Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
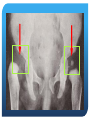
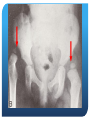
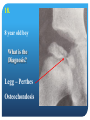
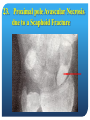
LMCC Orthopedic Review Lecture “Back to Basics” April, 2012 Dr. P.R. Thurston LMCC Orthopedic Review Lecture There are 10 basic topics about which questions may be framed for medical student examinations in Orthopedics. 1) 2) 3) 4) 5) 6) 7) 8) 9) 10) Fractures. Low Back Pain. Child, Painless Limp. Pulmonary Fat Embolus. Compartment Syndrome. Metabolic Bone Disease. Metastatic Disease. Septic Hip / Osteomyelitis – Children. Dislocations. Trivia. Definitions Fracture:A discontinuity in the structural integrity of a bone. Infraction:- An incomplete fracture. Dislocation:Complete loss of contact of the articular surfaces of a Subluxation:- Non-concentric joint surfaces. Reduction:Returning a fracture or dislocation to an anatomical alignment. Comminution:- Multiple fragments. joint. Fractures Definition :- A discontinuity in the structural integrity of a bone. A fracture occurs because the force applied exceeds the breaking strength of the bone so that the Load can no longer be transferred across that zone of the bone. Fractures Mechanical Properties of Bone Bone is a two-phase material :- Calcium HydroxyApatite Osteoid Ca10(PO4)6(OH)2 = mineral Collagen type I and II = fibrous Calcium is strong in compression, but weak in tension. Osteoid is strong in tension, but weak in compression. Fractures (for adult bone) BUT :- Calcium is stronger in compression than Osteoid is in tension And therefore :- Bone always fails first in tension Fractures A bone consists of three areas :- Each region has its own fracture characteristics. the Diaphysis the Metaphysis the Epiphysis. Fractures Diaphyseal Bending Torque Oblique Spiral Direct Metaphyseal Traction Transverse Compression Epiphyseal Intra-articular Pediatric Mixed Fracture Description This fracture is angulated laterally, since it points laterally. The distal fragment is tilted medially Fracture Description 1) The distal fragment is always described with relation to the proximal segment. 2) Displacement = Translation of bone ends. 3) Angulation = Orientation of bone ends. 4) Angulation identifies to where the fracture points. 5) For clarity, the tilt of the distal fragment is often used to describe angulation. Fractures A fracture can occur in :Growing Bone. = Pediatric Deformities. Normal bone subject to abnormal forces. = Traumatic Fractures. Abnormal bone subject to normal forces. = Pathologic Fractures. Normal bone subject to cyclic forces. = Fatigue or Stress Fractures. Fractures I IV Salter-Harris Classification II III V Fractures Salter-Harris Classification 1) Fractures interfering with growing bones. 2) Worse prognosis with increasing number. 3) Probability of surgery increases with number. Stress or Fatigue Fractures Repeated loading below acute failure threshold. Eventual fatigue failure. Military recruits, runners, aerobics. Tibia, metatarsals, femoral neck. Initial x-ray can be negative. Bone tenderness – Bone scan. Pathologic Fractures Failure through abnormally weakened bone Minimal trauma – BEWARE Osteoporosis Metastasis Tumours:- Benign, Malignant (Multiple Myeloma). Metabolic Bone Disease Pathologic Fractures Metastases: Lytic Sclerotic - Lung - Colon - Thyroid - Renal - Breast - Prostate Pathologic Fractures Metastases: - require fixation to prevent fracture if they are > 1/3. - produce pain on weight bearing in the lower limb. - survival > 3 months. - cannot be managed by medical therapy. - radiotherapy after fixation (2 weeks) (radiotherapy induced osteonecrotic fractures) Pathologic