Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
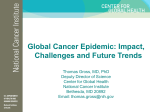
Technical Working Group Meeting on Regional Action Plan and Targets for Prevention and Control of Noncommunicable Diseases Bangkok, Thailand, 11-13 June 2013 NCDs AND ORAL CANCER RATIONALE FOR INCLUSION IN SEAR NCD ACTION PLAN AND VOLUNTARY TARGETS Document prepared for WHO SEARO by: Dr. Habib Benzian The Health Bureau Ltd Consultants for Global Health The Little Barn, Haversham Manor Haversham, MK19 7DZ United Kingdom Mobile: +49 179 7825 420 [email protected] Updated version 31.5.2013 Disclaimer The Health Bureau Ltd (HBL) has no liability for accuracy or inaccuracy of facts reported and used as basis for the outlined conclusions. This document has been prepared for WHO SEARO for a specific context and should not be relied on or used for any other context without an independent check being carried out as to its suitability and prior written authority of The Health Bureau Ltd (HBL) being obtained. HBL accepts no responsibility or liability for the consequences of this document being used for a purpose other than for which it was commissioned. Any person using or relying on the document for such other purposes agrees, and will by such use and reliance be taken to confirm his agreement to indemnify HBL for all loss and damage resulting there from. HBL accepts no responsibility or liability for this document to any party other than WHO SEARO by whom it was commissioned. To the extent that this report is based on information supplied by other parties, HBL accepts no liability for accuracy; however, appropriate measures to ensure correctness were taken. The Health Bureau Ltd 2013 2 1. BACKGROUND & CONTEXT The WHO Regional Office for South-East Asia (SEARO) convened a Regional Consultation to Develop a Regional Strategic Action Plan with Indicators and Targets for Prevention and Control of NCDs in SEA Region during 25–27 February 2013 in New Delhi, India. The participants provided inputs for the draft Regional Action Plan (2013–2020) and discussed the regional indicators and voluntary targets for prevention and control of noncommunicable diseases (NCDs). The proposed nine global targets were confirmed for the region; in addition participants highlighted the need for addressing common cancers such as cervical cancer and oral cancers, as well as indoor air pollution. A small technical working group was tasked to revise the draft Regional Strategic Action Plan, the indicators and targets for consideration of the Regional Committee in September 2013. This document provides the rationale for inclusion of oral cancer in the Regional Strategic NCD Action Plan as requested during the Regional Consultation. The document will be discussed in a meeting of the technical working group in Bangkok in June 2013. 2. WHY SHOULD ORAL CANCER BE INCLUDED IN THE VOLUNTARY TARGETS FOR SEA REGION? There are clearly defined arguments to support the inclusion of oral cancer in the voluntary targets of the Regional Strategic Action Plan for the Prevention and Control of NCDs. 1. The SEA Region is facing a very specific oral cancer burden that differs from other world regions, mainly due to culturally determined practices of tobacco use and habitual chewing of carcinogenic substances. Oral cancer is a significant public health problem for a number of countries in the SEA Region, ranking 2nd for men, 6th for women among all cancers. Oral cancer is the most prevalent cancer for men in India. 2. Oral cancer shares risk factors and determinants that are common to other NCDs, such as tobacco use, high alcohol consumption, nutritional deficits, viral infections, poor (oral) hygiene and genetic dispositions (among other factors). The policy basis for including oral cancer in the NCD context is solid with a number of WHO resolutions supporting a focus on oral cancer among other oral diseases. Therefore, the inclusion of oral cancer is in coherence with major NCD strategies. 3. There is ample scientific evidence related to different aspects of oral cancer, indicating good to medium effectiveness and feasibility of prevention and screening, early detection and referral, as well as guidelines for clinical care and rehabilitation. 4. Examples of successful public health strategies, both in high-, middle- and low-income countries indicate feasibility of integrating oral cancer prevention and care into a primary health care context. 5. Data on oral cancer is available through national, regional and global epidemiological surveillance mechanisms, though oftentimes with limitations due to general weakness of national disease surveillance and/or cancer registration systems in particular. 