Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
C. GRACE PETRIKOWSKI
isorders of tlJe temporomandibular joint are
-that interfere with the normal
form or function of the joint. These disorders include
dysfunction of the articular disk and associated ligaments and muscles, joint arthritides, inflammatory
lesions, neoplasms, and growth or developmental
abnormalities.
including diagnostic imaging, before commencing
treatment.
The clinical signs and symptoms of :Otherdisorders
of the TMJ may include swelling in and around the
joint, an elevated temperature, and rednessof the overlying skin.
Clinical Features
'Iemporomandibular joint ('I'MJ) dysfunction is the
most common jaw disorder, with 28% to 86% of adults
and adolescentsshowing one or more clinical signs or
symptoms,A higher incidence of the disorder has been
reported in females, although the reason for this preponderance is not clear. Signs and symptoms of dysfunction may include one or more of the following:
pain in the TMJ or ear or both, headache, muscle tenderness,joint stiffness, clicking or other joint noises,
reduced range of motion, locking, and subluxation. In
most casesthe clinical signs and symptoms are transitory, and treatment is not indicated. However, a small
percentage of patients (5%) suffer severe dysfunction
(e.g., severe pain, marked functional impairment, or
both), which requires a thorough diagnostic workup,
~jl5
""UY"'Y
TMJ imaging may be necessaryto supplement information obtained from the clinical examination, particularly when an osseous abnormality or infection is
suspected,conservative treatment has failed, or symptoms are worsening. Diagnostic imaging also should
be considered for patients with a history of trauma, significant dysfunction, alteration in range of motion,
sensory or motor abnormalities, or significant changes
in occlusion. TMJ imaging is not indicated for joint
sounds if other signs or symptoms are absent or for
asymptomatic children and adolescentsbefore orthodontic treatment. The purposes of TMJ imaging are to
evaluate the integrity and relationships of the hard and
soft tissues,confirm the extent or stage of progression
CHAPTER
25
DIAGNOSTIC
IMAGING
OF THE
TEMPOROMANDIBULAR
539
JOINT
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
importance of understanding the range of normal
appearance. The extreme aspects of,the condyle are
called the medialpoleand lateralpoles.The long axis of
the condyle is slightly rotated on the condylar neck such
that the medial pole is angled posteriorly, forming an
angle of 15 to 33 degrees with the sagittal plane. The
two condylar axes typically intersect near the anterior
border of the foramen magnum in the submentovertex
projection.
Most condyles have a pronounced ridge oriented
mediolaterally on the anterior surface, marking the
anteroinferior limit of the articulating area. This ridge
is the upper limit of the pterygoid fovea,a small depression on the anterior surface at the junction of the
condyle and neck. It is the attachment site of the superior head of the lateral pterygoid muscle and should
not be mistaken for an osteophyte (spur), which indicates degenerative joint disease.
Although the mandibular and temporal components
of the TMJ are calcified by 6 months of age, complete
calcification of cortical borders may not be completed
until 20 years of age. As a result, radiographs of condyles in children may show little or no evidence of a
cortical border. In the absence of disease,the cortical
borders in adults are visible radiographically. A layer of
fibrocartilage covers the condyle but. is not visible
radiographically.
of known disease, 'and evaluate the effects of treatment.
The clinician must correlate the radiographic information with the patient's history and clinical findings to
arrive at a final diagnosis and plan the management of
the underlying disease process.
.
A thorough understanding of the anatomy and morphology of the TMJ is essential so that a normal variant
is not mistaken for an abnormality. The TMJs are
unique in that although they constitute two separate
joints anatomically, they function together as a single
unit. Eachcondyle articulates with the mandibular fossa
of the temporal bone. A disk composed of fibrocartilage is interposed between the condyle and mandibular fossa. A fibrous capsule lined with synovial
membrane surrounds and enclosesthejoint. Ligaments
and muscles restrict or allow movement of the condyle.
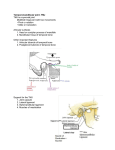
CONDYLE
The condyle is a bony, ellipsoid structure connected to
the mandibular ramus by a narrow neck (Fig. 25-1).
The condyle is approximately 20 mm long mediolaterally and 8 to 10mm thick anteroposteriorly. The shape
of the condyle varies considerably; the superior aspect
may be flattened, rounded, or markedly convex,
whereas the mediolateral contour usually is slightly
convex. These variations in shape may cause difficulty
with radiographic interpretation; this underlines the
A
FIG. 25-1
MANDIBULAR
FOSSA
The glenoid (mandibular) fossa is located at the inferior aspectof the squamous part of the temporal bone
and is composed of the glenoid fossaand articular eminence of the temporal bone (Fig. 25-2, A). It is some-
B
Mandibular
condyle. The medial pole (arrow) is on the right in each case.
A, Anterior aspect. B, Superior aspect.
PART V
540
RADIOGRAPHIC
INTERPRETATION
OF PATHOLOGY
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
~
FIG. 25-2
A, Basal view of the skull showing the mandibular fossa. AE, Articular eminence; A7; articular tubercle; CC, carotid canal; EAM, external auditory meatus; Mf;
mandibular fossa; Sf; squamotympanic
fissure; ZA, zygomatic arch. B, Pneumatization of
the articular eminence with a mastoid air cell (panoramic view) (arrow). (B, Courtesy Dr.
D. Tyndall and Dr. S.R. Matteson, Chapel Hill, N.C.)
times described as the temporalcomponentof the 'I'MJ.
