Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
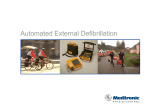
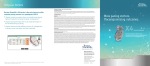
Optisure™ Defibrillation leads Models LDA220, LDA230, LDA210, LDA220Q, LDA230Q, LDA210Q, LDP220, LDP230, LDP220Q, LDP230Q, LDP210Q User's Manual Unless otherwise noted, ™ indicates that the name is a trademark of, or licensed to, St. Jude Medical or one of its subsidiaries. ST. JUDE MEDICAL and the nine-squares symbol are trademarks and service marks of St. Jude Medical, Inc. and its related companies. © 2015 St. Jude Medical, Inc. All Rights Reserved. Description Optisure™ Models LDA220, LDA230, LDA210, LDA220Q, LDA230Q, LDA210Q, LDP220, LDP230, LDP220Q, LDP230Q, and LDP210Q transvenous tachyarrhythmia leads are steroid-eluting, active or passive fixation leads, and are designed for long-term attachment to an implantable cardioverter defibrillator (ICD). All leads have two defibrillation electrodes except for models LDA210, LDA210Q, and LDP210Q which have one. The leads provide true bipolar rate-sensing, pacing, and delivery of cardioversion/defibrillation shocks. Certain Optisure models and lead lengths have been tested for use in the MRI environment and are designated MR Conditional. See MR Conditional ICD System (page 5). All models are designed for implantation with the distal tip positioned in the right ventricle. For models LDA220, LDA230, LDA210, LDA220Q, LDA230Q, and LDA210Q, the tip incorporates an extendable/retractable helix for fixation in the ventricle. The retractable helix allows the electrical testing of possible lead positions prior to advancement of the fixation helix. The design of the tip aids visibility under fluoroscopy. For models LDP220, LDP230, LDP220Q, LDP230Q, and LDP210Q, the tip of the lead has tines for fixation in the ventricle. The low profile, flat-wire defibrillation electrodes with silicone rubber backfilling are intended to preclude tissue ingrowth. Models LDA220, LDA230, LDA220Q, LDA230Q, LDP220, LDP230, LDP220Q, and LDP230Q are quadripolar leads and models LDA210, LDA210Q, and LDP210Q are tripolar leads. Portions of the lead body have an Optim™ (silicone polyurethane copolymer) insulation overlay. The lead body insulation tubing is Optim™ insulation and silicone rubber for longterm biocompatibility and biostability. The lead body is treated with Fast-Pass™ coating to provide lubricity during lead implant. After contact with body fluid, the tip electrode elutes an amount less than 1.0 milligram of dexamethasone sodium phosphate (DSP), a steroid. This minimizes tissue inflammation, which, in turn, is intended to reduce both acute and chronic pacing thresholds. For information on the specifications of any lead model, refer to the following tables. Figure 1. Nominal dimensions of DF4-LLHH lead connector (mm) 1. 2. 3. 4. RV tip RV ring RV coil SVC coil Table 1. Active fixation lead technical specifications Length (cm) LDA220 LDA230 LDA210 LDA220Q 60, 65, 75 52, 58, 65 1 LDA230Q LDA210Q Table 1. Active fixation lead technical specifications LDA220 LDA230 LDA210 Lead introducer (Fr) 8 Electrode configuration: helix Tip electrode Ring electrode cylindrical Defibrillation electrode Electrode spacing: trifilar coil Tip to ring electrode (mm) 11 Tip to distal defibrillation electrode (mm) 17 Tip to proximal defibrillation electrode (cm) Connector type 1 17 Sense/pace Defibrillation Sense/pace/ defibrillation Materials 2 21 n/a LDA220Q LDA230Q LDA210Q 17 21 n/a DF4LLHH DF4LLHO 1 IS-1 bipolar (3.2 mm) n/a connector 2 DF-1 unipolar 1 DF-1 n/a (3.2 mm) unipolar(3.2 connectors mm) connector n/a DF4LLHH Body Fast-Pass™ Conductors 35N LT and 35N LT DFT Connectors MP35N and stainless steel Insulators silicone rubber, Optim™, ETFE, and PTFE Defibrillation electrodes platinum iridium alloy Pacing electrode (helix) titanium nitride-coated platinum iridium alloy MP35N DSP Steroid-eluting plug Electrode surface area (mm2): 6 Pacing tip Pacing ring 17 1 St. Jude Medical IS-1 lead connectors conform to the international connector standard ISO 5841-3. St. Jude Medical DF-1 lead connectors conform to the international connector standard ISO 11318/Amd. 1. MP35N is a trademark of SPS Technologies. 35N LT and 35N LT DFT are registered trademarks of Fort Wayne Metals. 