Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Brain (1985), 108,925-940
PREDICTIVE OCULAR MOTOR CONTROL IN
PARKINSON'S DISEASE
by A. M. BRONSTEIN 1 and c. KENNARD 2
• (From the Department of Neurology, The London Hospital, London El IBB)
SUMMARY
A comparison was made of predictive eye movements of both the saccadic and pursuit ocular motor
systems in parkinsonian patients and aged-matched normal controls. In a predictive task our patients,
who were mildly or moderately affected, showed a reduced tendency to make anticipatory saccades
compared with normal controls. Although there was some impairment of pursuit during a
nonpredictive task as shown by an increased phase lag, a normal amount of improvement took place
with a predictive task. This difference between prediction in the saccadic and pursuit system is possibly
explained by an increased reliance on a visual input by parkinsonian patients which prevents them
making use of verbal instruction to generate anticipatory (eye in advance of target) saccades.
Improvement of pursuit with a predictive target track is possible in such patients since normally in
these circumstances the target is mainly followed rather than anticipated. The metrics of saccadic and
smooth pursuit eye movements (saccadic velocity and pursuit turnover velocity) were normal.
INTRODUCTION
Tracking experiments, a fruitful approach to the study of movement strategies in
Parkinson's disease, typically requires the subject to follow, with their eyes or limb, a
target displayed on a screen which either moves in a regular or an irregular pattern.
In normal subjects target movement in a regular pattern enables predictive tracking
of the eye or limb to take place (Noble et ai, 1955). This requires the formation of a
mental representation of the target path, followed by the design of a motor program
to give a suitable output. As a result of this, the lag and error between the eye or limb
and the target is reduced and the subject's tracking performance is therefore
improved. In some circumstances the eye or limb may actually precede the target. In
several papers, Flowers (1976, 1978a, b) has shown a number of hand-tracking
abnormalities in Parkinson's disease, particularly in those experiments in which a
predictive motor strategy was required. In a subsequent paper, however, Flowers
and Downing (1978) failed to demonstrate a predictive deficiency in an ocular motor
(OCM) tracking experiment and, therefore, concluded that only the limbs showed
a predictive abnormality in Parkinson's disease. This seemed to us an unexpected
1
Present Address: M RC Neuro-otology Unit, National Hospital for Nervous Diseases, Queen Square, London,
WC1N 3BG.
2
Correspondence to: Dr C. Kennard, Department of Neurology, The London Hospital, Whitechapel, London
El IBB.
926
A. M. BRONSTEIN AND C. KENNARD
finding since it would imply that the neural organization of predictive movements
for eye and limb functions differently in Parkinson's disease, in contrast to other
clinical conditions. For example, patients with prefrontal lesions exhibit defects in
high level motor programming which are equally present in the OCM and somatic
motor systems (Luria et al., 1966; Guitton et al., 1982). In addition, Flowers and
Downing only examined one aspect of ocular motor behaviour, the smooth pursuit
system. We considered that the saccadic ocular motor system should be assessed
separately because of important functional differences which exist between these
two ocular motor subsystems.
In this paper we report the results of tests of both saccadic and smooth pursuit eye
movements in mild to moderately affected parkinsonian patients compared with
age-matched normal controls. It will be shown that these patients, although having
a relatively normal basic oculomotor performance for their age (for instance,
saccadic velocity and smooth pursuit configuration), displayed abnormalities of
ocular motor prediction similar to those which have previously been reported in the
limbs. A preliminary account has already appeared (Bronstein and Kennard, 1984).
MATERIALS AND METHODS
Clinical Material
Eight patients with idiopathic Parkinson's disease were selected for the study. They were mild to
moderately affected (Hoehn and Yahr, grade I—III) and clinically did not have signs or symptoms of
dementia or coexistent cerebrovascular disease {see Table 1). Their mean age was 65 years (range 53-70
years) as was that of the control group of 8 age-matched normal subjects (range 50-82 years), who were
hospital patients with no neurological abnormality, plus one medical secretary.
Recording Techniques
Eye movements were recorded by the infrared reflection technique (Stark et al., 1962). This system
provided linear recordings over a range ±20 deg with a bandpass of 300 Hz. Head movements were
TABLE
1. C L I N I C A L A S S E S S M E N T OF D I S A B I L I T Y IN T H E P A R K . I N S O N I A N
Subject
1
2
3
4
5
6
7
Sex
M
F
M
M
M
F
M
Age
(yrs)
69
66
61
65
63
69
70
Tremor
Nil
Mild(B)
Nil
Nil
Mild (B)
Severe (U)
Nil
Rigidity
Moderate (B)
Mild(B)
Mild(U)
Moderate (B)
Moderate (B)
Mild (B)
Mild (B)
Bradykinesia
Mild(B)
Mild (B)
Moderate (U)
Moderate (U)
Moderate (B)
Moderate (B)
Mild(B)
8
M
53
Mild (B)
Mild(B)
Moderate (B)
U — unilateral.
B •= bilateral.