The articular eminence forms the anterior limit of the
glenoid fossa and is convex in shape. Its most inferior
aspectis called the summitor apexof the eminence. In
a normal TMJ, the roof of the fossa,the posterior slope
of the articular eminence, and the eminence itself form
an S shape when viewed in the sagittal plane. The most
lateral aspect of the eminence consists of a protuberance,called the articular tubercle,
which is a ligamentous
attachment. The squamotympanic fissure and its medial
extension, the petrotympanic fissure, form the posterior limit of the fossa.The middle portion of the roof
of the fossa forms a small portion of the floor of the
middle cranial fossa,and only a thin layer of cortical
bone separates the joint cavity from the intracranial
subdural space. The spine of the sphenoid forms the
medial limit of the fossa. Fossa depth varies, and the
development of the articular eminence relies on functional stimulus from the condyle. For example, the
mandibular fossa is very flat and underdeveloped in
patients with micrognathia or condylar agenesis.The
fossaand articular eminence develop during the first 3
years and reach mature shape by the age of 4 years;
young infants lack a definite fossa and articular
eminence.
All aspectsof the temporal component may be pneumatized with small air cells derived from the mastoid
air cell complex (Fig. 25-2, B). Pneumatization of
the articular eminence is seen radiographically in
approximately 2% of patients. Like the condyle, the
mandibular fossa is covered with a thin layer of
fibrocartilage.
INTERARTICULAR
DISK
The interarticular disk (meniscus), composed of
fibrous connective tissue,is located between the condylar head and mandibular fossa. The disk divides the
joint cavity into two compartments, called the inferior
(lower) and superior (upper) joint spaces,which are
located below and above the disk, respectively (Fig.
25-3). A normal disk has a biconcave shape with a
thick anterior band, thicker posterior band, and a thin
middle part. The disk also is thicker medially than laterally. The medial and lateral margins of the disk blend
with the capsule. The thin central portion normally
serves as an articulating cushion between the condyle
and articular eminence. The anterior band is thought
to be attached to the superior head of the lateral pterygoid muscle, and the posterior band attachesto the posterior retrodiskal tissues (also called the posterior
attachment).The junction between the posterior band
and posterior attachment usually lies within 10 degrees
of vertical above the condylar head. The disk and posterior attachment are collectively called the softtissue
componentofthe TMJ
During mandibular opening, as the condyle translates downward and forward, the disk, also moves
:J
CHAPTER 25
DIAGNOSTIC
IMAGING
OF
THE
TEMPOROMANDIBULAR
541
JOINT
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
.
Joint space
{
Synovial membrane
Superior,
I
Inferior \
/
Interarticular
disk,
LaterC11 I
pterygoi;::
,
Superiorbelly.
muscle
Inferiorbelly-
l
.
c~nective
Articular surfaces,
Articular
eminence
~
Superior lamina
} -posterior
tissue
attachment
"
Synovial membrane
A
Middle
cranial
'"'~~_/
Inferior
Articular
surfaces-
/
jJOlnt space
Interarticula r disk
_Articular
eminence
Mandibular condyle
Lateral capsular wall
Medial collateral ligament'
Medial capsular
c
FIG. 25-3
TMj anatomy. A, Lateral view. B, Sectioned cadaver specimen In the same
orientation. Af, Articular eminence; /0, interarticular disk; LPM,lateral pterygoid muscle;
MC, mandibular condyle; PA,posterior attachment. C, Coronal view. (Courtesy Dr. W.K.
Solberg, Los Angeles, Calif.)
forward and rotates so that its thin central portion
remains between the articulating convexities of the
condylar head and articular eminence. Laterally and
medially, the disk attaches to the condylar poles,
helping to ensure passivemovement of the disk with the
condyle so that the condyle and disk translate forward
together to the summit of the articular eminence. As
the mandible opens, the condyle also rotates against the
lower surface of the disk in the inferior joint space.On
mandibular closing, this process reverses,with the disk
moving back with the condyle into the mandibular
fossa.
superior lamina stretches and allows the dISk to move
forward with condylar translation. The inferior lamina
attaches to the posterior surface of the condyle. The
posterior attachment is covered with a synovial mem.brane that secretessynovial fluid, which lubricates thejoint.
As the condyle moves forward, tissuesof the posterior attachment expand in volume, primarily as a
result of venous distention, and as the disk moves
forward, tension is produced in the elastic posterior
attachment. This tension is thought to be responsible
for the smooth recoil of the disk posteriorly as the
mandible closes.
POSTERIOR ATTACHMENT
TMJ BONY RELATION5HIPS
(RETRODISKAl
TISSUES)
The posterior attachment consistsof a bilaminar zone
of vascularizedand innervated loose fibroelastic tissue.
The superior lamina, which is rich in elastin, inserts
into the posterior wall of the mandibular fossa. The
RadiograPhicjoint spaceis a general term used to describe
the radiolucent area between the condyle and temporal component (see Fig. 25-3). This general term
should not be confused with the terms suPerior joint
spaceand inferiorjoint spacedescribed earlier, which refer
542
PART V
RADIOGRAPHIC
INTERPRETATION
OF PATHOLOGY
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
to soft tissuespacesabove and below the disk. The radiographic joint space contains the soft tissue components of the joint. The left and right condylar positions
within the fossa can be determined and compared by
the dimensions of the radiographic joint spaceviewed
on corrected lateral tomographs. A condyle is positioned concentrically when the anterior and posterior
aspectsof the radiolucent joint space are uniform in
width. The condyle is retruded when the posterior joint
spacewidth is less than the anterior (Fig. 25-4) and protruded when the posterior joint spaceis wider than the
anterior. .