2 2 Table 1. Active fixation lead technical specifications Distal defibrillation Proximal defibrillation Electrode length: Pacing tip (mm) LDA220 LDA230 LDA210 367 LDA220Q LDA230Q LDA210Q 638 638 n/a 638 638 n/a 8 n/a 8 8 n/a 1.80 Pacing ring (mm) 2.79 5 Distal defibrillation (cm) 8 Proximal defibrillation (cm) Electrical resistance (Ω): 60 cm: 17 Pace 65 cm: 18 75 cm: 21 15 Sense Defibrillation Maximum diameter (mm) Maximum helix revolutions 52 cm: 15 58 cm: 17 65 cm: 19 <6 <6 2.54 at defibrillation electrodes 20 Table 2. Passive fixation lead technical specifications LDP220 Length (cm) Lead introducer (Fr) Electrode configuration: LDP230 60,65,75 8 semispherical shape Ring electrode cylindrical Tip to ring electrode (mm) LDP230Q LDP210Q 52,58,65 Tip electrode Defibrillation electrode Electrode spacing: LDP220Q trifilar coil 11 Tip to distal defibrillation 17 electrode (mm) 17 Tip to proximal defibrillation electrode (cm) 21 17 3 21 n/a Table 2. Passive fixation lead technical specifications LDP220 LDP230 LDP220Q LDP230Q LDP210Q Connector type 3 1 IS-1 bipolar(3.2 mm) connector 2 DF-1 unipolar(3.2 Defibrillation mm) connectors Sense/pace/defibrillation n/a Sense/pace n/a n/a DF4-LLHH DF4LLHH DF4-LLHO Materials 4 Body Fast-Pass™ Conductors 35N LT and 35N LT DFT Connectors Insulators MP35N and stainless MP35N steel silicone rubber, Optim™, ETFE, and PTFE Defibrillation electrodes platinum iridium alloy Pacing electrode titanium nitride-coated platinum iridium alloy dexamethasone sodium phosphate Steroid-eluting plug Electrode surface area (mm2): 3.5 Pacing tip Pacing ring 17 Distal defibrillation 367 Proximal defibrillation Electrode length: 638 Pacing tip (mm) 0.45 Pacing ring (mm) 2.41 Distal defibrillation (cm) 5 Proximal defibrillation (cm) Electrical resistance (Ω): Pace Sense Defibrillation Maximum diameter (mm) 8 638 638 638 n/a 8 8 8 n/a 60 cm: 33 65 cm: 36 75 cm: 42 15 52 cm: 29 58 cm: 32 65 cm: 36 <6 <6 2.54 at defibrillation electrodes 3 St. Jude Medical IS-1 lead connectors conform to the international connector standard ISO 5841-3. St. Jude Medical DF-1 lead connectors conform to the international connector standard ISO 11318/Amd. 1. 4 MP35N is a trademark of SPS Technologies. 35N LT and 35N LT DFT are registered trademarks of Fort Wayne Metals. 4 Indications The Optisure™ Models LDA220, LDA230, LDA210, LDA220Q, LDA230Q, LDA210Q, LDP220, LDP230, LDP220Q, LDP230Q, and LDP21OQ transvenous leads are indicated for use with compatible pulse generators (refer to the applicable defibrillator manual for system indications). They provide pacing and sensing and deliver cardioversion/defibrillation therapy to the heart. A transvenous lead system may offer the patient the benefit of avoiding a thoracotomy for lead implantation. If the initial lead configuration is not effective, repositioning of the lead or other lead configurations should be attempted. In some patients, a nonthoracotomy lead configuration may not provide reliable conversion of arrhythmias, and the use of subcutaneous or epicardial patch defibrillation leads should be considered. Table 3. Accessories and their intended uses Accessory Intended use Insulate and protect the lead connector when it is not connected to a device. Stylet Stiffen and support the lead to facilitate placement. Protect the lead from damage when it is secured to the Suture sleeve venous entry site. Vein pick Lift and dilate the vein at the lead entry site. Stylet guide (funnel, IS-1 models Assist the insertion of the stylet into the lead connector pin only) to facilitate placement. Clip-on tool Extend and retract the helix of an active-fixation lead. DF-1 plug (single coil model Seal unused lead receptacles. only) Provide a safe and secure connection and disconnection IS4/DF4 connector sleeve to the lead. Lead cap Contraindications Contraindications for use of the Optisure™ leads with an implantable pulse generator include ventricular tachyarrhythmias resulting from transient or reversible factors such as drug toxicity, electrolyte imbalance, or acute myocardial infarction. Transvenous lead systems are contraindicated for patients with tricuspid valvular disease or a mechanical heart valve. Optisure™ leads are contraindicated for patients for whom a single dose of 1.0 mg of dexamethasone sodium phosphate is contraindicated. Optisure™ leads are contraindicated for use with extra firm (red color knob) stylets for active fixation lead models. The lead is not designed, sold, or intended for use other than as indicated. MR Conditional ICD System The St. Jude Medical™ MR Conditional lead is part of the St. Jude Medical MR Conditional ICD system. An MR Conditional lead is conditionally safe for use in the MRI environment when used in a complete MR Conditional ICD system and according to the instructions in the MRI Procedure 5 Information document for the St. Jude Medical™ MR Conditional ICD System. Patients with an implanted St. Jude Medical MR Conditional ICD system can have an MRI scan if the conditions for use, as described in the MRI Procedure Information document, are met. The following models and lead lengths have been tested and determined to be MR Conditional when used according to the instructions in the MRI Procedure Information document. Models