Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
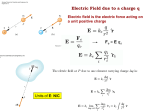
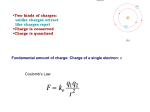
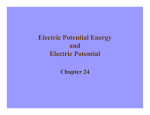
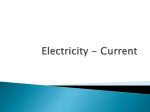
Attachment B: (MAP Program Plan) Handbook for the Travis County Healthcare District MEDICAL ASSISTANCE PROGRAM (MAP) SUBROGATION Subrogation is the right to recover amounts paid by a government-sponsored plan that are the obligation of other payers (such as an insurance company). If you are injured or become ill under circumstances in which a third party may legally be obligated to pay the medical, dental and/or pharmacy expenses, MAP will pay your covered expenses. MAP reserves the right, however, to be reimbursed for all medical expenses from the settlement or judgment made by the third party. EXCLUSIONS Services and related items excluded from coverage by the Medical Assistance Program (MAP) include but are not limited to the following list. MAP does not cover items on this list. 1. Services or supplies not specifically covered by the Medical Assistance Program; 2. All services that have been denied through pre-authorization by the Medical Assistance Program; 3. Services not provided within the MAP designated network, unless pre-authorized; 4. Services, supplies and equipment provided or primarily utilized outside the boundaries of Travis County unless provided under an agreement between the Travis County Healthcare District and the provider; 5. Services and supplies for persons whose primary residence is outside the boundaries of Travis County; 6. Services, supplies or equipment provided without active MAP coverage; 7. Services and supplies to any individual who is a resident or inmate in a public institution; 8. In-patient hospital and related services for a patient in an institution for tuberculosis, mental disease, or a nursing section of a public institution for the mentally retarded; 9. Services provided for any work-related illness, injury or complication thereof arising out of the course of employment for which Worker's Compensation Benefits or any other similar regulation of the United States are provided or should be provided according to the laws of the state, territory or subdivision thereof governing the employer under which such illness or injury occurred; 10. Services or supplies provided in connection with cosmetic surgery except as required for the repair of accidental injury if the initial treatment is received within 12 months of the accident in which the injury was sustained, or for improvement of the functioning of a malformed body member, or when prior authorization is obtained for other medically necessary purposes; 11. Services, supplies and medications for which benefits are available under a manufacturer’s Patient Benefit Program, or any other contract policy or insurance which would have been available in the absence of the Medical Assistance Program; 12. Services payable by any health, accident, or other insurance coverage; or by any private or other governmental benefit system, or any legally liable third party; 13. Services, supplies or medications considered experimental or investigational, i.e., services and items which have not been approved for marketing by the Food and Drug Administration Services; The Medical Assistance Program serves the healthcare needs of eligible residents in Travis County and is funded by the Travis County Healthcare District. Exclusions Page 1 – Revised 01/02/2009 Page 1 of 8 Attachment B: (MAP Program Plan) Handbook for the Travis County Healthcare District MEDICAL ASSISTANCE PROGRAM (MAP) 14. Supplies or medication related to infertility; 15. Any services to include, but not be limited to, drugs, surgery, medical or psychiatric care or treatment for transsexualism, gender dysphoria, sexual re-assignment or sex change; 16. Procedures that relate to obesity, obesity therapy and/or special diets (including medically supervised fasting and liquid nutrition) related to weight reduction whether necessitated by surgery or a specifically identified medical condition; 17. Services provided by an interpreter; 18. Services provided by a relative of the enrollee or a member of his or her household; 19. Services and supplies that are provided under any governmental plan or law under which the individual is or could be covered (e.g., Victims of Crime, Texas Rehabilitation Commission, Veteran's Benefits, Medicare, Medicaid, TRICARE, CHAMPUS, etc.); 20. Co-insurance fees and deductibles. MAP is not a secondary payer for any other insurance or governmental health care program; 21. Charges for services not medically necessary, which are not incident to and necessary for the treatment of an injury or illness; 22. Charges for acute hospital services and supplies provided as an inpatient to the extent that it is established upon review of the claim submitted that the enrollee’s condition did not require a hospital level of care and could