Drugs
Nil
Sinemet
Sinemet
Sinemet
Sinemet
Sinemet
Sinemet
Bromocriptine
Madopar
Bromocriptine
GROUP
EYE MOVEMENTS IN PARKINSON'S DISEASE
927
recorded by means of a light helmet, worn by the subject, which was attached to a low torque
potentiometer via a rigid rod. The visual target was a white spot of light (30 min of arc), reflected onto a
curved white screen placed 150 cm away from the subject. Target, eye and head positions were recorded
on paper by an ink-jet recorder (Mingograph), and onto magnetic tape for computer analysis. Gaze
position (eye position in space) was derived off-line by adding eye and head position signals in a
differential amplifier.
Subjects performed saccadic and smooth pursuit experiments in one session. The experiments were
performed with the head motionless and then repeated while the subject was encouraged to move his
head.
Saccadic Experiments
The target moved in a square wave step function across the screen in the horizontal plane in three
different conditions.
Random saccades (RS). The target moved randomly between 9 different positions on the screen
(1 central and 4 on each side) generating 8 possible target amplitudes, 5, 10, 15, 20, 25, 30, 35 and
40 deg. The time interval between target displacements was randomized between 0.6 and 1.2 s. The
subjects were told that the target would jump randomly on the screen and were asked to follow it as
accurately as possible. The test duration was 50 s generating 55 steps.
Hidden predictive saccades (HPS). This protocol consisted of a sequence of 20 regular target
displacements which, without any warning, appeared in the middle of a random sequence. The target
moved symmetrically 30 deg from 15 deg left to 15 deg right and back, with a fixed time interval of 0.9 s.
Test duration and instructions to the subject were identical to RS.
Predictive saccades (PS). This protocol consisted of 33 regular 30 deg target displacements between
15 deg left and 15 deg right, with a fixed time interval of 0.9 s (0.55 Hz). Pilot studies and experiments in
the literature (Stark et al., 1962) have shown that this time interval regularly produces predictive
saccades in normal subjects. The subjects were told in advance that the target, in contrast to the
previous test they had undergone, would move regularly on the screen, jumping between two fixed
points. No instruction as to whether or not they should try to predict or anticipate the target was given.
The duration of this test was 30 s.
For eye-head coordination experiments, time intervals between target displacements were 60 per
cent longer in order to allow complete head stabilization before a new target step took place.
Analysis of results. Eye saccadic velocity was measured with computer software described elsewhere
(Smith et al., 1981) and included all saccades from RS, HPS and PS tests, except those produced in
advance of the target displacement (anticipatory saccades). The computer program generates an
amplitude/peak velocity plot of saccades and fits an exponential curve to the data. The asymptote of
the peak velocity (k) is used to express saccadic velocity.
The latency of saccades produced in RS was measured by the computer. The latency of each saccade
occurring during HPS and PS were determined by hand from the chart recordings since the computer
program would only measure saccades produced after a target displacement had taken place.
Gaze displacement during head movement was measured by the same computer program as
described for eye saccades. In addition, the latencies of head movements occurring during combined
eye-head experiments were measured by computer.
Smooth Pursuit Experiments
The target moved horizontally with a constant peak amplitude of 30 deg, under two different
conditions:
Random smooth pursuit (RSP). The target moved sinusoidally in an unpredictable manner at one of
five different frequencies, 0.08, 0.16, 0.32, 0.48 and 0.65 Hz. One frequency was used for a random
period of between 1.3 and 2.6 s, after which it randomly changed to a different frequency. Two stimulus
sequences of 50 s each were presented. The subjects were instructed to follow the target with their eyes
as accurately as possible and were informed that it would be moving irregularly and at a variable speed.
928
A. M. BRONSTEIN AND C. KENNARD
Predictive smooth pursuit (PSP). Identical target frequencies were then individually presented. Two
sequences of 45 s each were used; the first sequence continued for 22 s at a target frequency of 0.08 Hz
(approximately 2 cycles), and then the second for an identical period at 0.16 Hz (approximately 6
cycles). In the second sequence three 15 s periods, with target frequencies of 0.32 Hz (5 cycles), 0.48 Hz
(8 cycles) and 0.65 Hz (10 cycles), respectively, completed the test. The subjects were informed that the
target would move regularly and the experimenter told them during the sequences when the target
frequency was changed. No instruction was given as to whether or not they should anticipate the
target.
Analysis of results. Phase error of smooth pursuit was measured by hand for two target frequencies,
0.32 and 0.65 Hz. Their zero velocity points (maxima and minima) of both smooth pursuit eye
movement and of target movement were determined in saccade-free regions. The difference between
eye and target position, expressed in degrees, corresponded to the phase error, typically phase lag.
Phase measurements were made for the eye, gaze and head in RSP and PSP. Approximately 7 (range 3
to 15) half cycles were measured for each condition.
Turnover velocity of the smooth pursuit system was measured by computer as described elsewhere
(Bittencourt at ah, 1982). In brief, the program simultaneously measures eye and target velocity and,
by comparing the two, is able to identify whether smooth pursuit eye movements or catch-up saccades
are being used to track the visual target. The data are sampled at 256 Hz and a plot is produced of the
percentage of time spent in actual smooth pursuit during tracking as a function of target velocity.
Normally, as the speed of the target increases, eye tracking becomes more and more saccadic so that
less time is spent in smooth pursuit. The target velocity at which the percentage of time spent in smooth
pursuit drops by 3 dB, is the turnover velocity and provides a measure of the point at which smooth
pursuit breaks down into mainly saccadic tracking. Gaze movements were treated in a similar manner
by computer analysis.