and lead lengths marked not listed in the table below have not been tested and their use in an MR environment is not determined. Table 4. MR Conditional models and lead lengths for Optisure leads Model LDA210Q LDA210Q LDA220Q LDA220Q Lead Length 58 65 58 65 MR Status MR Conditional MR Conditional MR Conditional MR Conditional Warnings and Precautions Testing has demonstrated that the St. Jude Medical™ MR Conditional ICD system is conditionally safe for use in the MRI environment when used according to the instructions in the MRI Procedure Information document. Models and lead lengths not listed in the table MR Conditional ICD System (page 5) have not been tested and its use in an MR environment is not determined. Package Contents The lead is packaged separately and supplied sterile. Packages contain: 1 lead with stylet and suture sleeve in place 1 vein pick 2 clip-on tools (active fixation models only) Stylets of varying firmness 1 stylet guide (funnel, IS-1 models only) 1 DF-1 plug (single coil model only) Product documentation IS4/DF4 connector sleeve Storage The lead should be stored at room temperature. Permitted storage temperatures are between -5°C (23°F) and +50°C (122°F). Potential Adverse Events Possible complications of the use of transvenous lead systems include, but are not limited to, supraventricular or ventricular arrhythmias, conduction disturbances, cardiac perforation, cardiac tamponade, loss of contractility, air embolism, heart wall rupture, myocarditis, postoperative heart failure, chronic mechanical stimulation of the heart, tricuspid valve dysfunction, lead fracture necessitating surgical removal, pneumothorax, hemothorax, 6 infection, tissue necrosis, and erosion of the skin. Specific events and effects are summarized in the following table. WARNING Implanted cardiac leads are subjected to a hostile environment within the body due to constant, complex flexural and torsional forces, interactions with leads and/or the pulse generator, or other forces associated with cardiac contractions and patient physical activity, posture, and anatomical influences. Cardiac leads’ functional lifetimes can be affected by these and other factors. Refer to the defibrillator manual for additional system complications and precautions as well as those specific to the pulse generator. Table 5. Potential Adverse Events Event Dislodgement, breaching of the lead insulation, connector fracture, poor connection to the pulse generator, electrode fracture, or conductor discontinuity. Cardiac perforation Venous perforation Myocardial irritability Transvenous implantation procedure Chronic implantation Contamination Post-shock rhythm disturbances Threshold elevation or exit block Shunting or insulating of current during defibrillation with internal or external paddles Possible Effects Intermittent or continuous loss of sensing, possibly resulting in nondetection of arrhythmia; oversensing of artifact, possibly causing inappropriate delivery of therapy from the pulse generator; intermittent or continuous loss of defibrillation, cardioversion, or pacing therapy; possible muscle or nerve stimulation in the pocket area; intermittent or continuous loss of cardioversion/defibrillation therapy, sensing, or pacing therapies. Intermittent or continuous loss of sensing, cardiac tamponade, or hemorrhage Acute hemorrhage (may not be readily apparent), or cardiac tamponade Premature ventricular contractions, supraventricular and ventricular tachyarrhythmias Air embolism Venous thrombosis and/or obstruction Infection requiring removal of lead system, pulse generator, or both Post-shock bradycardia or supraventricular arrhythmias Loss of efficacy of defibrillation, cardioversion, or pacing therapy Increased external defibrillation energy and/or repositioning of paddles required Instructions for Use Required Equipment Equipment for cardiac monitoring, fluoroscopic imaging, external defibrillation, and measuring lead signals should be available for immediate use during lead implantation and 7 tachyarrhythmia induction testing. Additional quantities of all sterile implantable devices should be available in case of accidental contamination or damage. Package Inspection St. Jude Medical packages all leads under clean conditions and sterilizes them using ethylene oxide gas before shipment. If the lead package and seal are intact, the lead and accompanying components are ready to use. Inspect the package carefully before opening and check the “Use Before” date on the product label. Verify that the sterility indicator on the inner package is not purple. Purple indicates that the package has not been sterilized. Do not use the lead if there appears to be damage to the package or the lead. If the package is wet, damaged, or