Fractures Osteitis Deformans / Paget’s Disease 4% of pop. Over 40 yrs. accelerated bone turnover often assymptomatic monostotic > polyostotic loss of stature AV shunting pathologic bone Gout Urate crystalopathic arthritis Crystals in periarticular tissues Inconsistant elevated serum urate Allopurinol and colchicine Tophi in periarticular soft tissues Deposits in non-articular cartilage Juxta-articular erosions Indications for Closed Reduction There is significant displacement. Reduction is possible. The reduction, if gained, can be held. The fracture has not been produced by a traction force. Indications for Open Reduction 1) 2) 3) 4) 5) 6) 7) 8) There is a significant Displacement. Open Fractures. Intra-articular Fractures. Un-reducible Fractures Reductions that cannot be maintained in a cast. Comminuted or Segmental Fractures. Floating Joints. Fractures with Neurovascular damage. Open Fractures Classification :1. < 1 cm., inside-out, little soft tissue damage. = low potential for infection. 2. 1 cm. – 10 cms., outside-in, requires debridement, but no flap or skin graft. = moderate potential for infection. 3. > 10 cms., outside-in, high energy, devitalized muscle, comminution or bone loss, soft tissue loss. Open Fractures Classification :3A. No loss of soft tissue cover, no flap required. 3B. Flap required due to soft tissue stripping. 3C. Associated vascular injury. Type 1. Open Fracture = 6 mm, extend & debride Degloving Mechanism Degloving Mechanism Type III C Injuries – Vascular Injury Note pallor of the ankle No pulses Fracture Complications 1. Pulmonary Fat Emboli 2. Compartment Syndromes Pulmonary Fat Emboli :- A.R.D.S. - Long bone fractures, burns, contusions. - Interstitial pneumonitis due to free fatty acids - S.O.B. & confusion in young adults. - Axillary & Subconjunctival Petechiae. - Serum lipase elevated. - pAO2 reduced – if < 50 – 20% mortality. - Ventillatory support - Dexamethazone. - 5 day course. Pulmonary Fat Emboli :- A.R.D.S. Since Pulmonary Fat Emboli occur as an on-going process, involving either repeated showers of emboli or an evolution of insults, the most effective treatment is:- Early Fracture Fixation for both prevention and management. Compartment Syndromes - increased interstitial tissue pressure. - fractures, burns, tight dressings. - normal pressure < 25 mm. Hg. - when the tissue pressure > venous capillary pressure, but less than the arteriolar pressure. - 6 P’s - pain. - pallor. - pulselessness. - paresthesias. - paralysis. - poikylothermia. Compartment Syndrome Symptom: Pain out of proportion to that expected for the injury. Signs: 1. Loss of function of muscle due to ischemia within the compartment. 2. Pain with passive stretch 3. Numbness etc. are LATE findings! 4. If neuro symptoms present, potential for full neuro recovery is only 10 %. Rx Compartment Syndrome Release all compressive dressings / plaster. Elevate extremity to heart level. Fasciotomies. 4 compartment fasciotomy Compartment Syndrome Careful monitoring. Recognise it - 5 P’s Call Orthopaedic Surgeon Pressure measurements Back Pain Classification of MechanicalBack Pain Postural syndrome (MacKenzie) normal tissues become painful by the application of prolonged stresses (sitting, bending etc) Dysfunction syndrome soft tissues are shortened and stiff. Usually >30 year old, poor posture, under exercised, reduced mobility Derangement syndrome Disc derangement (tears and herniation) Causes and Classification of Back Pain: McNab Viscerogenic Vasculogenic Neurogenic Psychogenic Spondylogenic Spondylogenic Osseus: Trauma Infection Neoplasms Inflammatory Metabolic (eg.Pagets) Deformities Soft tissues: Muscles SI joints Disc Facets Anatomy Extension Flexion Three joint