Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
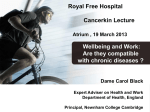
Psychological Considerations in Pain Supraspinal Pain Modulation and Implications for Optimal Treatment of the Patient in Pain Amy E. Williams, PhD* Assistant Professor Director of Riley Pain Center Clinical Director of Psychiatry Consultation Liaison Service at Riley Hospital for Children Department of Psychiatry – Riley Child and Adolescent Psychiatry Clinic Indiana University School of Medicine – Indiana University Health Physicians 705 Riley Hospital Drive, Suite 4300 1 Indianapolis, IN 46202 *No Disclosures The Pain Experience • Pain Scale – YouTube • Pain – Subjective experience • Nociception – Nerve transmission • Nociceptors http://www.cerebromente.org.br/n16/history/mind-history_i.html Modulation of Pain Cognition, Attention, Emotion, Coping Inhibitory Processes Facilitation Processes Exercise Sunburn PAIN Noxious Input 3 Physiological pathway for supraspinal influences on pain 1. Psychological variables (Emotion, Attention, Cognition, Coping) 2. PAG -> RVM -> Dorsal Horn Conditioned Pain Modulation (Diffuse Noxious Inhibitory Controls) • Noxious stimulus -> ventrolateral quadrant of spinal cord -> Subnucleus Reticularis Dorsalis-> Dorsal Lateral Funiculus -> Dorsal Horn 4 Conditioned Pain Modulation + 5 CPM in 7-12 year-old girls with IBS n = 21 n = 22 6 PSYCHOLOGICAL FACTORS Emotion Pain Report Nociceptive Blink Reflex Depressed mood Anxiety Somatization Fear Anger/Frustration 9 Operant Conditioning Behavior Consequence Take tylenol for a headache headache goes away Outcome more likely to take tylenol Add Something Remove Something Increase Behavior + reinforcement - reinforcement Decrease Behavior + punishment - punishment 10 Operant Conditioning Behavior Consequence Outcome Positive Reinforcement • Social attention Pain Behavior Well Behavior Negative Reinforcement (escape/avoidance conditioning) • Temporary reduction in pain • Avoidance of dis-liked tasks or situations (like school, chores, work) • Temporary reduction in worry (after seeking reassurance from physician) Increased Pain and Pain Behaviors Positive Punishment • Increased pain • Social ridicule • Interpersonal stress Negative Punishment • Loss of social attention • Loss of resources (disability) 11 Catastrophizing Children who catastrophize have more pain disability In children who catastrophize, parents can help reduce their pain disability by promoting coping 12 Vervoort, T. T., Huguet, A. A., Verhoeven, K. K., & Goubert, L. L. (2011). Mothers’ and fathers’ responses to their child’s pain moderate the relationship between the child’s pain catastrophizing and disability. Pain, 152(4), 786-793. Reinforcement: Caregiver Empathy • Responding with reassurance, apologies, and empathy actually increases pain – Tells patient that caregiver is worried – Reinforces pain behavior by temporarily reducing distress – Gives permission to express distress – which increases their experience of pain 13 Distraction Distraction • • Walker, LS, Williams, SE, Smith, CA, Garber, J, Van Slyke, DA. (2006). Parent attention versus distraction: Impact on symptom complaints by children with and without chronic functional abdominal pain. Pain, 122(1-2), 43-52. repetitive, pleasant, engaging Anterior Cingulate Cortex 14 Physiological Arousal • Hypothalamus – ANS Pain During Relaxed Breathing Park E, Oh H, Kim T. (2013). The effects of relaxation breathing on procedural pain and anxiety during burn care. Burns 39: 1101-1106. 15 Sleep Psychological and behavioral factors can lead to sleep deprivation Sleep deprivation Increased pain – Impaired pain inhibitory processes? – Mediated by prostaglandins? Positively associated with symptoms and functioning 16 17 What does this have to do with my patients? Psychological Conceptualization of the patient in pain 18 Conceptualization • Patients do have pain – They are not faking and it is not “all in their head” But… • Psychosocial factors can alter pain perception, disability, and medical treatment effectiveness – accounted for 59% of variance in disability following low back injury 19 Conceptualization: Pain and Disability • Improved pain ≠ improved functioning – Pain intensity does not predict physical activity – Psychosocial job factors predict return to work independent of injury severity – Weak relationship between decreased pain and increased