A computer program (BMDP2V) for analysis of variance and covariance with repeated measures
was used for statistical analysis. Comparisons between groups (patients and controls) under different
test conditions (eye-gaze, 0.3-0.6 Hz, random-predictive) were made and interactions between these
various groups and conditions were also available. Other statistical tests used are mentioned in the
Results.
RESULTS
Saccadic Movements
Random saccades. Latencies of saccades were slightly but significantly prolonged
in the parkinsonian patients (F = 6.96, P = 0.02); interaction between eye and gaze
conditions were not significant. The latency of head movements was prolonged
(t = 2.23, P < 0.05; Student's t test). No differences were found in the velocity for
either eye or gaze (Table 2).
TABLE 2. MEAN LATENCY AND PEAK VELOCITY OF SACCADES IN PARKINSONIAN
PATIENTS AND NORMAL CONTROLS
Latency (ms) ± SD
Parkinsonian
Controls
Peak velocity {aegis) ± SD
Eye
Gaze
Head
Eye
Gaze
221 ± 24*
185 ± 2 1
221 ±24*
193 ± 24
328 ± 4 1 *
272 ± 57
612 ±125
645 ±141
563 ± 104
543 ±114
* P < 0.05.
EYE MOVEMENTS IN PARKINSON'S DISEASE
929
Control
Target
20degI
Eye
20deg
Patient
Target
20 deg I
Eye T
20 deg 1
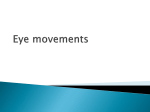
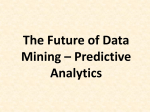
FIG. 1. Saccadic eye movements of a normal control and a parkinsonian patient during the hidden predicUve
sequence. The target made random step displacements until the point marked by the asterisk, when regular
displacement between twofixedpoints commenced. Some predictive saccades occurred in both subjects (arrows)
before or at the time of the target movement. In this and subsequentfiguresupward movements of the target or eye
represents movement to the right.
Control
Patient
Target
30 deg 1
Eye [
30 deg I
-T
'
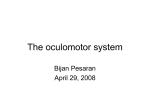
FIG. 2. Saccadic eye movements of a normal control and parkinsonian patient during the predictive sequence.
The asterisk indicates the twenty-fifth target displacement in that run. The normal subject makes entirely
anticipatory saccades (onset before target displacement) which are only irregularly seen in the parkinsonian subject.
In addition, at one point (saccade 24) the patient makes a hypometric multiple-step saccade and then fails to follow
the target for 1 cycle.
Predictive saccades. Figs 1 and 2 show examples from the recordings of a patient
and a normal control during the HPS and PS experiments. During the HPS sequence
(fig. 1), both subjects appear to identify the repetitive pattern and produce a few
predictive saccades. During the PS sequence (fig. 2), in which the subjects had been
told in advance that the target would move regularly between two points, noticeable
differences appeared between the two subjects. The normal subject tended consistently to reduce his saccadic latency or even anticipate the target, whereas the
patient only irregularly made anticipatory saccades. Occasionally, a patient would
'freeze' and miss a couple of target displacements as shown in the figure. Only 2
patients showed this phenomenon, each on one occasion. It is interesting that it only
occurred in the PS run and never in the HPS or RS run, in spite of the fact that RS
sequences were of longer duration and included shorter interstimulus intervals than
PS sequences.
930
A. M. BRONSTEIN AND C. KENNARD
In fig. 3 a plot showing the evolution of mean saccadic latencies for all the subjects
during RS, HPS and PS sequences is presented. The latency is considered positive
when the response follows the stimulus and negative when the response occurs
before the stimulus (anticipation). During the regular target displacements in the
HPS sequence, both groups progressively reduced their latencies. There was a
significant correlation between trial (saccade) number and latency (Kendall
correlation coefficient: controls, r = 0.59, P < 0.01; patients, r = 0.33, P < 0.05).
-200-1
\
-100-
lul
1
+ 100-
8. +200+300Random
Hidden predictive
Predictive
Fio. 3. Sequential analysis of mean saccadic response time (latency) for parkinsonian patients (open circles,
broken line) and normal controls (filled circles, continuous line) in random (RS), hidden predictive (HPS) and
predictive (PS) tests. In the RS the mean latency of patients is slightly prolonged, but during HPS it can be seen that
the latency of both groups gradually shortens with successive cycles. In PS the latency rapidly shortens in both
groups, but whereas normal controls show a plateau mean response time of approximately — 120 ms (anticipatory
saccades), the patients are unable to improve beyond the response time found in HPS. Vertical bars represent
± 1SD.
However, the most prominent differences occur during the PS sequence where
it can be seen that mean latencies are negative (anticipatory) in controls and
positive in patients. There was a significant difference (z = 1.96, P = 0.05 MannWhitney test) between the saccadic mean latencies of patients (107 ± 181 (SD) ms)
and controls ( — 116 + 220 ms) during the PS sequence. During the predictive
sequence in the HPS run the percentage of saccades which are anticipatory is very
similar in both groups (controls: 23%, patients: 22%). During the PS run the
patients marginally increased this value to 29 per cent, in marked contrast to the
controls in whom 60 per cent of saccades became anticipatory; this interaction
between conditions (HPS and PS) and subject groups was statistically significant
(F = 5.62, P = 0.03) (fig. 4).
