraneous matter. These include the physical actions of the epiglottis and arytenoid cartilages in blocking the airway, the intense spasm of the true and false vocal cords any time objects come near the vocal cords, and a highly sensitive cough reflex with afferent impulses generated throughout the larynx, trachea, and all branch points in the proximal tracheobronchial tree. However, none of these mechanisms is perfect, and foreign bodies frequently lodge in the airways of children. • Often, the child presents after a sudden episode of coughing or choking while eating with subsequent wheezing, coughing, or stridor. However, in numerous cases, the choking episode is not witnessed, and, in many cases, the choking episode is not recalled at the time the history is taken. • The most tragic cases occur when acute aspiration causes total or near-total occlusion of the airway, resulting in death or hypoxic brain damage. • The more difficult cases are those in which aspiration is not witnessed or is unrecognized and, therefore, is unsuspected. • In these situations, the child may present with persistent or recurrent cough, wheezing, persistent or recurrent pneumonia, lung abscess, focal bronchiectasis, or hemoptysis. • If the material is in the subglottic space, symptoms may include stridor, recurrent or persistent croup, and voice changes. • In one series, as many as one third of parents were unaware of the aspiration or remembered an event that occurred more than a week before the presentation.In as many as 25% of cases, aspiration occurred more than one month before presentation. Consequently, a high index of suspicion in addition to the history may be necessary to reach the diagnosis. In another series of 280 foreign body aspirations, 47% were detected more than 24 hours after the aspiration.However, 99% had signs or symptoms or abnormal plain radiographs before the bronchoscopy. Physical • Major findings include new abnormal airway sounds, such as wheezing, stridor, or decreased breath sounds. These sounds are often, but not always, unilateral. • Sounds are inspiratory if the material is in the extrathoracic trachea. If the lesion is in the intrathoracic trachea, noises are symmetric but sound more prominent in the central airways. These sounds are a coarse wheeze (sometimes referred to as expiratory stridor) heard with the same intensity all over the chest. • Once the foreign body passes the carina, the breath sounds are usually asymmetric. However, remember that the young chest transmits sounds very well, and the stethoscope head is often bigger than the lobes. A lack of asymmetry should not dissuade the observer from considering the diagnosis. • Similarly, a lack of findings upon physical examination does not preclude the possibility of an airway foreign body. • Radiography: • Most aspirated foreign bodies are food material and are radiolucent. Thus, one has to look indirectly for signs of the foreign body. • Aspirated foreign body (backing to an earring) lodged in the right main stem bronchus. • Fluoroscopy: • Fluoroscopy of the chest may be helpful in showing focal air trapping, paradoxical diaphragmatic motion, or both. • CT scanning: • Chest CT scanning may reveal the material in the airway, focal airway edema, or focal overinflation not detected using plain radiography. Even if no foreign body is evident on any of the radiographic studies, a foreign body may still be present, and a bronchoscopy should be performed if the suspicion is high. Procedures • Bronchoscopy • If the history and physical findings are diagnostic, no workup is needed. The child should immediately be referred for rigid bronchoscopy. Although a flexible bronchoscopy is useful in detecting a foreign body, removing most foreign bodies using the currently available flexible bronchoscopes and their attachments is difficult. However, removal using a fiberoptic bronchoscope has been reported. • If the possiblity of foreign body is significant but has not been diagnosed by phyical examination or radiographic studies, flexible bronchoscopy should be strongly considered. • Heimlich maneuver • If the child has respiratory distress and is unable to speak or cry, complete airway obstruction is probable, and the likelihood of morbidity or mortality is high. In those cases, a Heimlich maneuver may be performed. If the child is able to speak, the Heimlich maneuver is contraindicated because it might dislodge the material to an area where it could cause complete airway obstruction. Medical Care • Bronchodilators and corticosteroids should not be used to remove the foreign body, and chest physical therapy with postural drainage may dislodge the material to an area where it may cause more harm, such as at the level of the vocal cords. • Medications are not necessary before removal, although the endoscopist may observe enough focal swelling after the material is removed to recommend a short course of systemic corticosteroids. • Unless the airway secretions are infected with organisms present, antibiotics are not necessary. Surgical Care • Surgical therapy for an airway foreign body involves endoscopic removal, usually with a rigid bronchoscope. Consultations • If the diagnosis is in question or a flexible bronchoscopy is needed, a pediatric pulmonologist should be consulted. • A pediatric surgeon or pediatric otolaryngologist usually performs the rigid bronchoscopy if necessary. Medication Summary • No medications are needed. If significant swelling is observed in the airway or if granulation tissue is present, a corticosteroid (eg, prednisolone, prednisone) may be administered. Unless airway secretions are infected, antibiotics are not helpful or necessary. Asthma • Asthma is a chronic inflammatory disorder of the airways characterized by an obstruction of airflow. Among