punctured, or if the seal is broken, contact St. Jude Medical. St. Jude Medical does not recommend use of the product after its expiration date. If the lead package has been breached outside a sterile field or the expiration date has passed, contact St. Jude Medical. Sterilization The package contents have been sterilized with ethylene oxide before shipment. This lead is for single use only and is not intended to be resterilized. If the sterile package has been compromised, contact St. Jude Medical. Handling the Lead Use caution when handling the lead. It is designed to be pliable, but it will not tolerate excessive bending or stretching. Permanent damage to the lead may result from severe bending, kinking, or stretching, or from excessive manipulation with surgical instruments. Never apply pressure to the lead with a surgical instrument, such as a hemostat. Do not try to alter electrodes or apply pressure to the tips of electrodes. Avoid contact of the electrode with a hard surface and guard against contaminating the lead tip with insulating materials such as lubricants or medical adhesive. Use powderless surgical gloves or be sure that talc has been removed from surgical gloves before handling the lead. Because lead insulation attracts particulate matter such as lint and dust, minimize contamination by protecting the lead from materials that shed such particles. Do not immerse the helix electrode in liquid or wipe it with any liquid as this will reduce the amount of DSP eluted after implantation. Implantation Procedure Implantation of a transvenous lead generally involves: Selecting, isolating, and opening the desired vein. Inserting the lead using the vein pick and stylets. Positioning and securing the lead. Testing the sensing, pacing, and cardioversion/defibrillation functions of the lead. Suturing the lead in place. Connecting the lead to the pulse generator Techniques for implantation vary among physicians and depend on the patient's anatomy and physical condition. The following description presents a typical technique; other methods may also be applicable. CAUTION If using a percutaneous lead introducer with a hemostasis valve, make 8 sure the valve allows for appropriate passage of the lead without damaging the lead body. To avoid distortion of the Optisure™ lead tip, do not use a St. Jude Medical™ Seal-Away™ hemostasis valve. Stylet Guide (Funnel, IS-1 models only) Use the stylet guide (funnel) to assist the insertion of a stylet into the lead's IS-1 connector pin. Insert the stylet guide over the IS-1 connector pin prior to introducing the stylet. Preparing the Active Fixation Lead Test the extension and retraction of the helix before implanting the lead. 1. Insert a stylet into the lead, if necessary. Verify that the stylet is fully inserted. 2. Straighten the lead on a flat surface. 3. Pinch the clip-on tool open and insert the connector pin into the first notch. For DF4 leads only, place the clip-on tool on the larger diameter surface of the connector pin. For all leads, make sure the clip-on tool remains in this position on the connector pin when you rotate the clip-on tool to extend the helix and release the handles of the tool so that it grasps the connector pin firmly. 4. While keeping the lead as straight as possible, grasp the connector boot with one hand and with the other hand, rotate the clip-on tool clockwise to extend the helix. (Refer to the Technical Specifications tables for the number of rotations required to extend the helix.) The helix is fully extended when at least 2 turns are visible beyond the lead tip. 5. 6. CAUTION While extending or retracting the helix: Keep the lead as straight as possible. Bending or kinking the lead body may interfere with the helix movement or cause damage to the lead. Do not grasp the lead body. Doing so may interfere with the helix movement or cause damage to the lead. Rotate the clip-on tool counter-clockwise to retract the helix. CAUTION Do not further rotate the connector pin after the helix is fully extended or retracted. Doing so may damage the helix mechanism. To remove the clip-on tool, pinch the handles and withdraw the connector pin from the tool. Selecting and Opening a Vein The suggested entry site is the left cephalic vein entered through a venous cutdown. Alternatively, the lead may be implanted percutaneously through the left subclavian vein.If a percutaneous subclavian entry is chosen, the puncture site should be as lateral as possible (in the area under the lateral two-thirds of the clavicle, lateral to the subclavius muscle). The right subclavian vein and the internal jugular vein can also be used. Inserting the Lead A vein pick included in the package is intended to aid in inserting the lead into the vein. Its use