Smooth Pursuit Movements
Turnover velocity analysis. No significant differences were found between the two
groups (fig. 5). Both groups increased their turnover velocity in the predictive mode
(F = 27.93, P < 0.001). In addition it was found that turnover velocity gaze values
EYE MOVEMENTS IN PARKINSON'S DISEASE
931
70-|
60-
5040-
'M 30-
20-
100J
Hidden
predictive
Predictive
FIG. 4. Histograms to show the percentage of saccades which are
anticipatory (commenced before target displacement) in normal
controls (open areas) and parldnsonian patients (hatched areas)
during the HPS and PS. No difference is shown in the HPS, but
during PS normal subjects considerably increase the percentage of
anticipatory saccades whereas parkinsonian patients do not.
were higher than eye alone (F = 5.00, P = 0.04), but this was made more evident in
the predictive mode (interaction eye-gaze/random-predictive: F = 5.45, P = 0.03).
This improvement in the smooth pursuit turnover velocity during the head-free
condition is thought to be due to an increased efficiency of the catch-up saccades
generated by the latter condition and has been discussed elsewhere (Bronstein and
Kennard, 1984).
Phase lag analysis. Fig. 6 shows a recording from a normal subject and a patient
during random and predictive conditions, in which a few cycles of the target moving
at the highest frequency used are shown. Two particular features may be seen; first,
701
Eye
Gaze
60
50-
f- 40-
li
30Random
Predictive
Random
Predictive
FIG. 5. Mean turnover velocity (deg/s) of eye and gaze (head free) in random and predictive pursuit for patients
(circles) and controls (squares). Vertical bars represent ± 1 SD.
A. M. BRONSTEIN AND C. KENNARD
932
Control
Patient
3Odeg
30deg
30deg
3Odeg
FIG. 6. Examples of eye movements of a normal control and parkinsonian patient during random {upper) and
predictive (lower) smooth pursuit. In each pair of traces the target is above and left eye below. The zero velocity
points of the target (solid vertical line) and eye (interrupted vertical line) are indicated. The difference in position
expressed in deg between the eye and the target indicates the phase error which can be seen to be greater in the
parkinsonian patient than the normal control. The phase error is reduced during predictive pursuit compared with
random pursuit in both subjects.
the morphology of the eye movement in the two subjects is rather similar. Both show
impaired pursuit containing frequent catch-up saccades. Secondly, the main
difference between the two subjects' performance is in the phase error, the patient
showing phase lags approximately double those of the control. In comparison
during the predictive sequence it can be seen that both subjects considerably reduce
their phase lag. During head-free tracking (fig. 7), although head movement itself
was not delayed in relation to the target, gaze still showed an increased phase lag.
The mean and standard deviations of the phase error in these different conditions
are plotted in fig. 8. The statistical analysis was performed for eye and gaze together
and separately for head. The eye and gaze phase lags are significantly larger in the
patients compared to controls (F = 6.99, P = 0.02). Reduction of phase lag in the
predictive condition was statistically significant (F = 45.88, P < 0.001). However,
this reduction was equally evident in the two groups, there being no significant
interaction between the random-predictive conditions and groups. The phase lag
found at the higher frequency are, as expected, significantly greater in both groups
( F = 106.83, P = 0.001).
The phase lag of the head, in contrast to eye and gaze, showed no significant
difference between the two groups. A greater mean phase lag of the head was found
at the higher frequency (F = 33.84, P < 0.001). There was a significant reduction in
phase lag during the predictive sequence (F = 30.02, P < 0.001). This reduction was
present in both groups to the same extent but there was no significant randompredictive group interaction.
EYE MOVEMENTS IN PARKINSON'S DISEASE
933
Is
Target
3Odeg.
Gaze I
30deg|
Eye I
3Odeg|
Head
30 deg|
FIG. 7. The eye, gaze and head movements of a parkinsonian patient during predictive head-free smooth pursuit.
The zero velocity points of the target (solid vertical line) and gaze and head (interrupted vertical line) are indicated.
There is very little phase error of the head which on some occasions is leading (i.e., anticipating) the target, whereas
the gaze still shows a considerable phase lag.
leg
Eye
Gaze
Head
-40
-35
-30
-25
Phase
1
-10
-5
0
+5
H
+ 10
0.3
0.6
0.3
0.6
Target frequency (Hz)
0.3
0.6
FIG. 8. The mean and standard deviation smooth pursuit phase error of eye, gaze and head for parkinsonian
patients (circles) and normal controls (squares) during pursuit of a target of frequency 0.3 and 0.6 Hz. The target
moved in the random (filled symbols) or predictive (open symbols) mode.
DISCUSSION
The main finding of this study of eye movements in Parkinson's disease is that
under certain predictable conditions there is a reduced tendency to make
anticipatory saccades. Surprisingly, however, two earlier studies did not report
934
A. M. BRONSTEIN AND C. KENNARD
abnormalities of prediction in the parkinsonian ocular motor system (Melvill Jones
and Mandl, 1976; Flowers and Downing, 1978). This was taken by Flowers and
Downing to indicate that the organization of motor activities involving predictive
movements may be different for the eye and limbs, each having its own separate
predictor mechanism which is differentially affected by Parkinson's disease. This
apparent contradiction with our results is partly due to the fact that they based their
conclusions solely on smooth pursuit experiments and did not investigate the
saccadic system. We have also found an improvement in predictive smooth pursuit
in parkinsonian patients shown by the reduction in phase lag and increase in
turnover velocity.