have been provided safely at a lesser level of care; 23. Charges for hospital care and services rendered after the patient has been discharged from the hospital by the attending physician, or for hospital care and services when a registered bed patient is absent from the hospital; 24. Charges resulting from or in connection with the commission of any illegal act, occupation or event (including the commission of a crime or violation of conditions of probation) if the covered individual is incarcerated; 25. Charges resulting from or in connection with any acts of war, declared or undeclared, or any type of military conflict, charges incurred due to diseases contracted or injuries sustained in any country while such country is at war or while en route to or from any such country at war, charges resulting from illness/injuries incurred while engaged in military services; 26. Inpatient and outpatient comprehensive rehabilitation; 27. Charges for custodial or sanitaria care, rest cures, or for respite care; 28. Charges for care and treatment of mental and/or nervous disorders, psychiatric treatment or individual, family, or group counseling services unless as a co-morbidity or secondary diagnosis during an inpatient stay; 29. Charges for treatment programs for substance abuse and/or detoxification. (Note: Even though this is not a MAP-covered service, you may ask the staff for low cost or free resources in the community if you need substance abuse treatment and/or detoxification.) 30. Charges that related to in-born errors of metabolism; 31. Charges for air ambulance; 32. Charges for private room except when appropriate documentation of medical necessity is provided; The Medical Assistance Program serves the healthcare needs of eligible residents in Travis County and is funded by the Travis County Healthcare District. Exclusions Page 2 – Revised 01/02/2009 Page 2 of 8 Attachment B: (MAP Program Plan) Handbook for the Travis County Healthcare District MEDICAL ASSISTANCE PROGRAM (MAP) 33. Charges for Chiropractic services/treatment; 34. Charges for Rolfing; 35. Charges for acupuncture, acupressure, or biofeedback; 36. Charges for services rendered by a massage therapist; 37. Charges for hypnosis; 38. Charges for eye refractions, eye glasses, eye exercises, contact lenses, or other corrective devices, including materials and supplies, or for the fitting or examinations for prescribing, fitting or changing of these items; 39. Charges for whole blood or packed red cells that are available at no cost to the client; 40. Charges for autologous blood donations; 41. Charges for blood clotting factors; 42. Charges for luxury/entertainment items (e.g., TV, video, beauty aids, etc.); 43. Charges/fees for completing or filing required forms/pre-authorizations; 44. Charges which accumulate during any period of time in which the client removes rental equipment from the delivery site and fails to immediately notify the Medical Assistance Programs of the new location; 45. Autopsies; 46. Cellular Therapy; 47. Chemolase injections (Chemodiactin, Chymopapain); 48. Chemonucleolysis intervertebral disc; 49. Cognitive therapy; 50. Dermabrasion; 51. Dialysis (in-patient or out-patient) or supplies related to dialysis, except for acute conditions not related to chronic renal failure while in the inpatient setting; 52. Educational counseling; 53. Ergonovine provocation test; 54. Fabric wrapping of abdominal aneurysms; 55. Hair analysis; 56. Histamine therapy - intravenous; 57. Hospice care; 58. Hyperactivity testing; 59. Hyperthermia; 60. Immunotherapy for malignant disease; 61. Immunizations required for travel outside the United States; The Medical Assistance Program serves the healthcare needs of eligible residents in Travis County and is funded by the Travis County Healthcare District. Exclusions Page 3 – Revised 01/02/2009 Page 3 of 8 Attachment B: (MAP Program Plan) Handbook for the Travis County Healthcare District MEDICAL ASSISTANCE PROGRAM (MAP) 62. Implantations (e.g., silicone, saline, penile, etc.); 63. Joint sclerotherapy; 64. Laetrile therapy; 65. Organ transplants, medications and/or treatments associated with the transplant; 66. Orthodontic treatment, crown, and bridge procedures; 67. Specialized pain management programs and/or treatment designed to provide chronic pain care unless provided through the CHC setting; 68. Penile prosthesis; 69. Prosthetic eye or facial quarter; 70. Radial and hexagonal keratotomy or refractive surgeries; keratoprosthesis/refractive keratoplasty; 71. Routine circumcision for clients one year of age or older; 72. Sterilization reversal; 73. Tattooing and/or tattoo removal; 74. Thermogram; 75. TORCH screen; 76. Adaptive equipment for daily living such as eating utensils, reachers, handheld shower extensions, etc.; 77. Admission kits; 78. Air cleaners/purifiers; 79. Any equipment, supplements, or supplies not ordered by a physician or provider and/or considered appropriate and necessary