2.1. PUBLIC HEALTH SIGNIFICANCE IN THE SEA REGION Oral cancers, which are predominantly squamous cell carcinomas (>90%), are a significant public health problem worldwide. Analysing the problem through a variety of indicators and statistical methods reveals that the SEA Region carries the biggest burden of all world regions and comprises some of the countries with highest rates for incidence, mortality and crude risk as well as absolute case numbers globally, both for men and women. Similarly, the key risk factors for oral cancer are of particular relevance in the region. 3 EPIDEMIOLOGY Some summary statistics (for full details see section 6. Tables and Figures): Table 1: Summary statistical characteristics of oral cancer in the SEA Region (GLOBOCAN2008) Indicator (per year) all SEAR countries Men Women Both 8.4 5.0 6.7 59,001 35,399 95,400 Incidence, percent of all cancers 7.9 4.0 5.8 Mortality, age-standardised (W) per 100.000 population 5.7 3.3 4.5 39,345 23,608 62,953 Mortality, percent of all cancers 6.9 4.2 5.6 Ranking (by case numbers) nd th 5th Incidence, age-standardised (W) per 100.000 population Incidence, cases numbers Mortality, case numbers 2 6 Other key epidemiological facts for oral cancer: Worldwide 6th most common cancer, estimations of 400,000-700,000 new cases per year. India: Oral cancer ranks 2nd for men, 4th for women and 3rd for both; over 100,000 new cases every year; highest incidence (40-50/100,0000) in men (60+ age group); most prevalent cancer for men; doubling incidence rate between 1985 and 2006. Sri Lanka: highest overall incidence for males in the region (16.5); as high as 100/100,000 for age group 60+. 5-yr survival rates are generally low (around 40% in India, generally below 50% compared to 50-70% in high-income countries) and have remained largely unchanged over the last decade. Low early detection rates, late presentation of cases and delayed referral rates contribute to low survival rates, together with inadequate oncology care. Clear gradients for all indicators along socio-economic status with higher rates, later diagnosis in more advanced tumour stages and lower survival rates among poor and disadvantaged population groups. Significant inequalities between men and women in terms of disease burden (due to differential exposure to key risk factors), though indicators among women are generally high and increasing; specific inequalities for several ethnic groups and minorities due to cultural practices and risk exposure (i.e. reverse smoking). Predictions for the region: doubling of rates by 2030 based on long latency time after risk exposure, persisting high rates for various risk factors and projected demographic developments. In some statistics oral cancers are grouped together with naso-pharyngeal, other pharyngeal and lip cancer under the term “head and neck cancer” (usually excluding skin cancer). Separation of these statistics would result in even higher oral cancer morbidity and mortality rates. RISK FACTORS Oral cancer shares key risk factors and determinants common to other major NCDs: Tobacco Tobacco use in all forms (including bidis, smokeless tobacco and water pipes) is the single most important risk factor for oral cancer with a clear causal dose-response relationship. There is a belief that tobacco products are beneficial to oral health and several toothpastes and other oral care products are produced on this basis containing tobacco. Other carcinogenic substances (areca nut, betel quid, pan masala, gutka etc) Specific risks arise from the use of other carcinogenic substances: “Betel quid with or without chewing tobacco is common in South Asia. It contains leaves of the Piper betel vine, smeared 4 with lime paste (aqueous calcium hydroxide), chopped nuts of the Areca catechu palm (chrysalidocarpus lutescens) tree, and condiments including astringent catechu bark extract (acacia catechu), cardamom, clove, and sweeteners. In South/Southeast Asia, it is mainly consumed with tobacco; in China and Taiwan, it is mainly chewed by itself, though most users smoke cigarettes. In South Asia, there has been a recent, major increase in pan masala and gutka consumption. These recent, commercialized, dry-packaged versions of betel quid do not include betel leaves. They are mainly produced in India and exported to over 30 countries. Areca nut alone is formally recognized by the IARC as carcinogenic; the dangers are much enhanced if tobacco is included. It is highly addictive. Betel quid is the major risk factor for OPMD and oral cancer in Sri Lanka, a fact of which the population is largely unaware.” (Johnson et al 2011) Alcohol Harmful use of alcohol is a major risk factor for oral cancer, particularly when combined with smoking, which results in a multiplication of risk. A clear dose-response relationship is