It is in the saccadic system that we have shown significant abnormalities in the
predictive capacity of parkinsonian patients. Moreover, the experimental design
permits us to make some observations upon the nature of this predictive defect.
During the hidden predictive saccade sequence both parkinsonian patients and
controls are initially unaware of the regularity of the target trajectory but, as shown
by the reduction in saccadic latency and by the increasing number of anticipatory
saccades, gradually recognize its predictable nature. Despite this, in the predictive
saccade (PS) test, parkinsonian patients, when compared with controls, produced
far fewer anticipatory saccades and did not further reduce their mean saccadic
latency.
Before the PS sequence all the subjects were informed about the regularity of the
target displacement, but special care was taken not to suggest whether they should
anticipate or follow it. Under similar test conditions to the ones we used, normal
subjects were found to have saccadic latencies which were critically influenced by the
type of verbal instruction (Polidora et al., 1957). Those subjects instructed to
'anticipate' had negative (anticipatory) mean latencies of about 100 ms and those
told to 'follow' the target produced their saccades 100 ms after the target jump. In
the absence of any specific instruction given in the PS sequence other than to inform
the subjects about the regularity of the target movement, the trend of our normal
subjects was to anticipate the target to a degree (60% anticipatory) similar to
previously published studies using comparable test conditions (Stark et al., 1962;
Horrocks and Stark, 1964). Parkinsonian patients in our experiments tended to
'follow' the target rather than regularly anticipate it, which probably reflects an
increased dependence on the visual stimulus. Their mean latency values of about
100 ms during PS are compatible with a predictive process in which reaction times
are only reduced to the lower limit. In this situation information contained in the
visual target can still induce modifications in the saccadic response (Horrocks and
Stark, 1964).
Previous work on manual tracking of a continuously moving target has shown
that parkinsonian patients are able to reduce tracking lag when the target path
becomes regular and therefore predictable (Flowers, 1978a; Bloxham et al., 1984;
Day et al., 1984). Experiments which involve discontinuous (i.e., ballistic) limb
movements in tracking a step function target (Flowers, 1976, 1978ft), however,
EYE MOVEMENTS IN PARKINSON'S DISEASE
935
showed a failure of prediction. Similarly, Bloxham et al. (1984) have shown that
parkinsonian patients are unable to make use of advance information in performing
a reaction time test. These findings, as well as the results in our PS experiment,
emphasize the difficulty parkinsonian patients have in making movements of eye or
limb in advance of the visual target. This abnormality reflects an increased reliance
on visual input which has previously been described (Cooke et al, 1978; Flowers,
19786; Stern et al., 1983), and is reminiscent of the much improved locomotor
function which occurs clinically when such patients are provided with a powerful
visual input, for example a striped floor (Martin, 1967).
Two possible pathophysiological explanations for this disturbance of prediction are worthy of consideration. The first arises from the similarity between
parkinsonian patients and patients with frontal lobe lesions who show a difficulty in
utilizing verbal instructions in the construction of motor programs (Luria, 1969).
An example of this in relation to the ocular motor system is shown in experiments on
patients with well-defined surgical lesions in the prefrontal region who, after
relevant verbal instructions, were unable to generate saccades in a direction opposite
to a sudden target displacement (Guitton et al., 1982). These patients therefore
followed the visual stimulus rather than the verbal instruction. Several studies
of cognitive and motor function in Parkinson's disease have already shown
abnormalities similar to those found in patients with frontal lobe lesions (DennyBrown, 1968; Morel-Maroger, 1977; Figini and Bronstein, 1981; Bowen et al,
1972; Lees and Smith, 1983). These frontal lobe type abnormalities found in
Parkinson's disease may be due to dysfunction of the ascending dopaminergic
mesocorticolimbic pathway projecting to the frontal cortex (Javoy-Agid and
Agid, 1980).
A second possible pathophysiological explanation for the failure of our
parkinsonian patients to make anticipatory saccades during the predictive sequence
is to be found in recent experimental studies of cells in the pars reticulata of the
substantia nigra in primates. This may also explain the other saccadic abnormality
we found which was a prolonged latency, previously reported in the ocular
(Shibasaki et al, 1979; Teravainen and Calne, 1980a, b; Shimizu et al, 1981) and
somatic motor systems (Kennard et al, 1982; Evarts et al, 1981). These experiments
have shown a clear relationship between the basal ganglia and the major saccadic
control centres, the frontal eye fields (area 8) (Kunzle and Akert, 1977) and the
superior colliculus (Hikosaka and Wurtz, 1983). The dopaminergic cells in the pars
compacta of the substantia nigra project to the caudate nucleus and putamen
(striatum), which in turn receives a projection from the frontal eye fields,
particularly to the posterior caudate nucleus. One of the two major outputs from the
striatum is to the pars reticulata of the substantia nigra, some of whose cells project
to the intermediate and deep layers of the superior colliculus (Jayaraman et al,
1977). These cells have been found to reduce their discharge rate both in response to
an appropriately located visual target and to a remembered target (Hikosaka and
Wurtz, 1983). Since they appear to be gabaergic inhibitory cells (Vincent et al,
936
A. M. BRONSTEIN AND C. KENNARD
1978), a decrease in discharge rate would reduce tonic inhibition, and hence increase
the excitability of collicular cells. These cells have been found to exhibit a burst of
discharge before saccades of a particular direction and amplitude (Wurtz and
Goldberg, 1972). A disturbance of the dopaminergic input to the corpus striatum, as
occurs in Parkinson's disease, may lead to an abnormal output to the substantia
nigra pars reticulata resulting in reduced facilitation of collicular cells leading to
prolonged latencies. Since the substantia nigra pars reticulata cells also discharge
prior to saccades to a remembered target, an abnormal input to these cells could lead
to an impaired ability to make anticipatory saccades, which are in essence saccades
to a remembered target. It is of interest that DeJong and Melvill Jones (1971)
showed that patients with Parkinson's disease took a longer time than controls
to make saccades back and forth between two targets which are continuously
illuminated. In this case the saccade must be initiated by something other than
the onset of a visual target, again possibly analogous to saccades to remembered
targets.
