Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
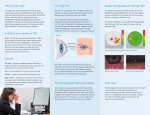
MOORFIELDS PHARMACEUTICALS: EMUSTIL ADVERTORIAL Evaporative Dry Eye Disease Reports from researchers in the field of dry eye disease, suggest that evaporative dry eye may be being under-reported and underdiagnosed.1 The authors indicate that incorrect treatment can result in an exacerbation of the pain, inflammation and visual disturbance associated with dry eye and consequently that correct diagnosis is critical to receiving the correct treatment.1 “The reports expose a greater need to re-evaluate the way that evaporative dry eye disease is currently diagnosed and treated”, says Dan Alalouff, Medical Information Executive at Moorfields Pharmaceuticals. Dry eye, a general term, which collectively describes aqueous deficient and evaporative dry eye, is estimated to affect as many as 17% of women and 11.1% of men 2,3,5 . As a multi-faceted disease of the lacrimal functional unit, the two types of dry eye are characterized by a range of, often overlapping, signs and symptoms including; incorrect tear composition, discomfort, visual disturbance, tear film instability and potential damage to the ocular surface resulting in decreased tear production, increased tear evaporation and inadequate lubrication of the eyes 1-5. Chronic dry eye is particularly prevalent among women, ranging from 5.7% to 9.8%, and this prevalence is thought to increase with age 2,3. Few epidemiological studies to gauge the specific incidence of evaporative dry eye have been conducted, however one study of 224 patients diagnosed with dry eye disease determined that 86% of these exhibited signs of meibomian gland dysfunction4. Different causes of evaporative and aqueous deficient dry eye Both aqueous deficient and evaporative dry eye subtypes present with very similar symptoms and in the case of moderate to severe dry eye, aqueous deficient dry eye may take on the features of evaporative dry eye 2,3. However, the causes of these two types of dry eye are distinct and relate to dysfunction of different components of the lacrimal system. Whilst, aqueous dry eye arises from chronic tear deficiency and dysfunction of the lacrimal glands, evaporative dry eye is primarily caused by dysfunction of the meibomian glands, embedded in the eyelids or extrinsic factors such as contact lense use, vitamin A deficiency and the effects of chronically applied topical anaesthetics and preservatives1-3. Meibomian gland dysfunction (MGD) produces abnormalities in the secreted lipids resulting in impaired tear film lipid layer (TFLL) integrity and the increased evaporation of tears1-3. Further details and diagrams of the major etiological causes of dry eye can be found on our educational website - www.dryeyesmedical.com The tear film layer is composed of three layers; an inner mucin layer, a central aqueous layer and an outer lipid layer. The superficial lipid layer of the tear film is derived from the meibomian glands, which serve to regulate the lipid content and quality of the layer. An intact functional lipid layer allows smooth movement of the eyelid over the eye, reducing the surface tension thus promoting the integrity of the aqueous portion and acting to reduce evaporation of underlying aqueous fluid in the open eye. Tear film instability is one of the primary reasons in developing dry eye and may be the initiating event in the onset of dry eye syndrome. The aqueous layer of the tear film is produced by the lacrimal gland, beneath the upper eyelid. This layer provides moisture, oxygen and electrolytes to the cornea. In aqueous deficient dry eye, where tear production is impaired, the aqueous layer can become more concentrated (hypertonic) and can lead to increased tear osmolarity. In severe dry eyes the tear hypertonicity may result in the development of ocular surface disease. Diagnosis of evaporative dry eye Schirmer’s testing may be used as a first step in identifying dry eye syndrome, as represented on blotting paper by a reduced level of tear secretion 1,3, . However, if tear secretion levels are normal, but the patient still shows signs and symptoms of dry eye, then assessment of Tear Break Up Time (TBUT) using fluorescein strips can be used to distinguish evaporative from aqueous deficient dry eye. A low TBUT suggests the lipid layer has been compromised, and therefore indicates meibomian gland dysfunction and the presence of evaporative dry eye3. Ingredients Soybean Oil 7% + Natural Phospholipids 3% Pack 20 x 0.3 ml Preservative-freeYes Use with contact lenses Yes Treatment of evaporative dry eye Mild to moderate cases of dry eye syndrome are often treated using lubricant eye treatments based on hydroxypropylmethylcellulose (HPMC) or sodium hyaluronate that serve to maintain the aqueous tear film layer but do not treat the underlying reduced tear film integrity associated with evaporative dry eye3. However, Emustil, a preservative free, natural eye drop emulsion which has been specifically formulated for treating evaporative dry eye, has been shown to significantly reduce the frequency and severity of symptoms in moderate to severe evaporative dry eye compared to other lubricant based treatments for dry eye5. Emustil is based on soy bean extracts and the same phospholipids that occur in natural tears, allowing the drops to integrate with and restore the tear lipid layer to reduce evaporation and osmolarity. Research from the Caledonian University has demonstrated Emustil to be as effective as meibomian lipids in reducing tear film evaporation5. References 1) The International Workshop on Meibomian Gland Dysfunction: Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction Geerling G, Tauber T, Baudouin C, Goto E, Matsumoto Y, O’Brien T, Rolando M, Tsubota K, and Nichols K Investigative Ophthalmology & Visual Science, Special Issue 2011, Vol. 52, No. 4 2)The International Workshop on Meibomian Gland Dysfunction: Report of the Diagnosis Subcommittee Alan Tomlinson, Anthony J. Bron, Donald R. Korb, Shiro Amano, Jerry R. Paugh, E. Ian Pearce, Richard Yee, Norihiko Yokoi, Reiko Arita, and Murat Dogru Investigative Ophthalmology & Visual Science, Special Issue 2011, Vol. 52, No. 4 3)2007 Report of the International Dry Eye WorkShop (DEWS) The Ocular Surface, 2007, Vol 5, No. 2 . Available from www.tearfilm.org/dewsreport 4)Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Cornea. 2012 May;31(5):472-8. 5)Effectiveness of Artificial Tears in the Management of Evaporative Dry Eye McCann L.C, Tomlinson A, Pearce E.I., and Papa, V. Cornea, 2012, Volume 31, No.1 6) State of the art management of chronic dry eye Proceedings from a scientific roundtable, 2006 A division of