is optional and depends on the chosen implantation technique. To use the vein pick, first isolate and open the selected vein with scissors or a scalpel. Orient the point of the vein pick in the direction the lead will be passed and insert the point through the incision into the vessel lumen. Raise and tilt the vein pick gently, and pass the lead under the pick into the vein lumen. Do not use the vein pick for puncturing the vein, dissecting tissue during cutdown, or 9 manipulating the lead. Extra stylets are packaged with each lead. To avoid damage to the lead or to body tissue, do not use excessive force or surgical instruments to insert a stylet into a lead. Attempt to keep the lead straight when inserting a stylet; do not insert the stylet into a severely bent lead. Hold the lead at the connector end with the lead straight while removing the stylet to avoid stress on the lead body. Keep the stylet clean and free of blood and tissue contact. Accumulated blood and/or tissue on the stylet may hinder its passage into or removal from the lead and make future insertion of stylets impossible. Positioning the Active Fixation Lead Confirm that the helix is completely retracted before implantation. When the helix is completely retracted, the helix tip might extend slightly beyond the lead tip. Note If blood clogs the helix, repositioning may require a greater number of pin rotations to extend the helix. Repeated repositioning attempts may impair the helix extension mechanism. 1. 2. 3. 4. 5. 6. 7. Under fluoroscopic guidance and with the helix retracted, advance the lead into the right atrium. To aid in passing the lead through the tricuspid valve and into the right ventricle: remove the stylet from the lead - shape the distal end of the stylet into a gentle curve - carefully reinsert the stylet into the lead - To avoid damage to the stylet and lead, do not attempt to curve the stylet while it is inserted in the lead. Do not use a sharp object to curve the distal end of the stylet. Under close fluoroscopic monitoring, advance the curved lead/stylet through the tricuspid valve. Pull the stylet back a few centimeters to reduce the risk of the lead damaging the valves or penetrating the heart muscle when it continues down into the ventricle. Continue to advance the lead. When the tip reaches position in the right ventricle, retract the stylet an additional ten centimeters or more. Accurate electrode positioning is vital for stable sensing and pacing. Verify that the lead tip is not placed in the coronary sinus or in a retrograde position, and that the entire distal defibrillation coil is below the tricuspid valve. If desired, evaluate one or more potential fixation sites using the helix tip prior to extending the helix. Refer to the appropriate pulse generator manual for the recommended procedures and values for measuring the sensed R-wave amplitude. CAUTION Do not place the lead near another implanted lead. Such close proximity could result in the electrodes making contact with each other and cause electrical interference. Once the desired fixation site has been located, hold the lead body stationary in one hand and attach the clip-on tool to the connector pin. For instructions on using the clip-on tool, see Preparing the Active Fixation Lead (page 9). 10 8. While keeping the lead as straight as possible, grasp the connector boot with one hand and with the other hand, rotate the clip-on tool clockwise to extend the helix. (Refer to the Technical Specifications sheet for the number of rotations required to extend the helix.) When viewed under fluoroscopy, the helix is fully extended when at least 2 turns are visible beyond the lead tip (Figure 2). Figure 2. Extension and retraction of the helix 1. 2. 3. 4. 9. 10. 11. Helix fully extended Helix fully retracted Marker ring Electrically active helix CAUTION Do not rotate the connector pin after the helix is fully extended or retracted. Doing so may damage the helix mechanism. Under fluoroscopy, verify that the helix is extended, then carefully withdraw the stylet while observing the lead's position. CAUTION The stylet must be withdrawn before defibrillation testing to prevent potential malfunction of the lead. However, the sensing and pacing functions of the lead can be evaluated with the stylet still in place. Verify that the helix is fixed by pulling gently on the lead and checking for resistance. If the lead is properly fixed, resistance will be felt and the lead will remain in place. A poorly affixed lead will come loose easily and must then be repositioned. Allow enough slack in the lead so that it is not under tension as the heart contracts, or the patient breathes deeply or stretches. At the same time for dual-coil leads, ensure that there is not an excess of slack which may allow the proximal electrode to contact the tricuspid valve. Verify proper lead placement by measuring the sensed R-wave amplitude and determining the pacing threshold. Refer to the appropriate pulse generator manual for recommended procedures and acceptable values. Note For DF4 leads, use a sterile patient cable with a plunger clip (such as Models 4160 or 4161) or the IS4/DF4 Connector Sleeve (Model EX3151). The use of alligator clips directly on the lead is not recommended because they may damage the lead. Positioning the Passive Fixation Lead 1. Under fluoroscopic guidance, advance the lead into the right atrium. 