established. Like for smoking, alcohol use as a risk factor is closely linked to socio-economic deprivation. HPV Infection Emerging evidence suggests that infection with HPV16 and 18 are independent or co-factors for certain oral cancers (oropharynx and posterior tongue), particularly in younger Western populations without other risk factors. HPV-positive oral cancers have been reported at varying rates (20-70%) and no clear conclusions are possible to date with regard to public health consequences for SEAR countries. Studies investigating the impact of HPV vaccinations against cervical cancer are under way. Poor oral hygiene The long-held belief that poor oral hygiene contributes to an increased risk for developing oral cancer has not been confirmed; yet a general neglect of hygiene (including oral) may be symptom of general socio-economic deprivation and related risk factors. Specific issues related to oral health and hygiene (such as sharp edges from a decayed tooth or broken denture) can cause malignancy through chronic mechanical irritation. Nutrition There is clear evidence for a link between under- and malnutrition and cancer, including oral cancer. Food rich in antioxidants from fruit and vegetables, a balanced vitamin intake together with a diet low in animal fat contribute to lower (oral) cancer rates. Nutrition, like other risk factors, is closely linked to socio-economic status and other determinants of health. Industrial and indoor pollution Both industrial and indoor air pollution contribute to head and neck cancer development. For those working or living near certain industries with contact to hydrocarbons and cement and those affected by indoor pollution have higher risks of to be contracted with chronic inflammation of the upper aero-digestive tract and malignancy. However, there also remains an influence of genetic disposition for the development of oral cancer that is difficult to fully quantify across different populations. 2.2. COHERENCE WITH MAJOR STRATEGIES The inclusion of oral cancer in the NCD context builds on a sound global and regional policy basis, which recognizes the specific challenges related to oral cancer prevention and control. In May 2013 the World Health Assembly adopted the Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013-2020, which explicitly addresses oral diseases and oral cancer in particular. The table in Appendix 3/Objective 4/p.50 lists various cancer control policy options for Member States. Among the options listed the document states: “Oral cancer screening in high-risk groups (e.g. tobacco users, betel-nut chewers) linked with timely treatment (FOOTNOTE: Screening is meaningful only if associated with capacity for diagnosis, referral and treatment)” (A66/A/CONF./1.rev1 p.50) 5 Furthermore, the document states that, “increasingly cancers, including some with global impact such as cancer of the cervix, liver, oral cavity and stomach, have been shown to have an infectious aetiology. In developing countries, infections are known to be the cause of about one fifth of cancers […]. Strong population-based services to control infectious diseases through prevention, including immunization (e.g. vaccines against hepatitis B, human papillomavirus, measles, rubella, influenza, pertussis, and poliomyelitis), diagnosis, treatment and control strategies will reduce both the burden and the impact of noncommunicable diseases.” (A66/A/CONF./1.rev1 p.41). Key examples of other WHO resolutions and major international conference consensus documents related to oral cancer are: WHA58.R22 2005 Cancer Prevention and Control …Urges Member States to…give “priority to tumours, such as cervical and oral cancer, that have a high incidence in low-resource settings and are amenable to cost-effective interventions”. …Recommendations for outcome-oriented objectives…“National health authorities may wish to consider the following outcome-oriented objectives for their cancer control programmes, according to type of cancer: “Cancers amenable to early detection and treatment (such as oral, cervical, breast and prostate cancers): to reduce late presentation and ensure appropriate treatment, in order to increase survival, reduce mortality and improve quality of life” WHA60.R17 2007 Oral Health: Action Plan for promotion and integrated disease prevention …Urges Member States to…”take steps to ensure that prevention of oral cancer is an integral part of national cancer-control programmes, and to involve oral health professionals or primary health care personnel with relevant training in oral health in detection, early diagnosis and treatment”. Political Declaration of the UN High-level Summit on Prevention and Control of Non-communicable Diseases 2011 Article 19: ….Member States