Examination of the smooth pursuit system in our patients showed an increased
phase lag, a feature previously described for hand tracking experiments in
Parkinson's disease and in monkeys with caudate lesions (Stark, 1968; Bowen, 1969;
Bowen et al., 1975; Flowers, 1978a). Since smooth pursuit operates by continuously
detecting and subsequently correcting retinal error (i.e., a closed-loop system), it
could be argued that a prolonged reaction time at one or more points during the
central processing for such a tracking task may well produce delay (lag) between
target and eye. An interesting finding, however, was that the phase lag of the head
during smooth pursuit was not significantly increased, which indicates its unique
form of motor control. With the head free to move during visual tracking of a target
the only important factor in the maintenance of foveation of the target is the retinal
or gaze error. Indeed changes in head gain or phase can be enormous and yet gaze
gain, phase or accuracy will remain unchanged (Lanman et al., 1978; Collewijn et
al., 1982). This is due to stabilization of the eyes on target by the vestibulo-ocular
reflex despite the variable head error (Lanman et al., 1978). There therefore appears
to be no need for precise detection of head error during head-free smooth pursuit
and this is reflected in its large variance for both groups of subjects shown infig.8.
Although the absolute value of eye-gaze smooth pursuit phase lag was increased
in the parkinsonian patients the percentage of reduction during regular sine wave
tracking was similar in both groups. This is in agreement with previous papers
(Flowers and Downing, 1978; Melvill Jones and Mandl, 1976) where preserved
predictive behaviour in the smooth pursuit system of parkinsonian patients was
found.
This apparent difference in predictive capacity between the saccadic and smooth
pursuit ocular motor systems in parkinsonian patients requires some explanation.
We believe that the normal marked dependence of smooth pursuit on the presence of
a visible moving target is one of the clues to this problem. Target anticipation in
smooth pursuit (i.e., eye in advance of target) occurs only exceptionally, as reflected
EYE MOVEMENTS IN PARKINSON'S DISEASE
937
in the constant delay (lags present between target and eye position), even amongst
normal subjects (fig. 8) (Lisberger et al., 1981). Moreover, it has long been known
that normal smooth pursuit eye movements are exceedingly difficult to generate
except in response to a slowly moving target. If, as we have suggested earlier, the
predictive deficit seen in the saccadic experiments is at least partly due to an
increased reliance on visual input, then we would not expect a similar deficit in the
smooth pursuit system since a predictive response does not involve anticipation to
the same degree as in the saccadic system. The target is constantly present and is
being pursued.
A final point of-interest emerging from our experiments is that, apart from the
'high level' abnormalities of the ocular motor system concerned with prediction, the
metrics of saccadic and smooth pursuit movements were relatively unimpaired. In
the patients studied, saccadic peak velocities were normal and the turnover velocity
of the smooth pursuit system, although marginally reduced, was not significantly
different from the normal controls. This would imply that the peripheral neuromuscular ocular plant, and the brainstem ocular motor nuclear and prenuclear
neurons were functioning normally. This relative normality contrasts with some of
the earlier literature and is due to at least two factors. First, these studies included
severely affected patients (Shibasaki et al., 1979; Corin et al., 1972; Teravainen and
Calne, 1980a, b), some of whom had other associated brain lesions (White et al.,
1983), or patients with undefined disease severity (DeJong and Melvill Jones, 1971;
Melvill Jones and Mandl, 1976; Shibasaki et al., 1979). Secondly, there was
sometimes a disparity between the ages of patients and controls (Shibasaki et al.,
1979; Shimisu et al., 1981). It is now generally agreed that performance of the ocular
motor system, in particular smooth pursuit, is highly dependent upon age (Sharpe
and Sylvester, 1978). Spooner et al. (1980) have recently shown that a group of
patients with vertebrobasilar insufficiency who were administered a battery of eye
movement tests could be considered either as abnormal, if a control group of
unselected age was used, or as normal if compared with an age-matched control
group. Consideration of the literature on ocular motor disturbances in Parkinson's
disease in relation to these points results in the conclusion that mild or moderately
affected patients, suffering only from idiopathic Parkinson's disease and compared
with a properly age-matched control group, show minimally impaired pursuit or
slowed saccades and our results would confirm this view. The possibility that more
severely affected patients could show a more severe degree of impairment obviously
remains, but in our opinion requires further validation.