The diagnostic significance of mild or moderate
condylar eccentricity is not clear; condylar eccentricity is seen in one third to one half of asymptomatic
individuals and is not a reliable indicator of the soft
tissue statusof the joint, particularly because the shape
of the condylar head is not concentric to the shape
of the fossa. Markedly eccentric condylar positioning
usually represents an abnormality. For example, inferior condylar positioning (widened joint space) may be
seen in casesinvolving fluid or blood within the joint,
and superior condylar positioning (decreased joint
space or no joint space, with osseous contact of joint
components) may indicate loss,.displacement, or perforation of intracapsular soft tissue components.
Marked posterior condylar positioning is seen in some
casesof disk displacement, and marked anterior condylar positioning may be seen in juvenile rheumatoid
arthritis.
CONDYLAR MOVEMENT
The condyle undergoes complex movement during
mandibular opening. Downward and forward translation (sliding) of the condyle occurs, whereby the
A
superior surface of the disk slides against the articular
eminence; at the same time a hingelike, rotatory movement occurs with the superior surfac~ of the condyle
against the inferior surface of the disk. The extent of
normal condylar translation varies considerably. In
most individuals, at maximal opening the condyle
moves down and forward to the summit of the articular eminence or slightly anterior to it (see Fig. 25-4).
The condyle typically is found within a range of 2 to
-5mm posterior and 5 to 8mm anterior to the crest of
the eminence. Reduced condylar translation, in which
the condyle has little or no downward and f{)rward
movement and does not leave the mandibular fossa,is
seen in patients who clinically have a reduced degree
of mouth opening. Hypermobility of the joint may be
suspected if the condyle translates more than 5 mm
anterior to the eminence. This may permit anterior
locking or dislocation of the condyle if a superior movement also occurs above and anterior to the summit of
the articular eminence.
The type of imaging technique selecteddepends on the
specific clinical problem, whether imaging of hard or
soft tissuesis desired, the amount of diagnostic information available from a particular imaging modality,
the cost of the examination, and the radiation dose. In
most casesthe imaging protocol begins with hard tissue
imaging to evaluate the osseouscontours, the positional
relationship of the condyle and fossa,and the range of
motion, although a combination of imaging techniques may be indicated. Soft tissue imaging is indicated
when information about disk position, morphology, or
integrity is needed or to image abnormalities in the
~
\,;
FIG. 25-4
Corrected lateral (sagittal) tomograms. A represents a lateral image slice, and
B represents a medial image slice of the same joint. Notice that the condyle appears centered in the lateral image and retruded in the medial image. C, Open view showing the
degree of condyle translation during mandibular opening.
rl
"""
CHAPTER
25
DIAGNOSTIC
IMAGING
OF
THE
TEMPOROMANDIBULAR
543
JOINT
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
FIG. 25-5
Panoramic view. The right condyle is smaller than the left and is not smoothly
corticated. Tomograms later showed marked erosive changes of the right condylar head.
muscles or surrounding tissues.A summary of the diagnostic information provided by eachimaging technique
is presented in Table 25-1.
HARD TISSUE IMAGING
Panoramic Projection
Becausethe panoramic projection provides an overall
view of the teeth and jaws, it servesas a screening projection to identify odontogenic diseasesand other disorders that may be the source of TMJ symptoms,Some
panoramic machines'have specific TMJ programs, but
these are of limited usefulness becauseof thick image
layers and the oblique, distorted view of the joint they
provide, which severely limits image quality, Gross
osseouschangesin the condyles maybe identified, such
as asymmetries,extensive erosions, large osteophytes,
or fractures (Fig. 25-5). However,no information about
condylar position or function is provided because the
mandible is partly opened and protruded when this
radiograph is exposed,Also, mild osseouschanges may
be obscured,and only marked changes in articular eminence morphology can be seen as a result of superimposition by the skull baseand zygomatic arch. For these
reasons,the panoramic view does not provide an adequate examination of the hard tissuesof the joints.
Transcranial Projection
The transcranial projection provides a sagittal view of
the lateral aspectsof the condyle and temporal component. The patient is positioned in a cephalostat; the
x-ray beam is directed downward from the opposite
side, through the cranium and above the petrous ridge
of the temporal bone, at a 25-degreepositive angle centered through thejoint. The horizontal direction of the
beam mav be individually corrected for the condylar
long axis (see Conventional Tomography, Chapter 13),
an average 20-degree anterior angle may be used. The
film cassetteis placed on the side to be imaged (Fig. 256). A routine transcranial seriesincludes projections of
both TMJs in the closed and maximally open positions
(Fig. 25-7).
Becauseof the positive beam angulation, the central
and medial aspectsof the joint are projected inferiorly,
and only lateral joint contours are visible in this pro-
\
/
A
A
250
to
\
'f--:::::=:~-=-"~
\
B
',~200
FIG. 25-6
Transcranial projection. A, The central ray is
oriented at a 25-degree positive angle from the opposite side
(8) and anteriorly 20 degrees, centered over the TM] of
interest.
,+,
,
544
PART V
RADIOGRAPHIC
INTERPRETATION
OF PATHOLOGY
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
IMAGING TECHNIQUE*
Arthridites
+
++
Developmental abnormalities
-1-t-
Trauma (fracture)
Asymmetry
-to
+
+
"
+
+
++
+
-t-
1-1+
-t-t-
-t-t-
-to
+
+
++
T
"t-
Soft Tissue
Disk perforation
joint effusion
JOintspace calcifications
Modified from Brooks SL et al: Imaging of the temporomandibular joint, position paper ot the American Acatlemy ot Ural anti Maxiliotacial KatllOlogy, Ural :)urg
Oral Pathol Oral Radiol Endod 83:609,1997.