2. To aid in passing the lead through the tricuspid valve and into the right ventricle: 11 3. 4. 5. 6. 7. 8. - remove the stylet from the lead - shape the distal end of the stylet into a gentle curve - carefully reinsert the stylet into the lead The flexibility of the lead's distal defibrillation coil allows the distal end of the lead to conform to the shape of the stylet. CAUTION To avoid damage to the stylet and lead, do not attempt to curve the stylet while it is inserted in the lead. Do not use a sharp object to curve the distal end of the stylet. Under close fluoroscopic monitoring, advance the curved lead/stylet through the tricuspid valve and into the ventricular chamber. Pull the stylet back a few centimeters to reduce the risk of the lead damaging the valves or penetrating the heart muscle when it continues down into the ventricle. Continue to advance the lead. When the tip reaches position in the right ventricle, retract the stylet an additional ten centimeters or more. Accurate electrode positioning is vital for stable sensing and pacing. Verify that the lead tip is not placed in the coronary sinus or in a retrograde position, and that the entire distal defibrillation coil is below the tricuspid valve. CAUTION Do not place the lead near another implanted lead. Such close proximity could result in the electrodes making contact with each other and cause electrical interference. Under fluoroscopic guidance, carefully withdraw the stylet while observing the lead's position. CAUTION The stylet must be withdrawn before defibrillation testing to prevent potential malfunction of the lead. However, the sensing and pacing functions of the lead can be evaluated with the stylet still in place. Verify that the tined tip is well fixed in a stable position in the trabeculae of the ventricle by pulling back gently on the lead while observing its position under fluoroscopy. If the lead is properly fixed, resistance will be felt and the lead will remain in place. A poorly affixed lead will come loose easily and must then be repositioned. Allow enough slack in the lead so that it is not under tension as the heart contracts, or the patient breathes deeply or stretches. At the same time, ensure that there is not an excess of slack which may allow the proximal electrode to contact the tricuspid valve. Verify proper lead placement by measuring the sensed R-wave amplitude and determining the pacing threshold. Refer to the appropriate pulse generator manual for recommended procedures and acceptable values. Note For DF4 leads, use a sterile patient cable with a plunger clip (such as Models 4160 or 4161) or the IS4/DF4 Connector Sleeve (Model EX3151). The use of alligator clips directly on the lead is not recommended because they may damage the lead. IS4/DF4 Connector Sleeve The IS4/DF4 connector sleeve is designed for use with an IS4 or a DF4 lead. It provides a safe and secure connection and disconnection to the lead connector. 1. Insert the IS4 or the DF4 lead into the IS4/DF4 connector sleeve until the lead cannot be 12 inserted any further. Figure 3. Inserting the lead into the connector sleeve 1. Contact clips 2. Lead connector pin 3. Connector ring electrodes 2. Verify the connector ring electrodes are visible in each of the contact clip windows. Figure 4. Connector ring electrodes displayed in the contact clip windows 3. Attach all alligator clips to the appropriate connector ring electrodes. Figure 5. Attaching the alligator clips Note Remove alligator clips prior to removing the connector sleeve from the lead. Testing Defibrillation Efficacy Once acceptable sensing and pacing performance have been verified, defibrillation lead testing may be performed to determine the voltage/energy requirements for reliable defibrillation, and to ensure that those requirements are well within the output capabilities of the pulse generator. 