recognise ...”that renal, oral and eye diseases pose a major health burden for many countries and that these diseases share common risk factors and can benefit from common responses to non-communicable diseases”. Crete Declaration on Oral Cancer Prevention 2005 (co-sponsored by WHO, International Congress on Oral Cancer, Hellenic Cancer Association, Hellenic Association for the Treatment of Maxillofacial Cancer) …The following areas of work should be strengthened: (a) Provision of systematic epidemiological information on prevalences of oral cancer and cancer risks in countries, particularly in the developing world. (b) Promotion of research into understanding biological, behavioural and psychosocial factors in oral cancer, emphasizing the inter-relationship between oral health and general health. (c) Integration of oral cancer information into national health surveillance systems which record chronic diseases and common risk factors. (d) Dissemination of information on oral cancer, prevention and care through every possible means of communication. (e) Active involvement of oral health professionals in oral cancer prevention through control of risk factors such as tobacco, alcohol and diet. (f) Training of primary health workers in screening and provision of first-level care in oral cancer (g) Access to health facilities and provision of systems for early detection and intervention, oral health care and promotion for the improvement of quality of life of people affected by oral cancer. 6 2.3. AVAILABILITY OF EVIDENCE-BASED, EFFECTIVE AND FEASIBLE PUBLIC HEALTH STRATEGIES Major implementation strategies in the NCD context include the reduction of common risk factors, the integration of determinants of health, the focus on prevention as well as addressing NCDs in a primary health care context. The main strategies related to oral cancer are fully aligned with these approaches, though tertiary prevention (clinical care/surgery) requires a rather specific skill-set and appropriate facilities, which on the other hand are not much different to other oncology treatment requirements. PRIMARY PREVENTION Primary prevention remains the key approach to oral cancer control – reducing exposure to risk factors and promoting healthy behaviour are the cornerstones of oral cancer prevention. Focussing on enacting effective tobacco control policies, building capacity among (oral) health professionals for effective behaviour change interventions and promoting healthy lifestyles through an inclusive and appropriate population approach will show positive results across a number of NCDs, including oral cancer. SECONDARY PREVENTION Secondary prevention for oral cancer mainly consists of screening for premalignant lesions and early stages of oral cancer, identifying them correctly, and in providing emergency care (if required) and rapid referral to specialist care if a suspicious condition has been diagnosed. The basic principle is, like with screening for other diseases, that early intervention improves patient outcomes and reduces subsequent treatment cost. Screening can include self-examination, oral visual inspection, adjunctive tests to visual inspection (such as toluidin staining and fluorescence), salivary testing and exfoliative cytology. Evidence suggests that offering visual screening to populations at risk (smokers, users of alcohol or other carcinogenic substances such as areca nut) is an efficient and cost-effective measure that reduces mortality. The costs of screening in a large-scale programme in Trivandrum in India were 0.62US$, while in the US costs were 84US$ per year (both programmes were considered cost-effective in terms of disability-adjusted life years (DALYs) and disease cost averted). There is no justification for adjunctive tests in addition to visual examination since they only increase cost and may not be feasible in a large-scale context as concluded in a recent Cochrane review. The advantage of simple visual examination is that trained non-specialist health personnel can perform it with sufficient reliability in terms of sensitivity and specificity, thus further reducing the costs of screening. The International Agency for Research on Cancer (IARC), a WHO agency based in Lyon (France), has conducted and evaluated screening programmes for oral and cervical cancer and has produced a number of manuals and documentation supporting the training and implementation of visual oral cancer screening. TERTIARY PREVENTION The survival and quality of life after oral cancer diagnosis largely depend on the availability and appropriateness of clinical care and rehabilitation. Despite advances in cancer diagnostics, staging, surgical intervention, multi-disciplinary care as well as chemo- and