*-, Does not provide diagnostic information for the abnormality; +, only occasionally useful; ++, often useful; +++, almost always useful.
tWhen including arthrocentesis.
jection. l'he Ipsl1ateralpetrous ndge otten ISsupenmposed over the condylar neck, which may obscure
osseouschanges in the condyle or temporal component. The image of the condyle, temporal component,
and joint space is distorted, and condylar position
cannot be reliably determined, particularly if the horizontal beam angle is not individualized for each
patient. The transcranial projection is useful for identifying grossosseouschanges on the lateral aspectof the
joint only, displaced condylar fractures, and range of
motion (open views).
degrees trom the anterior (Yig. ~5-~); the hIm cassette
is placed on the side being imaged. The patient opens
the mouth maximally to avoid superimposition of the
condyle on the temporal component. Because of the
negative beam angulation, this view depicts the medial
aspect of the condyle. The transpharyngeal view provides limited diagnostic information because the temporal component is not imaged well (Fig. 25-9). The
transpharyngeal projection is effective for visualizing
erosive changesof the condyle rather than more subtle
changes.
Transpharyngeal
(parma) t'rO)ectlon
The transpharyngeal (Parma) projection provides a
sagittal view of the medial pole of the condyle. The xray beam is directed superiorly at -5 degrees through
the sigmoid notch of the opposite side and 7 to 8
Transorbital
Projection
The transorbital projection is similar to the transmaxillary projection in that both provide an anterior view of
the TMJ, perpendicular to transcranial and transpharyngeal projections. In the transorbital view, the
CHAPTER 25
DIAGNOSTIC
IMAGING
OF THE
TEMPOROMANDIBULAR
545
JOINT
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
IMAGING TECHNIQUE*
SKULLVIEWS
CONVENTIONAL
COMPUTED
TOMOGRAPHY
TOMOGRAPHY
MAGNETIC
ARTHROGRAPHY
RESONANCE IMAGING
++
+t+
+++
+
++-
+1-+
+
++
++
+++
++
-++
++
+
+t+
c+++
++
Tt+
patient's head is tilted downward 10 degreesso that the
canthomeatalline is horizontal (Fig. 25-10). The x-ray
beam is directed from the front of the patient through
the ipsilateral orbit and TMJ of interest. The film cassette is placed behind the patient's head, perpendicular to the x-ray beam. The patient opens maximally or,
as an alternative, protrudes the mandible, thereby positioning the condyle at the summit of the articular eminence and avoiding superimposition of the articular
eminence or skull base on the condyle.
The entire mediolateral dimension of the articular
eminence, condylar head, and condylar neck is visible,
which makes this view particularly useful for visualizing
condylar neck fractures. The morphology of the convex
surface of the condylar head can be evaluated,making
this projection a useful adjunct to transcranial and
transpharyngeal projections in the diagnosis of gross
+++
Ii +
degenerative changes or other anomalies (Fig. 25-11).
The usefulnessof this projection is limited by the ability
of the condyle to move to the summit of the articular
eminence. If condylar motion is limited, only the condylar neck is visible becauseareasof the joint articulating
surfaces are obscured by superimposition of the temporal component on the condylar head. A similar projection is the reverse open Towne's projection, which
sometimes is used to image condylar neck fractures,
particularly if medial displacement has occurred,
because the condylar head and neck are visualized in
the frontal plane.
Submentovertex (Basal) Projection
The submentovertex (SMV) projection provides a view
of the skull base and condyles superimposed on the
condylar necks and mandibular rami. For this reason
PART V
546
RADIOGRAPHIC
INTERPRETATION
OF PATHOLOGY
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
B
FIG. 25-7
Transcranial projections of the left TM). The profile of the lateral aspect of
the condylar head is indicated by an arrow. Note the degree of translatory movement
between the closed view (A) and the open view (8).
FIG. 25-8
Transpharyngeal projection. A, The central ray
is oriented superiorly 5 to 10 degrees and (8) posteriorly
approximately 10 degrees, centered over the TMJ of interest. Note that the mandible
is positioned
at maximal
opening.
the SMV projection often is used to determine the
angulations of the long axis of the condylar head
for corrected tomography (see Chapter 11 for technique). This view may be used as an adjunct to views
depicting the TMJs in the lateral plane and is particularly useful for evaluating facial asymmetries, condylar
displacement, or rotation of the mandible in the hori-
FIG. 25-9
Transpharyngeal projection showing the
condyle at the articular eminence. The zygomatic arch is
superimposed over the glenoid fossa.
zontal plane associated with trauma or orthognathic
surgery.
Conventional Tomography
Tomography is a radiographic technique that produces
multiple thin image slices, permitting visualization of
an anatomic structure essentially free of superimpositions of overlapping structures (see Chapter 13).
Because this technique can provide multiple image
r
~:
~
~
CHAPTER
Z.5
UIAI.JNU:'
IlL
IMAI.JINI.J
Ut
..MI:
II:Mt'UKUMAI"U'DULAK
:>4/
IUI""
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
\
'\
-..
"""'"
~
/
'"
I-IL.. Z~-l U
IranSOrOI1:alproject:lon. I ne cenual ray ISorlemea aownwara apprOXlmal:elY
10 degrees and laterally approximately
30 degrees through the ipsilateral orbit, centered
over the TMJ of interest.
tiLl.
~3-1
I
Irilll~UrUllill
VIt:W
~IIUWIIIY
lIl~
LUIIUYI~
(arrow) below the articular eminence. The mastoid process
partly obscures the articulating surface on the most medial
aspect.