13 If defibrillation is performed, ensure that the stylet has been withdrawn from the implanted lead. If the tested configuration does not provide effective defibrillation, the lead may be repositioned or another lead configuration may be chosen and repeat testing may be performed. In some patients, however, no lead configuration may provide reliable defibrillation, and the use of an alternative lead system should be considered. Note If a thoracotomy is required, it should be done during a separate procedure. Suturing the Lead After acceptable lead performance is verified by testing, the position of the lead should be secured using the suture sleeve to prevent dislodgement or migration. The suture sleeve will protect the lead insulation and conductor coil against damage from ligatures: 1. Position the suture sleeve to place it near, against, or just inside the vein. 2. Ensure that excess slack in the lead body is removed before suturing by viewing the position of the lead under fluoroscopy. Allow enough slack in the lead so that it is not under tension as the heart contracts, or when the patient breathes deeply or stretches. 3. Using heavy, nonabsorbable suture on the distal groove, secure the suture sleeve to the vein. Tie the suture firmly but gently to avoid damaging the lead as shown in the figure below. 4. Use the proximal groove to secure the suture sleeve to the fascia and to the lead by first creating a base by looping heavy, nonabsorbable suture through the fascia underneath the groove and tying a knot. Tie sutures firmly around each available groove on the suture sleeve. The most distal groove may be used to tie off the vein over the suture sleeve. Figure 6. Suture the lead 1. Vein 2. Fascia 3. Lead body CAUTION Damage to the lead insulation, damage to the coil, and impairment of lead function may result from failure to use suture sleeves, tying the ligatures too tightly, or otherwise creating excessive strain at the insertion site. Never tie a ligature directly to the lead body. Be careful not to dislodge the lead tip during suturing. Always use heavy, nonabsorbable suture. If desired, a second suture sleeve may be utilized for additional security: 14 1. 2. Carefully open the slit in the sleeve and position the sleeve on the lead body. Follow the procedure (above) to suture and secure the sleeve. Connecting the Lead to the Pulse Generator To prevent damage to the lead, avoid the use of excessive force on the lead body or connector. To avoid dislodgement or potential fracture, do not put the lead under extreme tension or flexion. Do not apply pressure to the lead with a surgical instrument. 1. CAUTION Orient the excess lead length and the pulse generator to minimize the potential for insulation damage resulting from lead-to-lead or pulse generator-to-lead interaction. For example, minimize the potential for leads lying on top of each other under the pulse generator and ensure that there are no sharp bends in the lead. Lead insulation damage can result in electrical current arcing to the pulse generator, thereby damaging the highvoltage circuitry, or creating an alternate electrical current path which may result in compromised therapy delivery. Current practice indicates that a subcutaneous pocket is preferred over a subpectoral pocket. 5 6 Before the lead is connected to the pulse generator, the position of the lead should be reviewed under fluoroscopy, and the R-wave amplitude and pacing threshold measurements should be repeated to verify that the lead has not become dislodged or damaged. Refer to the pulse generator manual for the configuration of the ports on each model. CAUTION Grasp the lead as close as possible to the connector while inserting the lead connector straight into the pulse generator port. If necessary, regrip the lead and continue to insert the lead connector until it is fully seated in the pulse generator port. 2. Connect the lead, carefully pushing the lead connector all the way into the pulse generator ports. Verify visually through the clear top of the pulse generator that the lead connector has been pushed in completely and can be seen protruding behind the port connector. Be sure that the setscrew is tightened before implanting the device. 3. To avoid twisting the lead body, loosely roll excess lead length under the pulse generator before placing the excess lead and the generator in the subcutaneous pocket. In order to avoid stressing the lead conductors and insulation, the pulse generator should not be implanted in the subcutaneous pocket with the lead attached to the ports at a sharp angle. When placing the pulse generator and the lead into the subcutaneous pocket, do not grip the lead or the pulse generator with surgical instruments. Use of excessive force or improper instruments on the lead body or connector during pulse generator placement can cause damage affecting the long-term reliability of the connector and impairment of its function. After connection of the lead to the pulse generator, test the function of the lead with the pulse generator to ensure sensing, pacing, and cardioversion/defibrillation efficacy. 