radiotherapy, survival rates for oral cancer have remained virtually unchanged. “Delay in presentation is attributed to lack of awareness of early symptoms and access to health systems. Professional delay is related to failure of primary care professionals to recognize signs and symptoms indicative of cancer. The main factors associated with late presentation and diagnosis are gender, dental status, alcohol consumption, SES, and tumour location, especially at less visible surfaces of the oral cavity. Treatment of oral cancer should be initiated quickly, but access to centers providing multidisciplinary treatment is limited in developing countries. Facilities for sophisticated reconstruction, advanced radiotherapy, and medical oncology are rare. The high cost of modern cancer care is unaffordable in health systems with low resources, and high demand on facilities leads to delay, contributing to upstaging of disease and decreased survival” (Johnson et al. 2011). Furthermore, in most low- and middle-income countries there are no comprehensive treatment guidelines for oral cancer, a lack of training opportunities for surgeons, specialists and teams. “Treatment will never represent the route to reduced incidence” (Gupta et al. 2013). 7 2.4. EVIDENCE OF ACHIEVABILITY AT THE COUNTRY LEVEL PRIMARY PREVENTION There is good evidence for achievability of policies and legislation related to curbing key NCD risk factors, in particular tobacco use and alcohol regulations. SECONDARY PREVENTION Screening programmes for oral cancer have been successfully implemented in India, Sri Lanka, Bangladesh, Thailand and other low-income countries outside of the region. These programmes showed that screening of high-risk populations is possible, leads to reduced mortality, and results in increased awareness and training in health professionals. The large-scale programme in Trivandrum/Kerala involved more than 200,000 patients observed over a nine-year period and concluded that even under a resource-constrained developing country context visual screening for oral cancer is a cost-effective public health measure if targeted at high-risk populations. Similar findings are reported from the US. However, screening is only useful if appropriate care is available to patients identified with oral cancer or precancerous lesions. TERTIARY PREVENTION The capacity of health systems in the SEA Region with regard to cancer care, and more specifically oral cancer care, varies considerably. Oral cancers are often taken care of by general or plastic surgeons, although the speciality of maxillo-facial surgery is recognized in most countries of the region. The numbers of the oral health professional workforce are generally low, and updated statistics about practicing maxillo-facial specialists for each country are not available. The same applies to other oncology specialists, and to advanced diagnostic capabilities and availability of dedicated treatment centres for tertiary care. While India reports 1500 specialised oncologists, Bhutan reports just two in the country. 2.5. AVAILABILITY OF DATA COLLECTION INSTRUMENTS AND BASELINE Functioning and reliable cancer registration is key to sound epidemiological data on all cancers, including oral cancers. The IARC is promoting the establishment and the strengthening of existing national cancer registration systems and has opened a regional hub in New Delhi last year to coordinate efforts in the SEA Region. While some countries have relatively well functioning cancer registries (India, Sri Lanka, Thailand) others have weak or no systems at all (Bangladesh, East Timor), resulting in poor data on (oral) cancer so that policy decisions must be based on extrapolations. Baseline data is available from IARC GLOBOCAN 2008, however, for some countries of the region the data are based projections (i.e. East Timor). With regard to oral cancer risk factors the situation is much better thanks a number of surveillance instruments related to NCDs and common risk factors. 8 3. POSSIBLE VOLUNTARY TARGET AND INDICATORS VOLUNTARY REGIONAL TARGET 25% REDUCTION OF PREMATURE MORTALITY FROM ORAL CANCER BY 2025 The formulation of this target is in line with the approach and wording chosen in the Global NCD Action Plan and reflects overall changes in mortality, which can result from both, changes in incidence through reduction of risks as well as from improved health system performance. Given the predicted increases of oral cancer cases by 2030 it seems ambitious, but with the relatively high incidence rates and huge population numbers already small improvements may result in significant changes in mortality rates. Furthermore, oral cancer benefits from all approaches to reducing risk factors in the context of the other NCDs