Sllces
at
rlgllt
allgl~~
UllUUgll
UI~ jUllll,
II l~ ~Up"llUl
lU
the transcranial view in depicting true condylar position and revealing osseouschanges. For these reasons,
tomography is a valuable adjunct to plain film radiography and can provide information that may not be
available with plain films alone.
lomograpns typIcallY are exposea ill me sagllIal
(lateral) plane with several image slices in the closed
(maximal intercuspation) position and usually only one
image in the maximal open position. In "corrected"
sagittal tomography, the condylar long axis with respect
to the midsagittal plane is determined using an SMV
projection (Fig. 25-12): The patient's head is then
rotated to this angle, permitting alignment of image
slices perpendicul,ar to the condylar long axis. This
minimizes geometric distortion of the joint and allows
accurate assessmentof condylar position. Although a
corrected tomographic technique is preferred, when
not available,a 20-degreehead rotation toward the side
of interest is superior to image slicesparallel to the midsagittal plane. To minimize patient movement in open
views, a bite-block may be inserted between the
patient's anterior teeth becauseit takes severalseconds
to complete each tomographic exposure.
It is desirable to supplement this examination
with coronal (frontal) tomographs, particularly when
morphologic abnormalities or erosive changes of the
condylar head are suspected. For coronal tomographs, the patient is in a maximal open or protruded
position, which brings the condyle to the summit of
the articular eminence, free of superimposition of
the posterior slope of the eminence. The entire
condylar head is visible in the mediolateral plane (Fig.
25-13).
\..ompU1:eo
lomograpny
Computed tomography (CT) is indicated when more
information is needed about the three-dimensional
shape and internal structure of the osseous compo-
PART V
548
RADIOGRAPHIC
INTERPRETATION
OF PATHOLOGY
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
nents of the joint or if information regarding the surrounding soft tissues is required. CT produces digital
image slices (see Chapter 13). Multiple image slicesare
made in both the axial and coronal planes, although
the coronal imagesare the more useful. Data from axial
and coronal scans can be manipulated to produce
(reformat) images in the sagittal plane. Threedimensional reformatted images also can be produced.
These are useful for assessingosseousdeformities of the
jaws or surrounding structures. CT cannot produce
accurate images of the articular disk.
CT may be considered for determining the'presence
and extent of ankylosis and neoplasms and the extent
of bone involvement in some arthritides, imaging
complex fractures, and evaluating complications from
the use of polytetrafluoroethylene or silicon sheet
implants such as erosions into the middle cranial fossa
and heterotopic bone growth.
SOFT TISSUE IMAGING
FIG. 25-12
SMV projection. Tracing of angles between
the long axis of each condyle and the midsagittal plane. For
tomographic views the patient is rotated according to the
measured angles to produce an undistorted radiographic
view of each TM).
FIG. 25-13
lar condyle.
Frontal tomographic image of the mandibu-
The soft tissuesof the joint can be imaged with magnetic resonance imaging (MRI) or arthrography. Conventional imaging techniques do not demonstrate disk
position, morphology, or functiop. Soft tissue imaging
is indicated when TMJ pain and dysfunction are present
or when the clinical findings suggestdisk displacement
along with symptoms that are unresponsive to conservative therapy.
MRI and arthrography should be used only when
information about the condition of the soft tissue components of the joint is required to formulate a treatment plan. The choice of technique depends on patient
factors, such as allergy to contrast agents and claustrophobia, as well as on the cost,availability, and objectives
of the imaging technique. Arthrography is superior for
diagnosis of small disk perforations and joint adhesions. MRI can indicate a pathologic condition of the
soft tissue through altered tissue signal, allowing evaluation of the disk and surrounding muscles, and can
image joint effusion. The technique is noninvasive and
does not use ionizing radiation. Arthrography with
videofluoroscopy provides a superior motion study of
the joint, although some MRI techniques can provide
limited dynamic information.
Arthrography
Imaging of the hard tissuesshould be completed before
arthrographic imaging is performed. Arthrography is a
technique in which an indirect image of the disk is
obtained by injecting a radiopaque contrast agent into
one or both joint spaces under fluoroscopic guidance
(Fig. 25-14). A perforation is detected by the flow of
contrast agent into the superior joint space from the
CHAPTER
25
DIAGNOSTIC
IMAGING
OF THE
TEMPOROMANDIBULAR
JOINT
549
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
a
A
FIG. 25-14
A and B, Arthrographs in which both the lower and upper joint spaces have
been injected with contrast media (spaces appear white) that highlights the disc (black). In
both images the anterior aspect of the patient is on the left side of the image. In A the
posterior band (white arrow) and the anterior band (black arrow) are evident. B reveals a
disc with an enlarged posterior band (arrow).
lower space,and adhesions are detected by the manner
in which contrast agent fills the joint space.Mter both
spacesare filled, disk function is studied using fluoroscopy during open and closing movements. The
fluoroscopic study usually is supplemented with tomographs of the joint.
Arthrography is indicated when information about
disk position, function, morphology, and the integrity of
diskal attachments is required for treatment planning.
The risks of this procedure include allergic reactio~nto
the nonionic iodine contrast agent and infection. Draw-
backs of this procedure are its invasive nature and its
association with postoperative discomfort.
Magnetic Resonance Imaging
MRI uses a magnetic field and radiofrequency pulses
rather than ionizing radiation to produce multiple
digital image slice~ (see Chapter 13). BecauseMRI can
provide superb imagesof soft tissues,this technique can
be used for imaging the articular disk. MRI allows construction of images in the sagittal and coronal planes
without repositioning the patient (Fig. 25-15). These
DC
FIG. 25-15
MRI of a normal TM!. A, Closed view showing the condyle and temporal
component. The biconcave disk is located with its posterior band (arrow) over the condyle.
B, Coronal image showing the osseous components and disk (arrows) superior to the
condyle. (Courtesy Dr. Per-Lennart Westesson, Rochester, N.Y.)