In conclusion, this study of eye movements in parkinsonian patients has shown
significant abnormalities in the predictive behaviour of the saccadic system which
may relate to dopamine deficiency either in the frontal lobe, or as a result of
abnormal interactions between the basal ganglia and superior colliculus. As similar
disturbances have previously been found in hand tracking experiments, our results
do not support the hypothesis that the eye and limb predictive mechanisms are
differentially affected by the disease.
938
A. M. BRONSTEIN AND C. KENNARD
ACKNOWLEDGEMENTS
We are grateful to Dr I. T. Brown for technical expertise, and to Dr L. Henderson for his helpful
criticism of the manuscript.
This study was partly supported by the Mason Medical Trust and by a fellowship from the Wellcome
Trust to Dr Bronstein.
REFERENCES
BITTENCOURT P
R M,
SMITH A T, LLOYD
DSL,
RICHENS
A (1982) Determination of smooth pursuit
eye movement velocity in humans by computer. Electroencephalography and Clinical Neurophysiology, 54, 399-405.
BLOXHAM C A, MINDEL T A, FRITH C D (1984) Initiation and execution of predictable and
unpredictable movements in Parkinson's disease. Brain, 107, 371-384.
BOWEN F P (1969) Visuomotor deficits produced by cryogenic lesions of the caudate. Neuropsychologia,
7, 59-65.
BOWEN F P, HOEHN M M, YAHR M D (1972) Cerebral dominance in relation to tracking and tapping
performance in patients with parkinsonism. Neurology, Minneapolis, 22, 32-39.
BOWEN F P, KAMTENNY R S, BURNS M M, YAHR M D (1975) Parkinsonism: effects of levodopa on
concept formation. Neurology, Minneapolis, 25, 701-704.
BRONSTEIN A M, KENNARD C (1984) Predictive eye movements in normal subjects and in Parkinson's
disease. In: Theoretical and Applied Aspects of Eye Movement Research. Edited by A. G. Gale and
F. Johnson. Advances in Psychology, Volume 22. Amsterdam: Elsevier, pp. 463-472.
COLLEWUN H, CONUN P, TAMMINGA E P (1982) Eye-head coordination in man during the pursuit of
moving targets. In: Functional Basis of Ocular Motility Disorders. Edited by G. Lennerstrand,
D. S. Zee and E. L. Keller. Oxford: Pergamon, pp. 369-378.
COOKE J D, BROWN J D, BROOKS V B (1978) Increased dependence on visual information for movement
control in patients with Parkinson's disease. Canadian Journal of Neurological Sciences, 5,
413-415.
CORIN M S, ELIZAN T S, BENDER M B (1972) Oculomotor function in patients with Parkinson's disease.
Journal of the Neurological Sciences, 15, 251 -265.
DAY B L, DICK J P R, MARSDEN C D (1984) Patients with Parkinson's disease can employ a predictive
motor strategy. Journal of Neurology, Neurosurgery and Psychiatry, 47, 1299-1306.
DEJONG J D, MELVILL JONES G (1971) Akinesia, hypokinesia, and bradykinesia in the oculomotor
system of patients with Parkinson's disease. Experimental Neurology, 32, 58-68.
DENNY-BROWN D (1968) Clinical symptomatology of diseases of the basal ganglia. In: Handbook of
Clinical Neurology, Volume 6. Edited by P. J. Vinken and G. W. Bruyn. Amsterdam: NorthHolland, pp. 133-172.
EVARTS E V, TERAVAINEN H, CALNE D B (1981) Reaction time in Parkinson's disease. Brain, 104,
167-186.
FIGINI H A, BRONSTEIN A (1981) Algunos aspectos de la psicomotilidad en los sindromes
parkinsonianos. Revista Neurologica Argentina, 7, 55-56.
FLOWERS K A (1976) Visual 'closed-loop' and 'open-loop' characteristics of voluntary movement in
patients with parkinsonism and intention tremor. Brain, 99, 269-310.
FLOWERS K (1978a) Some frequency response characteristics of parkinsonism on pursuit tracking.
Brain, 101, 19-34.
FLOWERS K (19786) Lack of prediction in thef motor behaviour of parkinsonism. Brain, 101, 35-52.
FLOWERS K A, DOWNING A C (1978) Predictive control of eye movements in Parkinson disease. Annals
of Neurology, 4, 63-66.
GurrroN D, BUCHTEL H A, DOUGLAS R M (1982) Disturbances of voluntary saccadic eye movement
EYE MOVEMENTS IN PARKINSON'S DISEASE
939
mechanisms following discrete unilateral frontal lobe removals. In: Functional Basis of Ocular
MolUity Disorders. Edited by G. Lennerstrand, D. S. Zee and E. L. Keller. Oxford: Pergamon,
pp. 497-500.
HIKOSAKA O, WURTZ R H (1983) Visual and oculomotor functions of monkey substantia nigra pars
reticulata. IV. Relation of substantia nigra to superior colliculus. Journal of Neurophysiology, 49,
1285-1301.
HORROCKS A, STARK L (1964) Experiments on error as a function of response time in horizontal eye
movements. MIT Research Laboratory of Electronics Research Report, 72, 267-269.