functioning or return to work Patients need to return to activities before pain is gone and may require directed intervention to return to previous activities even after pain is gone --Athlete recovering from injury – rehabilitation approach 20 Conceptualization: Acute vs. Chronic Pain • Acute Pain – Adaptive Response • Withdraw and protect from injury • Rest & avoid things that can exacerbate pain • Parental attention & accommodation 21 Conceptualization: Acute vs. Chronic Pain • Chronic Pain – Adaptive response • • • • Acceptance of pain presence Maintain normal activities Active pain coping strategies Reduce factors that exacerbate long-term pain • Manage pain exacerbations 22 Conceptualization Patient Mindset – Acute pain vs chronic pain mindset – Identification with illness Exacerbating Factors – Behaviors/cognitions that enhance or maintain pain and disability – Negative emotional states that contribute to pain – Quality and quantity of sleep Functioning & Disability – General functioning – Work/school – Adherence to medical recommendations Pain Management Strategies – Active vs. passive coping strategies 23 STRATEGIES WITHIN THE PHYSICIAN OFFICE Acknowledge Symptoms and Promote Coping • Some empathy is good – Reflect the patients concerns • “Sounds like this has been really difficult for you.” • “Your pain is really interfering with your job lately.” • Switch to focus on functioning – “let’s work on developing a plan so you can get back to enjoying your life.” – “Sounds like you would like to be able to play tennis again. I would like to help you with that goal.” Teach the Mind-Body Connection • Chronic Pain is a nerve mis-fire or faulty signal • Many factors contribute to pain – Effective treatment involves multiple approaches Manage Reassurance-Seeking • Excessive reassurance can increase symptoms – Have regular scheduled visits rather than frequent emergency calls/visits – Avoid un-necessary tests – Provide an explanation for symptoms • Negative test results rule out specific conditions and point us towards a functional problem rather than a structural problem – Recognize catastrophizing and somatization and help them reframe • Or refer for psychotherapy Focus on Functioning • Minimize your inquiries about pain – Instead inquire about functioning • Help caregivers to reduce inquiries about pain • Promote rehabilitation model – Functioning is not a direct result of pain level – Pain tends to get better after your functioning improves – If we wait until our pain gets better to function we usually only get worse • Set functional goals – “After last session you were able to walk for 10 minutes each day. I recommend we increase that a little this week. How many minutes do you think we should set as your goal this week?” Provide a Pain Plan • Can prevent/reduce – Frequent phone calls or last-minute appointments – Frequent use of or over-reliance on pain medications – Urgent care or ED visits for acute exacerbations • Algorithm for responding to pain – Step-wise instructions – Ex., stretching, gentle exercise, heat/cold, distraction/pleasant activities, relaxation, medications, call doctor When to Refer for Psychotherapy Comorbid mental illness Functional interference Exacerbated by psychosocial factors Medical interventions are not providing expected benefits Seeking miracle cure Strong personal identification with illness Non-adherence to physician recommendations Assess for barriers to medical/surgical outcomes – Before escalating treatment – Not seeing expected improvement 30 Does CBT Really Help? • Grey matter changes after CBT for chronic pain – Increased bilateral dorsolateral prefrontal, posterior parietal, subgenual anterior cingulate/orbitofrontal, and sensorimotor cortices, hippocampus, – Reduced supplementary motor area • Decreased pain catastrophizing associated with – increased left dorsolateral prefrontal and ventrolateral prefrontal cortices, right posterior parietal cortex, somatosensory cortex, and pregenual anterior cingulate cortex 31 ACUTE/PROCEDURAL PAIN Early Pain Experiences • Management of procedural pain in infancy childhood is crucial • Frequent painful procedures in infancy/childhood associated with changes in somatosensory processing related to pain – More pain in future • How to manage infant pain during injections – The Power of a Parent's Touch 33 Needle Pain • Needle phobias develop around 4-5 years