550
PART V
RADIOGRAPHIC
INTERPRETATION
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
images usually are acquired in open and closed
mandibular positions using surface coils to improve
image resolution. Sagittal slicesshould be oriented perpendicular to the condylar long axis. The examinations
usually are performed using Tl-weighted, protonweighted, or T2-weighted pulse sequences.Tl-we'ighted
or proton-weighted images best demonstrate osseous
and diskal tissues,whereas T2-weighted images demonstrate inflammation and joint effusion. Motion MRI
studies durin~ opening and closing can be obtained by
having. the patient open in a seriesof stepped distances
and using rapid image acquisition. ("fast scan") techniques. Medial disk displacements are best detected
using MRI. The change in tissue signal that results from
tissue changes in the disk and retrodiskal tissue may
make accurate identification of the disk difficult.
MRI does not have the morbidity associatedwith the
introduction of needles into the joint (as occurs in
arthrography), but MRI is a more expensive examination and is contraindicated in patients who are pregnant or who have pacemakers, intracranial vascular
clips, or metal particles in vital structures. Some
patients may not be able to tolerate the procedure
because of claustrophobia or an inability to remain
motionless.
Radiographic
of the TMJ
Abnormalities
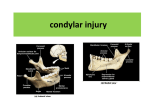
DEVELOPMENTAL ABNORMALITIES
Developmental abnormalities may be broadly categorized as anomalies in the form and size of joint components. The most striking radiographic changes
usually are seen in the condyle, although the temporal
component also may be deformed, often remodeling to
accommodate the abnormal condyle. Condylar articular cartilage is a mandibular growth site, and as a result,
developmental abnormalities at this location may manifest as altered growth on the affected side of the
condyle, mandibular ramus, mandibular body, and
alveolar process on the affected side(s).
CONDYLAR
HYPERPLASIA
Definition
Condylar hyperplasia is a developmental abnormality
that results in enlargement and occasionally deformity
of the condylar head; this may have a secondary effect
on the mandibular fossaas it remodels to accommodate
the abnormal condyle. The etiology may be overactive
cartilage or persistent cartilaginous rests,increasing the
thickness of the entire cartilaginous and precartilagi-
OF
PATHOLOGY
nous layers.This condition uslJallyis unilateral and may
be accompanied by varying degre~s of hyperplasia of
the ipsilateral mandible.'
Clinical Features
Condylar hyperplasia is more common in males,and it
usually is discovered before the age of 20 years. The
condition is self-limiting and tends to arrest with termination of skeletal growth, although in a small
number of casescontinued growth and adult onsethave
been reported. The condition may progress slowly or
rapidly. PatientS have a mandibular asymmetry that
varies in severity,depending on the degree of condylar
enlargement. The chin may be deviated to the unaffected side, or it may remain unchanged but with an
increase in the vertical dimension of the ramus,
mandibular body, or alveolar process of the affected
side. As a result of this growth pattern, patients may
have a posterior open bite on the affected side. Patients
may also have symptomsrelated to TMJ dysfunction and
may complain of limited or deviated mandibular
opening or both caused by restricted mobility of the
enlarged condyle.
Radiographic Features
The condyle may appear relatively normal but symmetrically enlarged, or it may be altered in shape (e.g.,
conical, spherical, elongated, lobulated) or irregular in
outline. It maybe more radiopaque becauseof the additional bone present. A morphologic variation manifesting as elongation of the condylar head and neck with a
compensating forward bend, forming an inverted L,
may be seen. Also, the condylar neck may be elongated
and thickened and may bend laterally when viewed
in the coronal (anteroposterior) plane (Fig. 25-16).
The cortical thickness and trabecular pattern of the
enlarged condyle usually are normal, which helps to distinguish this condition from a condylar neoplasm. The
glenoid fossa may be enlarged, usually at the expense
of the posterior slope of the articular eminence. The
ramus and mandibular body on the affected side also
may be enlarged, resulting in a characteristic depression of the inferior mandibular border at the midline,
where the enlarged sidejoins the contralateral normal
mandible. The affected ramus may have increased vertical depth and may be thicker in the anteroposterior
dimension.
Differential Diagnosis
A condylar tumor, most notably an osteochondroma, is
included in the differential diagnosis. An osteochondroma usually is more irregular in shapecompared with
a hyperplastic condyle. Surface irregularities and continued growth after cessationof skeletal growth should
CHAPTER
25
DIAGNOSTIC
IMAGING
OF THE
TEMPOROMANDIBULAR
JOINT
551
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
increase suspicion of this tumor. Occasionally a condylar osteoma or large osteophyte that occurs in chronic
degenerative joint disease may simulate condylar
hyperplasia.
Treatment
Treatment consisting of orthodontics combined with
orthognathic surgery ideally should be attempted
after condylar growth is complete. Determining when
condylar growth has stopped may be difficult; imaging may include longitudinal radiographic studies to
assessthe dimensions of the condyle and mandible,
nuclear imaging techniques, 'or both. A lack of unusual bone activity, demonstrated in a technetium
bone scan, is a useful indication of arrested condylar
growth.
PART V
552
RADIOGRAPHIC
INTERPRETATION
OF
PATHOLOG'
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
CONDYLAR
HYPOPLASIA
Definition
Condylar hypoplasia is failure of the condyle to attain
normal size because of congenital and developmental
abnormalities or acquired diseasesthat affect condylar
growth. The condyle is small, but condylar morphology
usually is normal. The condition may be inherited
or may appear spontaneously. Some caseshave been
attributed to early injury or injury to the articular cartilage by birth trauma or intraarticular inflammatory
lesions..