complex (Kirkaldy Willis) Recurrent rotational strain Synovial reaction facet joint Disc circumferencial tears Cartilage destruction Osteophyte formation radial tear Disc herniation Capsular laxity Instability Internal disc disruption Subluxation Lateral N. Ent decrease disc height Enlargement of articular process Central Stenosis osteophytes Non operative Treatment of Back Pain Do nothing Activity modification Medications Exercise and physiotherapy Braces Manipulation Massage therapy Traction/inversion therapy Vitamins/Supplements/Diets Weight control Disc herniation Ms J.H. 25 y.o. female presented with cauda equina syndrome Cauda Equina Syndrome Sciatica associated with bowel or bladder dysfunction. Perineal numbness. Low or Sequestrated Lumbar Disc. Pressure on S1, S2 and/or S3 nerve roots. Requires immediate Decompression to avoid permanent disability. Spinal stenosis Symptoms: unilateral radicular pain bilateral claudication better with forward flexion of trunk better walking uphill rare bowel/bladder involvement Signs: usually no neuro signs look for pulses stress test Investigations: XR CT Myelo-CT MRI Developmental Dysplasia of the Hip An in utero Anterior Subluxation of the hip. Growth in this position produces excessive Anteversion / Adduction. Classification: Positional 2/1000 Hereditary 2 x more likely if mother Teratologic Arthrogryphosis 50% bilateral, F > M 8:1 Test ALL newborns at birth Conservative Rx at birth – Pavlik, D.diaper Surgical Rx if resistant Legg-Perthe’s Disease Osteochondrosis (avascular necrosis) Proximal Femoral Epiphysis Necrosis, revascularization, fragmentation, healing 3 – 11 yrs., M > F 4:1, 15% bilat. Subluxation laterally, Coxa plana, Coxa magna Osteoarthritis 50 yrs. Slipped Capital Femoral Epiphysis Weakness of the physis of the femoral head allows medial and inferior slip during the last phase of growth. Shortening of the leg, adduction, painless limp and external rotation contracture. Observation if mild, fixation if severe Surgery risks Avascular Necrosis of femoral head Ages for Hip Disease D.D.H. Septic Hip Legg-Perthes Transient Synovitis S.C.F.E. Birth Birth – 11 3 – 11 3 – 11 11 - 16 Osteomyelitis Acute infection, metaphyseal 90% Staph., 20% mortality 100% growth abnormality Periosteal elevation, osteolysis Sequestrum, Involucrum Dislocations The articular surfaces are no longer in contact. Commonly affects Shoulders > PIP joints > Elbows > Ankles. Often associated with fractures. Occasionally associated with neurologic injuries Shoulder Dislocations 95 % anterior 1 % posterior Luxatio erecta Medial Axillary nerve injury Rapid reduction Shoulder Dislocations Conscious sedation. Traction reduction. Immobilization. Recurrent. Voluntary Habitual. Multiaxial instability. Elbow Dislocation Posterolateral. Median nerve injury. Ulnar nerve injury. Rapid reduction. Early mobilization. Time for a 10 minute break! 1. Talipes Equinovarus is the proper name for :- a. b. c. d. e. Flat feet In-toeing Club feet Knock knees Wry neck Pes Planus Metatarsus Adductus Genu Valgus Torticolis Talipes Equinovarus congenital deformity of the foot Equinus, Inversion, Adduction, Supination 2 per 1000 live births 50% bilateral M >F 2:1 Serial corrective casts at birth Surgery if resistant EARLY TREATMENT IS ESSENTIAL 2. A Trendelenburg sign refers to :- a. b. c. d. e. f. Leg length discrepancy Gait abnormality Knee recurvatum Scoliosis Hip Contracture Abductor weakness Trendelenberg Gait 3. All of these are signs of D.D.H. except :- a. b. c. d. e. Limited Abduction Ortolani Sign Asymmetric Skin Folds Galeazzi’s Sign McMurray Sign Knee Meniscal Tear Ortolani, Barlow & Galeazzi Signs 4. a. b. c. d. e. The most common congenital spinal abnormality is :- Scoliosis Spina Bifida Torticolis Klippel – Feil Syndrome Multiple Hereditary Osteochondroma Spinal Bifida defect of neural tube closure Lumbar spine, commonly low 2 per 1000 myelodysplasia Mild to complete paraplegia Occulta, meningocoele, Myelomeningocoele Bowel and bladder dysfunction 5. ? 