children and adolescents aged 5-17 years, asthma accounts for a loss of 10 million school days annually and costs caretakers $726.1 million per year because of work absence. • Essential update: BPA exposure and risk of childhood asthma • Results of a prospective birth cohort study of 568 women in the third trimester of pregnancy showed postnatal bisphenol A (BPA) exposure was associated with significantly increased risk for wheeze and asthma in offspring at ages 3, 5, and 7 years. Investigators measured urine BPA concentrations in mothers and their children to estimate BPA exposure. After adjusting for secondhand smoke exposure and other asthma risk factors, postnatal BPA exposure was associated with a 40% to 50% increased risk for wheeze and asthma. The study also found that exposure during the third trimester was inversely associated with risk for wheeze at age 5. Signs and symptoms • The clinician should establish whether the patient has any of the following symptoms: • Wheezing: A musical, high-pitched whistling sound produced by airflow turbulence is one of the most common symptoms of asthma • Cough: Usually, the cough is nonproductive and nonparoxysmal; coughing may be present with wheezing • Cough at night or with exercise: Coughing may be the only symptom of asthma, especially in cases of exercise-induced or nocturnal asthma; children with nocturnal asthma tend to cough after midnight, during the early hours of morning • Shortness of breath • Chest tightness: A history of tightness or pain in the chest may be present with or without other symptoms of asthma, especially in exercise-induced or nocturnal asthma • Sputum production • In an acute episode of asthma, symptoms vary according to the episode’s severity. Infants and young children suffering a severe episode display the following characteristics: • Breathless during rest • Not interested in feeding • Sit upright • Talk in words (not sentences) • Usually agitated • With imminent respiratory arrest, the child displays the aforementioned symptoms and is also drowsy and confused. However, adolescents may not have these symptoms until they are in frank respiratory failure. Physical examination • Findings during a severe episode include the following: • Respiratory rate is often greater than 30 breaths per minute • Accessory muscles of respiration are usually used • Suprasternal retractions are commonly present • The heart rate is greater than 120 beats per minute • Loud biphasic (expiratory and inspiratory) wheezing can be heard • Pulsus paradoxus is often present (20-40 mm Hg) • Oxyhemoglobin saturation with room air is less than 91% Physical Examination • Findings in status asthmaticus with imminent respiratory arrest include the following: • Paradoxical thoracoabdominal movement occurs • Wheezing may be absent (in patients with the most severe airway obstruction) • Severe hypoxemia may manifest as bradycardia • Pulsus paradoxus may disappear: This finding suggests respiratory muscle fatigue Diagnosis • Tests used in the diagnosis of asthma include the following: • Pulmonary function tests: Spirometry and plethysmography • Exercise challenge: Involves baseline spirometry followed by exercise on a treadmill or bicycle to a heart rate greater than 60% of the predicted maximum, with monitoring of the electrocardiogram and oxyhemoglobin saturation • Fraction of exhaled nitric oxide (FeNO) testing: Noninvasive marker of airway inflammation • Radiography: Reveals hyperinflation and increased bronchial markings; radiography may also show evidence of parenchymal disease, atelectasis, pneumonia, congenital anomaly, or a foreign body • Allergy testing: Can identify allergic factors that may significantly contribute to asthma • Histologic evaluation of the airways: Typically reveal infiltration with inflammatory cells, narrowing of airway lumina, bronchial and bronchiolar epithelial denudation, and mucus plugs Management • Guidelines from the National Asthma Education and Prevention Program emphasize the following components of asthma care: • Assessment and monitoring: In order to assess asthma control and adjust therapy, impairment and risk must be assessed; because asthma varies over time, follow-up every 2-6 weeks is initially necessary (when gaining control of the disease), and then every 1-6 months thereafter • Education: Self-management education should focus on teaching patients the importance of recognizing their own level of control and signs of progressively worsening asthma symptoms; educational strategies should also focus on environmental control and avoidance strategies, as well as on medication use and adherence (eg, correct inhaler techniques and use of other devices) • Control of environmental factors and comorbid conditions • Pharmacologic treatment • Pharmacologic treatment Assesment • Pharmacologic asthma management includes the use of agents for control and agents for relief. Control agents include the following: • Inhaled corticosteroids • Inhaled cromolyn or nedocromil • Long-acting bronchodilators • Theophylline • Leukotriene modifiers • Anti-immunoglobulin E (IgE) antibodies (omalizumab) • Relief medications include the following: • Short-acting bronchodilators • Systemic corticosteroids • Ipratropium Respiratory insufficiency • Process of breathing consists of four stages (I – external, pulmonary respiration, II-IV — internal) • I stage. External respiration is the passage of air through the respiratory ways from the nose up to the alveoli and the process of gas exchange between the environment and the lungs. External respiration has two functions — enrichment of blood with oxygen (arterialization) and the removal of carbon dioxide, • II stage. Transport of oxygen from the lungs to the tissues. • III stage. Tissue respiration — in microcirculatory