Clinical Features
Condylar hypoplasia usually is a component of a
mandibular growth deficiency and therefore often is
associated with an underdeveloped ramus and (occasionally) mandibular body. Congenital abnormalities
may be unilateral or bilateral and usually are manifestations of a more generalized condition (e.g., micrognathia, Treacher Collins syndrome); they also may be
associatedwith congenital defects of the ear and zygomatic arch. Developmental abnormalities that manifest
during growth usually are unilateral. Acquired abnormalities are the result of damage during the growth
period from sources such as therapeutic radiation or
infection that diminish or prevent further condylar
growth and development. Patients with condylar
hypoplasia have ~andibular asymmetry and may have
symptoms of TMJ dysfunction. The chin commonly is
deviated to the affected side, and the mandible deviates
to the affected side during mandibular opening.
Degenerative joint disease is a common long-term
Radiographic Features
The condyle may be normal in shap~ and structure but
is diminished in size, and the mandibular fossa also is
proportionally small. The condylar neck and coronoid
process usually are very slender and in some casesare
shprtened or elongated. The posterior border of the
ramus and condylar neck may have a dorsal (posterior)
inclination. The ramus and mandibular body on the
affected side may also be small, resulting in a mandibular asymmetryand occasional dental crowding, depending on the severity of mandibular underdevelopment.
The antegonial notch is deepened. The associated
mandibular hypoplasia is more pronounced if the
effect takes place early in life (Fig. 25-17).
Differential Diagnosis
Condylar destruction from juvenile rheumatoid arthritis may appear similar to that of hypoplasia. A surveyof
other joints or testing for rheumatoid factor may be
helpful. Changes in condylar morphology in severe
degenerative joint diseaseor other arthritic conditions
may have a similar appearance, although arthritic
disease does not cause mandibular hypoplasia of the
affected side unless it occurs during growth and other
signs of arthritis are usually visible in the affected joint.
Ireatment
Orthognathic surgery, bone grafts, and orthodontic
therapy may be required.
JUVENILE
ARTHROSIS
Synonyms
Boering's arthrosis and arthrosis deformans juvenilis
sequela.
FIG. 25-17
A panoramic film revealing hypoplasia ot the left condyle. In tnlS case tne
hypoplasia is restricted to the condylar head and neck with minimum involvement of the
mandibular
ramus and body.
r"APTI=g
7~
nIAr:"'{)~Tlr
'~AAr:I'-Ir:
nl:
TWI:
TFMPnRnMANDIBLJLAR
""~
IOINT
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
Definition
juvenile arthrosis, a condylar growth disturbance first
described by Boering, manifests as hypoplasia and characteristic morphologic abnormalities. This condition
may be a form of condylar hypoplasia but is thought to
differ in that the affected condyle at one time ,was
normal and became abnormal during growth. juvenile
arthrosis may be unilateral or bilateral, and it predisDoses the TMT to secondary degenerative changes.
Clinical
Featur.esjuvenile
arthrosis affects children and adolescents
during the period of mandibular growth. It is more
common in females. It may be an incidental finding
in a panoramic projection, or the patient may have
mandibular asymmetry, signs and symptoms of TMj
dvsfunction. or both.
Radiographic Features
The condylar head develops a characteristic "toadstool"
appearance, with marked flattening and apparent
elongation of the articulating condylar surface and
dorsal (posterior) inclination of the condyle and
neck. The condylar neck is shortened or even absent in
some cases, with the condyle resting on the upper
margin of the ramus (Fig. 25-18). The articulating
surface of the temporal component often is flattened.
Progressive shortening of the ramus occurs on the
affected side, and the antegonial notch may be deepened, indicating mandibular hypoplasia. In longstanding cases, superimposed degenerative changes
may be present.
Differential Diagnosis
The radiographic appearance of juvenile arthrosis may
be very similar to, and in some casesis indistinguish-
able from, developmental hypoplasia of the condyle.
Destruction of the anterior aspectof the condylar head
from rheumatoid arthritis and severedegenerativejoint
disease or severe condylar degeneration after orthognathic surgery or joint surgery also may simulate juvenilp
~rthrn~i~
Treatment
Orthognathic surgery and orthodontic therapy may be
required to correct the mandibular asymmetry.Caution
should be exercised in undertaking orthodontic
therapy becausestresson the joint may result in, further
degeneration and orthodontic relapse.
CORONOID
HYPERPLASIA
Definition
Coronoid processhyperplasia maybe acquired or developmental, resulting in elongation of the coronoid
process. In the developmental variant, the condition
usually is bilateral. Acquired types may be unilateral
or bilateral and usually are a response to restricted
condylar movement caused by abnormalities such as
ankvlosis.
Clinical Features
Bilateral developmental coronoid hyperplasia is more
common in males, often commencing at the onset of
puberty, although the condition was reported in a 3year-olc;i.Patients complain of a progressive inability to
open the mouth and may have an apparent closed lock.
The condition is painless.
Radiographic Features
Coronoid hyperplasia is best seen in panoramic,
Waters', and lateral tomographic views and on CT
FIG. 25-18
Juvenile arthrosis. The condylar heads have a "toadstool" appearance and
are posteriorly inclined. The condylar necks are absent.