5. Polydactyly 6. ? 6. Syndactyly 7. ? 7. Sprengel’s Deformity Omovertebral Bone 8. A 6 year old boy with delayed physical development, convulsions, tetany, weakness, blue sclera and bony deformities is most likely suffering from :- a. b. c. d. e. Physical Abuse Ehlers – Danlos Syndrome Osteogenesis Imperfecta Multiple Hereditary Exostoses Myositis Ossificans 9. A 6 year old boy with delayed physical development, a rachitic rosary, weakness and bony deformities is most likely suffering from :a. b. c. d. e. Physical Abuse Rickets Scurvy Osteitis Deformans Myositis Ossificans 9. Rachitic Rosary 9. Delayed Ossification 10. This is :a. Osteomyelitis b. Osteomalacia c. Osteoporosis d. Osteitis Deformans e. Leprosy 11. A child with knee pain has a ____ problem until proven otherwise. a. b. c. d. e. Knee Femoral Tibial Hip Patella 12. All of the following are part of the differential of hip pain in a 6 year old, except :a. b. c. d. e. Femoral Osteomyelitis Septic Hip Transient Synovitis Legg-Perthes Osteochondritis Slipped Capital Femoral Epiphysis 13. Osteomyelitis in children is produced by what route of infection? a. b. c. d. e. Direct extension from another focus Hematogenous spread Perforating wounds Lymphatic spread Septic hip 14. Paronychia An infection of the base of the nail plate 15. Felon A pulp space infection 16. a. b. c. d. e. All of these are findings of a herniated L5-S1 disc, except :Absent Achilles reflex Lateral foot numbness S1 Nerve Root Sciatica Low back pain Extensor Hallucis Longus weakness L5 nerve root 17. Avascular necrosis of the femoral head is associated with all of the following except :a. b. c. d. e. Steroid use Alcohol Deep sea diving Lipid storage disease Diabetes 18. 8 year old boy What is the Diagnosis? Legg – Perthes Osteochondosis 19. Diagnosis? Gout 20. What is this deformity? A Diner Fork Deformity 21. Probable Diagnosis? A Colles Fracture 21. Colles Fracture 21. Colle’s Fracture distal radial fracture FOOSH occurs at all ages commonly 60 yrs. + osteoporosis intra-articular CR & K-Wires External vs Internal Fixation 22. Diagnosis? :- 22. Diagnosis? :- A Scaphoid Fracture 23. The common complication of this fracture is :- 23. Proximal pole Avascular Necrosis due to a Scaphoid Fracture 24. This is a :- a. Buckle Fracture b. Greenstick Fracture c. Stress Fracture d. Pathologic Fracture e. Growth Arrest line 24. This is a :a. Buckle Fracture b. Greenstick Fracture c. Stress Fracture d. Pathologic Fracture e. Growth Arrest line 25. Is this fracture treated by Closed or Open Reduction? 25. ORIF 25. Fractures of Necessity 26. What is the Diagnosis? 26. Posterolateral Dislocation of the Elbow 26. Reduction by traction. TRACTION 27. What is the Diagnosis? 27. Anterior Dislocation of the Shoulder 27. Reduction by traction Traction 28. This is a :a. Supracondylar # b. Olecranon # c. Dislocation d. Forearm # e. Radial Head # 28. Supracondylar Fracture 29. The complications of a Supracondylar fracture in children include all of the following except :a. Malunion b. Volkmann’s Ischemic Contracture c. Compartment Syndrome d. Cubitus Varus e. Peripheral Nerve Injuries f. Pulmonary Fat Embolus 30. The only sign of a Compartment Syndrome that is always present is :a. Pain b. Pallor c. Pulselessness d. Paresthesias e. Paralysis 31. Compartment pressures indicating the need for fasciotomy :- a. 0 – 15 mms. Hg b. 15 – 25 mms. Hg c. > 25 mms. Hg d. > 50 mms. Hg e. > 75 mms. Hg 32. A 20 yr. old male with a fractured femur has findings of confusion, tachypnea and conjunctival petechia. The most likely diagnosis is :- a. Pneumonia b. Pulmonary Fat Emboli c. Cerebral Contusion d. Cardiac Contusion e. Transient Stress Reaction 35. What fracture is this? A Fracture of the Humerus 35. The commonest complication of this fracture is :- 35. A Radial Nerve Palsy 36. Does this fracture require surgery? Yes, it is a Traction Injury and cannot be reduced and held closed. 