so that a considerable spill-over effect from these interventions can be expected. For discussion and decision of the technical expert group a set of indicator options are proposed as follows (modified from Hobdell et al. 2003 – Global Goals for Oral Health by 2020): INDICATOR OPTION 1 35% RELATIVE REDUCTION OF AGE-STANDARDISED OVERALL ORAL CANCER INCIDENCE The formulation of this indicator is in line with the approach and wording chosen in the Global NCD Action Plan. Reduction of incidence can result from decreased exposure to risk factors, either through changes in the environment and protective legislation or through individual behaviour and lifestyle. Age-standardised weighted incidence of oral cancer is routinely collected at regular intervals and collated on the national, regional and global level. A relative reduction of 35% compared to baseline (GLOBOCAN 2008) takes into account that incidence needs to be reduced more in order to achieve a relative mortality reduction of 25%. This is not unrealistic given the multitude of interventions aiming at reducing risk factor exposure, particularly tobacco control. INDICATOR OPTION 2 50% INCREASE OF VISUAL SCREENING FOR INDIVIDUALS AT RISK FOR ORAL CANCER This indicator focuses on the important role of early detection through screening of populations at risk for oral cancer. The challenge is, however, the data collection and documentation, as well as the absence of a reliable baseline. One way could be to establish sentinel sites for long-term evaluation to follow-up on screening interventions. INDICATOR OPTION 3 50% INCREASE OF HEALTH CARE PROVIDERS COMPETENT TO DIAGNOSE ORAL CANCER AND ENSURE RAPID REFERRAL This indicator supports the screening and early detection of oral cancer, as well as the effective referral to appropriate care. Data collection could be done on the basis of attendance figures of continuing professional education courses, or through the selection of sentinel sites for long-term evaluation. Challenges with this indicator are that the competency of providers to screen effectively is no guarantee that they are in fact screening as part of comprehensive screening interventions. Also, screening is only appropriate if adequate care is available. INDICATOR OPTION 4 30% INCREASE OF EARLY DETECTION OF ORAL CANCER This indicator again supports screening and early detection, but the data collection can be done at the facility where the patient presents for first diagnosis. It requires that the cancer registration system is also documenting the staging of the neoplasm. 9 4. GENERAL REMARKS & CONCLUSIONS Existing challenges and current shortcomings in terms of surveillance, prevention and control of (oral) cancer should rather be seen as opportunities to improve and strengthen the respective health system. By developing appropriate and pragmatic solutions aiming at inclusiveness and universal coverage in a primary health care context these challenges can be addressed. This includes the development of a dedicated research agenda to address the gaps in knowledge about oral cancer in the SEA Region. Though oral cancer care requires special training, particularly maxillo-facial surgery, the general challenges related to primary, secondary and tertiary prevention are not very different from other types of cancer. Given the complexity and cost-intensiveness of tertiary prevention a strong focus should be on primary and secondary prevention, including reduction of common risk factors. Similarly to all other cancers, a significant increase in absolute case numbers is to be expected over the next decades due to demographic developments and the long lead-in time of oral cancer.. In conclusion, the analysis of the epidemiological evidence, the available public health approaches, the policy basis, the feasibility of country implementation and continued monitoring through data collection clearly shows that oral cancer is of great and unique relevance for the SEA Region, particularly for India, Bangladesh, Sri Lanka, Nepal and Thailand. Including oral cancer would be completely in line with the policy template of the Global Action Plan on Prevention and Control of Noncommunicable Diseases 2013-2020. The inclusion of oral cancer in the Regional Strategic Action Plan for Prevention and Control of NCDs as an additional voluntary regional target would be a signal to Member States, but also to other countries and world regions, that oral diseases can and must be integrated in the NCD context and that addressing them in this context contributes to reducing the overall NCD burden. 