vessels oxygen is given to the tissues • IV stage. Transport of carbon dioxide from the tissues to the lungs. • Respiratory insufficiency (RI) — it is an insufficiency of the function of external respiration which leads to hypoxemia— insufficient quantity of oxygen in the arterial blood. Thus, respiratory insufficiency is a condition during which normal level of oxygen is not maintained in the blood. RI can develop in many diseases of the respiratory system (example, laryngitis, bronchitis, pneumonia, asthma, etc.) and is seen as a complication of the main disease. Stages of respiratory insufficiency Basic clinical signs Participation of accessory muscles in Color of skin respiration Stage of RI Respiratory rate I Insignificant signs appear only after physical work (slight tachypnea without the participation of accessory muscles, pallor, BP normal or moderately raised, heart rate:respiratory rate = 3.0-2.5 : 1). At rest there are no changes + On 25-50 % > > normal 2-1.5: 1 Acrocyanosis, normal perioral, periorbital cyanosis < normal Various ++ or (-) General > 50 % of cyanosis, marnormal, pathmorated skin ological types of respiration II III Blood Heart rate: pressure BR General reaction Sweat secretion Oxygen saturation of blood 90-100% Placid Is increased 70-90% Consciousness is suppressed, seizures Sticky sweat < 70% • As a result of hypoxemia, hypoxia develops — insufficient quantity of oxygen in the body. • However do not overlook other reasons of hypoxia: • Anemic hypoxia — insufficient quantity of hemoglobin in the blood. • Circulatory hypoxia — in arterial blood there is enough oxygen, but its distribution to the tissues is slowed and in insufficient quantity. • Tissue hypoxia — there is the required quantity of oxygen in the blood and its movement in blood is not impaired, but the tissues are not capable of using it fully (this frequently develops due to metabolism disorders). • Respiratory insufficiency is a frequent complication of respiratory diseases. Depending on the clinical signs, three stages of RI are differentiated Respiratory distress syndrome • Respiratory distress syndrome, also known as hyaline membrane disease, occurs almost exclusively in premature infants. The incidence and severity of respiratory distress syndrome are related inversely to the gestational age of the newborn infant. (See Etiology and Epidemiology.) • Enormous strides have been made in understanding the pathophysiology and management of respiratory distress syndrome, leading to improvements in morbidity and mortality in infants with the condition. Advances include the following (see Treatment and Medication): • The use of antenatal steroids to enhance pulmonary maturity • Appropriate resuscitation facilitated by placental transfusion and immediate use of continuous positive airway pressure (CPAP) for alveolar recruitment Respiratory distress syndrome • Early administration of surfactant • The use of gentler modes of ventilation, including early use of "bubble" nasal CPAP to minimize damage to the immature lungs • Supportive therapies, such as the diagnosis and management of patent ductus arteriosus (PDA), fluid and electrolyte management, trophic feeding and nutrition, and the use of prophylactic fluconazole • These therapies have also resulted in the survival of extremely premature infants, some of who continue to be ill with complications of prematurity. (See the image below.) • Chest radiographs in a premature infant with respiratory distress syndrome before and after surfactant treatment. Left: Initial radiograph shows poor lung expansion, air bronchogram, and reticular granular appearance. Right: Repeat chest radiograph obtained when the neonate is aged 3 hours and after surfactant therapy demonstrates marked improvement. Complications • Although reduced, the incidence and severity of complications of respiratory distress syndrome can result in clinically significant morbidities. Sequelae of respiratory distress syndrome include the following (see Prognosis, Clinical, and Workup): • Septicemia • Bronchopulmonary dysplasia (BPD) • Patent ductus arteriosus (PDA) • Pulmonary hemorrhage • Apnea/bradycardia • Necrotizing enterocolitis (NEC) Complications • • • • • Retinopathy of prematurity (ROP) Hypertension Failure to thrive Intraventricular hemorrhage (IVH) Periventricular leukomalacia (PVL) - With associated neurodevelopmental and audiovisual handicaps • Strategic goals include focusing direct attention on anticipating and minimizing these complications and preventing premature delivery whenever possible. • Schematic outlines the pathology of respiratory distress syndrome (RDS). Infants may recover completely or develop chronic lung damage, resulting in bronchopulmonary dysplasia (BPD). FiO2 = fraction of inspired oxygen; HMD = hyaline membrane disease; V/Q = ventilation perfusion References • A) Basic • 1. Manual of Propaedeutic Pediatrics / S.O. Nykytyuk, N.I. Balatska, N.B. Galyash, N.O. Lishchenko, O.Y. Nykyt yuk – Ternopil: TSMU, 2005. – 468 pp. • 2. Kapitan T. Propaedeutics of children’s diseases and nursing of the child : [Textbook for students of higher medical educational institutions] ; Fourth edition, updated and • Translated in English / T. Kapitan – Vinnitsa: The State Cartographical Factory, 2010. – 808 pp. • 3. Nelson Textbook of Pediatrics /edited by Richard E. Behrman, Robert M. Kliegman; senior editor, Waldo E. Nelson – 19th ed. – W.B.Saunders Company, 2011. – 2680 p. • B) Additional • 1. www.bookfinder.com/author/american-academy-of-pediatrics • 2. www.emedicine.medscape.com • 3. http://www.nlm.nih.gov/medlineplus/medlineplus.html • 4. http://intranet.tdmu.edu.ua/data/kafedra/internal/pediatria2/lectures_stud/en/med/lik/ptn/Propaedeutic %20pediatrics/3/08%20SEMIOTICS%20OF%20THE%20RESPIRATORY%20SYSTEM%20DISEASES.htm