to treat a documented medical condition/disease process; 80. Augmentive communication devices, e.g., TTY device, artificial voice box, and machinery of this nature; 81. Bed cradles; 82. Bladder stimulators (pacemakers); 83. Car seats; 84. Cervical pillows; 85. Electric wheelchairs or scooters (outpatient); 86. Enuresis monitors; 87. Equipment or services not primarily and customarily used to serve a medical purpose (e.g., an air conditioner might be used to lower room temperature to reduce fluid loss in a cardiac patient or a whirlpool bath might be used in the treatment of osteoarthritis, however because the primary and customary use of these items is a non-medical one, they cannot be considered as medical equipment); 88. Evaluations for learning disabilities; The Medical Assistance Program serves the healthcare needs of eligible residents in Travis County and is funded by the Travis County Healthcare District. Exclusions Page 4 – Revised 01/02/2009 Page 4 of 8 Attachment B: (MAP Program Plan) Handbook for the Travis County Healthcare District MEDICAL ASSISTANCE PROGRAM (MAP) 89. Feeding supplements (e.g., Ensure, Osmolyte) and supplies for long-term use; 90. Hearing aids; 91. Home and vehicle modifications, including ramps, tub rails/bars; 92. Humidifiers, except when used with respiratory equipment (e.g., oxygen concentrators, CPAP/BIPAP, nebulizers, or for clients with a tracheostomy (requires pre-authorization); 93. Implantable medication pumps and related supplies; 94. Over bed tables; 95. Prosthetic breasts and mastectomy bras; 96. Thermometers; 97. Vocational, educational, exercise, and recreational equipment; 98. Waist/gait belts; 99. Whirlpool baths and saunas; 100. Treatment or correction of temporomandibular joint (TMJ) dysfunction; 101. Refills or prescriptions in excess of the number specified by the Doctor, or refills dispensed one year or more after the date of the Doctor’s original order. The Medical Assistance Program serves the healthcare needs of eligible residents in Travis County and is funded by the Travis County Healthcare District. Exclusions Page 5 – Revised 01/02/2009 Page 5 of 8 Attachment B: CommUnityCare Plan Table 1: Demographic Information (Unduplicated Patients) October 2007-September 2008 Demographic Information Gender Total MAP and CommUnityCare Number Female Male Total Age Group 17 and younger 18-24 25-34 35-44 45-54 55-64 65+ Total Ethnicity African American Anglo Asian Hispanic Native American Other Total Page 6 of 8 Percent of Total 36,343 30,390 66,733 (54.5%) (45.5%) 100% 11,995 9,487 18,956 12,275 8,507 4,424 1,089 66,733 (18.0%) (14.2%) (28.4%) (18.4%) (12.7%) (6.6%) (1.6%) (100.0%) 4,810 6,889 942 52,448 31 1,613 66,733 (7.2%) (10.3%) (1.4%) (78.6%) (0.05%) (2.4%) (100.0%) Attachment B: CommUnityCare Plan Table 2: Net Paid Claims by Zip Code (MAP and CommUnityCare Lines of Business) October 2007-September 2008 ZIP 78745 78768 78741 78744 78753 78702 78660 78767 78704 78758 78723 78724 78617 78721 78752 78748 78653 78728 78701 78747 78757 78749 78759 78645 78734 78727 78641 78751 78756 78754 78735 78736 78669 78610 78719 78725 78722 blank 78703 78731 78733 78621 78726 78652 78664 78612 78729 MAP net paid claims 6,596 6,155 5,979 5,473 5,392 5,298 4,221 4,097 4,024 3,786 3,221 2,922 2,810 2,442 2,342 1,996 1,448 1,209 1,167 1,110 1,098 1,054 1,036 991 958 916 603 574 537 528 432 418 403 402 368 360 354 287 251 241 238 210 201 177 173 159 146 ZIP 78746 78705 78738 78750 78742 78739 78737 78620 78760 78730 78642 78644 78715 78640 78761 78732 78615 78764 78755 76530 78654 78711 78613 78646 78655 78681 78766 78133 78680 78709 78740 78763 78219 78616 78634 78639 78716 78717 78155 78718 78765 78942 77566 78602 78614 78708 78957 Grand Total MAP net paid claims 146 145 142 135 130 117 112 85 73 55 50 44 39 38 38 35 31 28 25 23 19 19 18 18 17 12 10 8 8 5 4 4 3 3 3 3 3 3 2 2 2 2 1 1 1 1 1 86,467 ZIP 78744 78741 78753 78745 78758 78723 78660 78724 78704 78752 78702 78617 78721 78748 78747 78757 78727 78653 78754 78751 78728 78734 78736 78735 78645 78759 78725 78749 78621 78719 78669 78733 78722 78742 78641 78767 Page 7 of 8 CommUnityCare line of business net paid claims ZIP 3901 78746 3879 78737 3724 blank 2781 78756 2588 78644 2226 78701 1862 78703 1753 78739 1738 78705 1738 78664 1613 78750 1499 78768 1134 78729 846 78610 598 78613 567 78654 441 78652 424 78726 416 78731 412 78612 411 78711 349 78615 302 78616 301 78715 291 78732 287 78730 266 78709 258 78681 249 78761 188 78602 135 78691 127 78620 119 78707 104 78764 101 78766 101 Grand Total CommUnityCare line of business net paid claims 96 89 88 70 68 65 65 63 56 55 50 49 47 44 38 38 36 35 33 28 24 20 16 15 14 7 6 5 5 4 4 3 1 1 1 38,968 Attachment B: CommUnityCare Plan CommUnityCare’s program plan is the 340B Drug Pricing Program, administered by the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA) – Office of Pharmacy Affairs (OPA). Program details may be found at http://www.hrsa.gov/opa Page 8 of 8