10 5. GLOSSARY OF TERMS Oral Cancer The definition of oral cancer varies, WHO uses the definition proposed by the International Agency for the Research on Cancer (IARC). This classification is the basis for the GLOBOCAN project, which provides contemporary estimates of the incidence of, and mortality, prevalence and disability-adjusted life years (DALYs) from major type of cancers, at national level, for 184 countries of the world. Diagnoses are encoded according to the International Classification of Diseases (ICD10). The latest data available is from GLOBOCAN 2008, released in 2011. Table 2: ICD 10 Cancer localisations ICD 10 Diagnosis Cancer localisation C00 Lip C01-02 Tongue C03-06 Mouth C07-08 Salivary glands C09-14 Pharynx GLOBOCAN defines ICD C00-C08 as oral cancer, while other cancer statistics also include cancer of the pharynx (ICD C09-14) under the term oro-pharyngeal or head-and-neck cancer, thus resulting in different epidemiological figures and difficulties in comparison. Incidence Incidence is the number of new cases arising in a given period in a specified population. This information is collected routinely by cancer registries. It can be expressed as an absolute number of cases per year or as a rate per 100,000 persons per year (see Crude rate and ASR below). The rate provides an approximation of the average risk of developing a cancer. Mortality Mortality is the number of deaths occurring in a given period in a specified population. It can be expressed as an absolute number of deaths per year or as a rate per 100,000 persons per year. Prevalence The prevalence of a particular cancer can be defined as the number of persons in a defined population who have been diagnosed with that type of cancer, and who are still alive at the end of a given year. Complete prevalence represents the number of persons alive at certain point in time who previously had a diagnosis of the disease, regardless of how long ago the diagnosis was, or if the patient is still under treatment or is considered cured. Partial prevalence, which limits the number of patients to those diagnosed during a fixed time in the past, is a particularly useful measure of cancer burden. Prevalence of cancers based on cases diagnosed within one, three and five years are presented as they are likely to be of relevance to the different stages of cancer therapy, namely, initial treatment (one year), clinical follow-up (three years) and cure (five years). Patients who are still alive five years after diagnosis are usually considered cured since the death rates of such patients are similar to those in the general population. There are exceptions, particularly with regard to breast cancer. Prevalence is presented for the adult population only (ages 15 and over), and is available both as numbers and as proportions per 100,000 persons. Disability-adjusted life years (DALYs) In establishing priorities for cancer control, information about both fatal and non-fatal cancer-related outcomes is necessary. Disability-adjusted life years (DALYs) is a key measure for such purposes in that it links the burden of cancer mortality in society with the degree of illness and disability among 11 cancer patients and long-term survivors. DALYs and its two components,- years of life lost (YLLs) and years lived with disability (YLDs)-, are presented within GLOBOCAN 2008 for all ages combined, and are available both as numbers and as standardised rate per 100,000 persons. Crude rate Data on incidence or mortality are often presented as rates. For a specific tumour and population, a crude rate is calculated simply by dividing the number of new cancers or cancer deaths observed during a given time period by the corresponding number of person years in the population at risk. For cancer, the result is usually expressed as an annual rate per 100,000 persons at risk. Age-standardised rate (ASR) An age-standardised rate (ASR) is a summary measure of the rate that a population would have if it had a standard age structure. Standardization is necessary when comparing several populations that differ with respect to age because age has a powerful influence on the risk of cancer. The ASR is a weighted mean of the age-specific rates; the weights are taken from population distribution of the standard population. The most frequently used standard population is the World Standard Population. The calculated incidence or mortality rate is then called age-standardised incidence or mortality rate (world). It is also expressed per 100,000. The world standard population used in GLOBOCAN is as proposed by Segi [1] and modified by Doll et al. [2]. The age-standardised rate is calculated using ten age-groups. The result may be slightly different from that computed using the same data categorised using the traditional five-year age bands. Cumulative risk Cumulative incidence/mortality is the probability or risk of individuals getting/dying from the disease during a specified period. For cancer, it is expressed as the number of new born children (out of 100, or 1,000) who would be expected to develop/die from a particular cancer before the age of 75 if they had the rates of cancer observed in the period in the absence of competing causes. (Source: IARC/GLOBOCAN 2008 http://globocan.iarc.fr) 12 6. TABLES AND FIGURES Table 3: Most common cancers according to world regions Source: Are C, Rajaram S, Are M, Raj H, Anderson BO, Chaluvarya Swamy R, Vijayakumar M, Song T, Pandey M, Edney JA, Cazap EL. A review of global cancer burden: trends, challenges, strategies, and a role for surgeons. J Surg Oncol. 