JAVOY-AGID F, AGID Y (1980) Is the mesocortical dopaminergic system involved in Parkinson disease?
Neurology, New York, 30, 1326-1330.
JAYARAMAN A, BATTON R R, CARPENTER M B (1977) Nigrotectal projections in the monkey: an
autoradiographic study. Brain Research, Amsterdam, 135, 147-152.
KENNARD C, ZANGEMEISTER W H, MELLORS S, STARK L, HOYT W F (1982) Eye-head coordination in
Parkinson's disease. In: Functional Basis of Ocular Motility Disorders. Edited by G. Lennerstrand,
D. S. Zee and E. L. Keller. Oxford: Pergamon, pp. 517-520.
KUNZLE H, AKERT K (1977) Efferent connections of cortical area 8 (frontal eye field) in Macaca
fascicularis: a reinvestigation using the autoradiographic technique. Journal of Comparative
Neurology, 173, 147-164.
LANMAN J, BIZZI E, ALLUM J (1978) The coordination of eye and head movement during smooth
pursuit. Brain Research, Amsterdam, 153, 39-53.
LEES A J, SMITH E (1983) Cognitive deficits in the early stages of Parkinson's disease. Brain, 106,
257-270.
LISBERGER S G, EVTNGER C, JOHANSON G W, FUCHS A F (1981) Relation between eye acceleration and
retinal image velocity during foveal smooth pursuit in man and monkey. Journal of Neurophysiology, 46, 229-249.
LURJA A R (1969) Frontal lobe syndromes, In: Handbook of Clinical Neurology, Volume 2. Edited by
P. J. Vinken and G. W. Bruyn. Amsterdam: North-Holland, pp. 725-757.
LURIA A R, KARPOV B A, YARBUSS A L (1966) Disturbances of active visual perception with lesions of
the frontal lobes. Cortex, 2, 202-212.
MARTIN J P (1967) The Basal Ganglia and Posture. London: Pitman Medical, pp. 33-35.
MELVILL JONES G, MANDL G (1976) Visual tracking of sinusoidal target movement in Parkinson's
disease. DRB Aviation Medical Research Unit Report, DR 225, 271-287.
MOREL-MAROGER A (1977) Effects of levodopa on 'frontal' signs in Parkinsonism. British Medical
Journal, 2, 1543-1544.
NOBLE M, FITTS P M, WARREN C E (1955) The frequency response of skilled subjects in a pursuit
tracking task. Journal of Experimental Psychology, 49, 249-256.
POLIDORA V J, RATOOSH P, WESTHEIMER G (1957) Precision of rhythmic responses of the oculomotor
system. Perceptual and Motor Skills, 7, 247-250.
SHARPE J A, SYLVESTER T O (1978) Effect of aging on horizontal smooth pursuit. Investigative
Ophthalmology and Visual Science, 17, 465-468.
SHIBASAKI H, TSUJI S, KUROIWA Y (1979) Oculomotor abnormalities in Parkinson's disease. Archives
of Neurology, Chicago, 36, 360-364.
SHIMIZU N, NATTO M, YOSHIDA M (1981) Eye-head co-ordination in patients with Parkinsonism and
cerebellar ataxia. Journal of Neurology, Neurosurgery and Psychiatry, 44, 509-515.
SMITH A T, BITTENCOURT P R M, LLOYD D S L , RICHENS A (1981) An efficient technique for
determining characteristics of saccadic eye movements using a minicomputer. Journal of
Biomedical Engineering, 3, 39-43.
SPOONER J W, SAKALA S M, BALOH R W (1980) Effect of aging on eye tracking. Archives of Neurology,
Chicago, 37, 575-576.
STARK L (1968) Neurological Control Systems: Studies in Bioengineering. New York: Plenum Press,
pp. 338-347.
940
A. M. BRONSTEIN AND C. KENNARD
STARK L, VOSSIUS G, YOUNG L R (1962) Predictive control of eye tracking movements. IRE
Transactions on Human Factors in Electronics, HFE-2, 52-57.
STERN Y, MAYEUX R, ROSEN J, ILSON J (1983) Perceptual motor dysfunction in Parkinson's disease: a
deficit in sequential and predictive voluntary movement. Journal of Neurology, Neurosurgery and
Psychiatry, 46, 145-151.
TERAVAINEN H, CALNE D B (1980a) Studies of parkinsonian movement: 1. Programming and execution
of eye movements. Ada Neurologica Scandinavica, 62, 137-148.
TERAVAINEN H, CALNE D B (19806) Studies of parkinsonian movement: 2. Initiation of fast voluntary
eye movement during postural disturbance. Ada Neurologica Scandinavica, 62, 149-157.
VINCENT S R, HATTORI T, MCGEER E G (1978) The nigrotectal projection: a biochemical and
ultrastructural characterization. Brain Research, Amsterdam, 151 159-164.
WHITE O B, SAINT-CYR J A, TOMLINSON R D, SHARPE J A (1983) Ocular motor deficits in Parkinson's
disease. II. Control of the saccadic and smooth pursuit systems. Brain, 106, 571-587.
WURTZ R H, GOLDBERG M E (1972) Activity of superior colliculus in behaving monkey. III. Cells
discharging before eye movements. Journal of Neurophysiology, 35, 575-586.
(Received January 2,1985. Revised March 19, 1985. Accepted April 10, 1985)