of age after negative needle experience – # of injections predictive of phobia – Phobias predict decreased medical treatment seeking throughout life • How to manage needle pain in childhood – It Doesn't Have to Hurt 34 Acute Pain in Adults • Some limited opportunity for control • Relaxation • Distraction – Non-procedural talk • Positive self-statements • Imagery – Pleasant imagery • Avoid empathic statements • Avoid apologies 35 References Manimala, M., Blount, R. L., & Cohen, L. L. (2000). The effects of parental reassurance versus distraction on child distress and coping during immunizations. Children's Health Care, 29(3), 161-177 Vervoort, T. T., Huguet, A. A., Verhoeven, K. K., & Goubert, L. L. (2011). Mothers’ and fathers’ responses to their child’s pain moderate the relationship between the child’s pain catastrophizing and disability. Pain, 152(4), 786-793. Walker, LS, Williams, SE, Smith, CA, Garber, J, Van Slyke, DA. (2006). Parent attention versus distraction: Impact on symptom complaints by children with and without chronic functional abdominal pain. Pain, 122(1-2), 43-52. Schurman, J., Friesen, C., Dai, H., Danda, C., Hyman, P., & Cocjin, J. (2012). Sleep problems and functional disability in children with functional gastrointestinal disorders: an examination of the potential mediating effects of physical and emotional symptoms. BMC Gastroenterology, 12142. doi:10.1186/1471-230X-12-142 Williams, A.E., Heitkemper, M., Self, M.M., Czyzewski, D.I, & Shulman, R. (2013). Endogenous Inhibition of Somatic Pain is Impaired in Girls with Irritable Bowel Syndrome Compared with Healthy Girls. Journal of Pain. 14(9):921-930. Williams, A.E., & Rhudy, J.L. (2009). Supraspinal modulation of trigeminal nociception and pain. Headache, 49(5), 704-720. Park E, Oh H, Kim T. (2013). The effects of relaxation breathing on procedural pain and anxiety during burn care. Burns 39: 1101-1106. Fields HL, Basbaum AI, Heinricher MM: Central nervous system mechanisms of pain modulation, in McMahon SB, Koltzenburg M (eds): Textbook of Pain. Philadelphia, PA, Elsevier/Churchill Livingstone, 2006, pp 125-142 Mallorquí-Bagué N, Bulbena A, Pailhez G, Garfinkel SN, & Critchley HD. Mind-Body Interactions in Anxiety and Somatic Symptoms. Harv Rev Psychiatry. 2016, 24(1): 53-60. doi: 10.1097/HRP.0000000000000085. Campbell C, Edwards R. Mind-body interactions in pain: the neurophysiology of anxious and catastrophic pain-related thoughts. Translational Research: The Journal Of Laboratory And Clinical Medicine [serial online]. March 2009;153(3):97-101. Available from: MEDLINE, Ipswich, MA. Accessed January 24, 2016. Coakley R, Schechter N. Chronic pain is like… The clinical use of analogy and metaphor in the treatment of chronic pain in children. Pediatric Pain Letter 2013;15(1): 1-8. www.childpain.org/ppl Hermann, C., Hohmeister, J., Demirakça, S., Zohsel, K., & Flor, H. (2006). Long-term alteration of pain sensitivity in school-aged children with early pain experiences. Pain, 125(3), 278-285. Lang, P.J., Bradley, M.M., & Cuthbert, B. (2005). The International Affective Picture System (IAPS): Affective ratings of pictures and instruction manual. Technical Report A-6. Levy, RL. (2011). Exploring the intergenerational Transmission of Illness Behavior: From observations to experimental intervention. Annals of Behavioral Medicine 41: 174-182 Seminowicz, D. A., Shpaner, M., Keaser, M. L., Krauthamer, G. M., Mantegna, J., Dumas, J. A., & ... Naylor, M. R. (2013). Cognitive-behavioral therapy increases prefrontal cortex gray matter in patients with chronic pain. The Journal Of Pain, 14(12), 1573-1584. Turk, D. C., & Gatchel, R. J. (2002). Psychological approaches to pain management: A practitioner's handbook (2nd ed.). New York, NY, US: Guilford Press. Walker, S.M., Franck, L.S., Fitzgerald, M., Myles, J., Stocks, J., & Marlow, N. (2009). Long-term impact of neonatal intensive care and surgery on somatosensory perception in children born extremely preterm. Pain, 141(1–2), 79-87. Wollgarten-Hadamek, I., Hohmeister, J., Demirakça, S., Zohsel, K., Flor ,H., & Hermann, C. (2009). Do burn injuries during infancy affect pain and sensory sensitivity in later childhood?. Pain, 141(1-2):165-172 https://www.youtube.com/watch?v=dH4HiSQd3bE#t=57 https://www.youtube.com/watch?feature=player_embedded&v=KgBwVSYqfps https://www.youtube.com/watch?v=3nqN9c3FWn8&feature=player_embedded