554
PART V
RADIOGRAI?HIC
INTERI?RETATION
OF I?ATHOLOGY
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
scans.The coronoid processesare elongated, and the
tips extend at least 1 cm above the inferior rim of the
zygomatic arch (Fig. 25-19). As a result, the coronoid
processesmay impinge on the medial surface of the
zygomatic arch during opening, restricting condylar
translation. The coronoid processesmay have a large
but normal shape or may curve anteriorly and may
appear very radiopaque. The posterior surface of the
zygomatic processof the maxilla may be remodeled to
accommodate the enlarged coronoid process during
function. The radiographic appearance of the TMJs
usually is normal:
Differential Diagnosis
Unilateral casesshould be differentiated from a tumor
of the coronoid process such as an osteochondroma or
osteoma. Unlike coronoid hyperplasia, tumors usually
have an irregular shape. The differential diagnosis
also includes any causeof inability to open, such as soft
tissue abnormalities and ankylosis, emphasizing the
importance of including the coronoid process in
imagesof the TMJs. An axial CT image with the patient
in a wide-open position is useful in establishing coronoid interference to opening.
Treatment
Treatment consistsof osteotomy or surgical removal of
the coronoid process and postoperative physiotherapy.
BIFID CONDYLE
Definition
A bifid condyle has a vertical depression, notch, or deep
cleft in the center of the condylar head seen in the
frontal or sagittal plane or an actual duplication of the
condyle, resulting in the appearance of a "double" or
"bifid" condylar head. This condition may be unilateral
or bilateral. It may result from an obstructed blood
-supply or other embryopathy, although a traumatic
cause has been postulated as a result of a longitudinal
linear fracture of the condyle.
Clinical Features
Bifid condyle usually is an incidental finding in
panoramic views or anteroposterior projections. Some
patients have signs and symptoms of temporomandibular dysfunction, including joint noises and
pain.
Radiographic Features
A depression or notch is present on the superior condylar surface,giving the anteroposterior silhouette a heart
shape; in more severecasesa duplicate condylar head
is present in the mediolateral plane (Fig. 25-20). The
mandibular fossa may remodel to accommodate the
altered condylar morphology.
Differential Diagnosis
A slight medial depressioh on the superior condylar
surface maybe considered a normal variation; the point
at which the depth of the depression signifies a bifid
condyle is unclear. The differential diagnosis also
includes a vertical fracture through the condylar head.
Treatment
Treatment is not indicated unless pain or functional
impairment is present.
Soft Tissue Abnormalities
INTERNAL
FIG. 25-19
Coronoid hyperplasia (sagittal tomogram).
The coronoid process is elongated and extends above the
inferior rim of the zygomatic arch (arrow) but otherwise is
shaped normally.
DERANGEMENTS
Definition
An internal derangement is an abnormality in the position and sometimes the morphology of the articular
disk that may interfere with normal function. The disk
most often is displaced in an anterior direction, but it
may be displaced anteromedially, medially, or anterolaterally. Lateral and posterior displacements are
extremely rare. Some hypothesize that disk displacements may be considered a normal variation based on
the frequency of this finding in asymptomatic patients.
The cause of internal derangements is unknown,
~
CHAPTER
DIAGNOSTIC
25
IMAGING
OF THE TEMPOROMANDIBULAR
555
JOINT
Simpo PDF Merge and Split Unregistered Version - http://www.simpopdf.com
~
A
FIG. 25-20
Bifid condyle. A, Sagittal tomogram showing a deep central notch with
duplication of the condylar head (arrows). The glenoid fossa has remodeled (enlarged) to
accommodate
thecenter
abnormal
condyle.
B, Coronal
depression in the
of the
condylar
head. tomogram. Another example. showing a
although parafunction, jaw injuries (e.g., dIrect
trauma), whiplash injury, and forced opening beyond
the normal range have been implicated.
Internal derangements can be diagnosed using
either arthrography or MR!. In some instances the disk
may resume a normal position with respect to the
condyle (called redu'ctiona/the disk)during mandibular
opening; when the disk remains displaced throughout
the entire range of mandibular movement, the term
nonreductionis used (Fig. 25-21). A chronically displaced
disk may become deformed, losing its normal biconcave shape,and it may become thickened and fibrotic.
Possible complications in long-standing chronic disk
displacement are degenerative joint disease and per"
foration through the disk or (more commonly) the
posterior attachment.
Clinical
Features
Disk displacement has been found both in symptomatic
patients and in healthy volunteers, suggesting that it
may be a normal variant and not necessarilya predisposing factor in TMJ dysfunction. It is not known why
some disks remain displaced or why symptoms of pain
and dysfunction are not found in all affected patients.
Symptomatic patients may have a decreased range of
mandibular motion. Internal derangements can be unilateral or bilateral; unilateral casesmay manifest clinically as mandibular deviation to the affected side on
opening. Joint noises are common and may manifest as
a click as the disk reduces to a normal position during
mandibular opening and occasionally as a softer click
as the disk becomes dIsplaced agam dUrIng manaIDular closing. Noises may be absent in chronically displaced, nonreducing disks, or crepitus may be heard.
Patients may complain of pain in the preauricular
region or headaches and may have episodes of closed
or open locking of the joint. Patients may have to
manipl,llate the mandible to open it fully past an apparent closed lock by applying medially directed pressure
to the affected joint or mandible with the hand.
Kaoiograpnlc
t-eatures
The disk cannot be visualized with conventional radiography or tomography; arthrography and MRI are the
techniques of choice. Although a retruded condylar
position has been associated with disk displacement,
condylar position in maximal intercuspation is not a
reliable indicator of disk displacement. Likewise,diminished range of motion at maximal opening is not a reliable indication of a nonreducing disk.
DISk Displacement
Identifying the disk may be difficult in casesof gross
deformation of the disk and other soft tissue components. Anterior displacement is the most common disk
displacement. When the mandible is in maximal intercuspation, partial or full anterior disk displacement is
indicated by anterior location of the posterior band of
the disk from the normal position, which is directly
superior to the condylar head. The normal articulating
surface of the disk (thin intermediate zone) is somewhat anteriorly positioned, and as a re~ult the osseous