37. This patient most likely has a fracture of the ….? Right Hip Fracture External rotation Shortening Flexion A Sub-capital Hip Fracture 38. All of the following are complications of this fracture except :a. Malunion b. Avascular necrosis c. Fat emboli d. Non-union e. Thrombophlebitis 38. Blood Supply of Femoral Head 38. Save Head versus Replacement 38. Subcapital Hip Fractures Properties 1. Avascular Necrosis - 30% 2. Malunion - 30% 3. Non-union - 30% 4. Surgery required 5. Older population 6. Pathologic - Osteoporotic Garden Classification 39. What’s the Diagnosis? 39. Intertrochanteric Hip Fracture 39. Intertrochanteric Fractures Properties 1. Varus deformity 2. Well - Healing 3. Traumatic + Osteoporosis 4. Surgery required 5. Mid-range Age population 40. Surgery or not? Yes, Subluxation of the Talus due to rupture of the Distal Tibio-fibular Syndesmosis. 41. Surgery or not? Yes, Unstable Bimalleolar Ankle Fracture 42. What is the approach to this fracture? 23 y.o. male Basketball injury Open fracture Numbness dorsum of toes 42. Reduce dislocation Sterile dressing Splint extremity Re-check NV status IV Antibiotics Tetanus Surgery 43. A 45 yr. old male, who was previously in good health, has sudden onset of transverse low back pain and right sided sciatica to his foot, after chopping wood at the cottage. Upon arising the following morning, he notices numbness on the outer border of his right foot and some weakness in the right leg. He has no bowel or bladder problems. The most likely diagnosis would be:- Disc. a. Lumbar Muscular Strain. b. Herniated Lumbar Disc. c. Herniated Lumbosacral d. Cauda Equina Syndrome. e. Spinal Stenosis. 44. Your initial approach to this problem would include some or all of the following:a. Bedrest. b. Anti-inflammatories. c. Muscle Relaxants. d. Spinal X-rays. e. Physiotherapy. f. Orthopedic/Neurosurgical referral. g. CT-Myelogram or MRI h. Discectomy 45. During the work-up for this problem, the patient complains that he has unaccountably soiled his underwear, without knowing it. Your response to this would be to:- a. Reassure the patient that this is not serious b. Order an urgent MRI c. Get an urgent referral to Neuro/Orthopedics d. Place the patient on immediate bedrest. 46. Which of the following signs and symptoms are consistent with a torn medial meniscus of the knee:a. Inability to squat b. Pain on descending stairs c. Locking d. Recurrent effusions e. All of the above. 47. A 35 yr. old male falls jogging and sustains an undisplaced lateral malleolar fracture of the ankle. He is treated in a Below-knee Walking cast, but returns to the ER 24 hrs. later complaining of increased, persistent, burning pain at the ankle. Your initial response to this situation would be :- a. Re-X-ray the ankle. b. Remove the cast. c. Measure the compartment pressures. d. Instruct the patient to elevate the limb and prescribe an anti-inflamatory. 48. The most common dislocations of the shoulder are:- a. Medial. b. Posterior. c. Luxatio Erecta. d. Anterior. 49. Metastatic lesions to bone, of the following tumours, usually produce lytic defects except:a. Thyroid. b. Pancreas. c. Prostate. d. Kidney. e. Lung. Th - Tha – That’s all folks!