5 Furman S, Hayes DL, Holmes DR. A Practice of Cardiac Pacing. 3rd ed. New York: Futura Publishing, Inc.; 1993:286-289. Belott, PH, Reynolds, DW. Permanent Pacemaker and Implantable Cardioverter-Defibrillator Implantation. In: Ellenbogen KA, Kay GN, Wilkoff BL, eds. Clinical Cardiac Pacing and Defibrillation. 2nd ed. Philadelphia, Pa: WB Saunders; 1995:613615. 6 15 Post-Implantation Follow-Up St. Jude Medical strongly recommends pre-discharge and chronic follow-up electrophysiology studies, including induction of ventricular fibrillation, in order to verify the long-term performance of the lead system. Follow-up chest x-rays to verify the position of the lead are also recommended. It is also recommended that repeat testing be performed if the patient’s clinical status or antiarrhythmic drug therapy has changed. Removing Chronically Implanted Leads Cap any abandoned lead and secure the lead cap with sutures to prevent unwanted transmission of electrical signals from the electrode to the heart. Seal the remaining open end of any severed lead with medical adhesive and a lead cap. Suture the remnant to adjacent tissue using heavy, nonabsorbable suture to prevent migration of the lead fragment into the heart. If the lead or any portion of it is extracted, handle it according to local regulations. Clean the extracted lead with disinfectant and return it to St. Jude Medical for investigation and safe disposal. For safety reasons, it is recommended that all used leads be enclosed in a protective cover. Please complete an Out of Service/Explant/Patient Death form and return it to St. Jude Medical with the extracted lead. Whenever possible, send along a printout of the programmed settings of the pulse generator. Accessories Table 6. Accessories available for use with the products described in this manual Clip-on tool (active fixation models only) DF-1 plug (single coil model only) Lead cap Stylets Stylet guide (funnel, IS-1 models only) Suture sleeve Vein pick IS4/DF4 connector sleeve Stylet Color Codes Table 7. Stylet color codes Knob Color Light green Green Yellow Description Extra-soft straight (40 mm taper) Soft straight (20 mm taper) Firm straight 16 Diameter 0.014 in/0.36 mm 0.014 in/0.36 mm 0.015 in/0.38 mm Technical Support St. Jude Medical maintains 24-hour phone lines for technical questions and support: 1 818 362 6822 1 800 722 3774 (toll-free within North America) + 46 8 474 4147 (Sweden) For additional assistance, call your local St. Jude Medical representative. Symbols The following symbols may be found on the product or product label: Symbol Description DF4-LLHH Quadrapolar connector (low voltage, low voltage, high voltage, high voltage) DF4-LLHO Quadpole connector (low voltage, low voltage, high voltage, open) Active fixation, Extendable/Retractable Steroid-eluting Not to be used when a single dose of 1.0 mg dexamethasone sodium phosphate is contraindicated Contains less than 1.0 mg dexamethasone sodium phosphate Minimum introducer size Optim lead insulation overlay with Fast-Pass coating Endocardial Defibrillation lead One lead Authorized EC Representative in the European Community Sterilized using ethylene oxide Accessories Product literature Contents Caution, Consult Accompanying Documents 17 Symbol Description Consult instructions for use Follow instructions for use on this website Date of Manufacture Reorder number Country of manufacture; BE- Belgium, MY- Malaysia, US- United States Do not use if package is damaged Do not reuse Manufacturer Serial number Temperature limitations Prescription only Use by Device has been demonstrated to pose no known hazards in a specified MRI environment with specified conditions of use. Affixed in accordance with European Council Directive 90/385/EEC. Hereby, St. Jude Medical declares that this device is in compliance with the essential requirements and other relevant provisions of these Directives. Made in USA 18 Cardiac Rhythm Management Division Manufacturer: St. Jude Medical Cardiac Rhythm Management Division 15900 Valley View Court Sylmar, CA 91342 USA +1 818 362 6822 European Authorized Representative: St. Jude Medical Coordination Center BVBA The Corporate Village Da Vincilaan 11 Box F1 1935 Zaventem Belgium +32 2 774 68 11 Manufacturing Site: St. Jude Medical Puerto Rico LLC Lot A Interior - #2 Rd Km. 67.5 Santana Industrial Park Arecibo, PR 00612 USA Manufacturing Site: St. Jude Medical Operations (M) Sdn. Bhd. Plot 102, Lebuhraya Kampung Jawa, Bayan Lepas Industrial Zone 11900 Penang Malaysia sjm.com August 2015 Art 60066360/B Australian Sponsor: St. Jude Medical Australia Pty. Limited 17 Orion Road Lane Cove NSW 2066 Australia