2013;107(2):221-226. Figure 1: Age-standardised (W) incidence of cancers in the SEA Region Incidence/100 000 population –30 –20 –10 0 10 20 30 Lung Breast Cervix uteri Lip/oral cavity Oesophagus Stomach Colorectum Liver Non-Hodgkin lymph Larynx Ovary Bladder FEMALES MALES Brain/Nervous Leukaemia Thyroid Hodgkin’s lymphoma Kidney Prostate Corpus uteri Testis Gallbladder Pancreas Lung and oral cancer in males and breast and cervical cancer in females are most common Source: World Health Organization (WHO), Office for South-East Asia. Noncommunicable Diseases in the SouthEast Asia Region: Situation and Response 2011. New Delhi: WHO/SEARO; 2011 13 Figure 2: Estimated DALYs for oral cancer for different world regions (Source: IARC/GLOBOCAN 2008 http://globocan.iarc.fr) Figure 3: Estimated cumulative mortality (%) for oral cancer (Source: IARC/GLOBOCAN 2008 http://globocan.iarc.fr) 14 7. REFERENCES Amarasinghe HK, Usgodaarachchi U, Kumaraarachchi M, Johnson NW, Warnakulasuriya S. Diet and risk of oral potentially malignant disorders in rural Sri Lanka. J Oral Pathol Med. 2013 American Cancer Society. Cancer Facts & Figures 2011. Available from: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc029771.pdf Are C, Rajaram S, Are M, Raj H, Anderson BO, Chaluvarya Swamy R, Vijayakumar M, Song T, Pandey M, Edney JA, Cazap EL. A review of global cancer burden: trends, challenges, strategies, and a role for surgeons. J Surg Oncol. 2013;107(2):221-226. Ayo-Yusuf OA, Lalloo R, Johnson NW. Trends and ethinc disparities in oral and oro-pharyngeal cancers in South Africa, 1992-2001. SADJ. 2013;68:168-173. Beaglehole R, Benzian H, Crail J, Mackay J. The Oral Health Atlas: mapping a neglected global health issue. Geneva & Brighton: FDI World Dental Education Ltd & Myriad Editions; 2009 Bray F, Ren JS, Masuyer E, Ferlay J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer. 2013;132(5):1133-1145. Brocklehurst P, Kujan O, Glenny AM, Oliver R, Sloan P, Ogden G, Shepherd S. Screening programmes for the early detection and prevention of oral cancer. Cochrane Database Syst Rev. 2010;11:CD004150. Brocklehurst PR, Baker SR, Speight PM. Oral cancer screening: what have we learnt and what is there still to achieve? Future Oncol. 2010;6(2):299-304. Cancela MD, Ramadas K, Fayette JM, Thomas G, Muwonge R, Chapuis F, Thara S, Sankaranarayanan R, Sauvaget C. Alcohol intake and oral cavity cancer risk among men in a prospective study in Kerala, India. Community Dent Oral Epidemiol. 2009 Chaturvedi AK, Engels EA, Pfeiffer RM, Hernandez BY, Xiao W, Kim E, Jiang B, Goodman MT, Sibug-Saber M, Cozen W, Liu L, Lynch CF, Wentzensen N, Jordan RC, Altekruse S, Anderson WF, Rosenberg PS, Gillison ML. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol. 2011;29(32):4294-4301. Chiba I. Prevention of Betel Quid Chewers' Oral Cancer in the Asian-Pacific Area. Asian Pac J Cancer Prev. 2001;2(4):263-269. Dedhia RC, Smith KJ, Johnson JT, Roberts M. The cost-effectiveness of community-based screening for oral cancer in high-risk males in the United States: a Markov decision analysis approach. Laryngoscope. 2011;121(5):952-960. Downer MC, Moles DR, Palmer S, Speight PM. A systematic review of measures of effectiveness in screening for oral cancer and precancer. Oral Oncol. 2006;42(6):551-560. Ferlay J, Shin HR, Bray F, Forman D, Marthers C, Parkin DM. International Agency for Research on Cancer GLOBOCAN 2008: Cancer incidence and mortality worldwide. IARC Cancer base No 10. 2010 Gupta B, Ariyawardana A, Johnson NW. Oral cancer in India continues in epidemic proportions: evidence base and policy initiatives. Int Dent J. 2013;63(1):12-25. Hobdell M, Petersen PE, Clarkson J, Johnson N. Global goals for oral health 2020. Int Dent J. 2003;53(5):285288. Hussain SA. Cancer control in South Asia: Awareness is key to success. South Asian J Cancer. 2013;2(2):55. Iqbal A, Warraich R, Udeabor S, Rana M, Eckardt A, Gellrich NC, Rana M. Role of human papillomavirus infection and other factors in patients with head and neck squamous cell carcinoma. Oral Dis. 2013 Jayaprakash V, Reid M, Hatton E, Merzianu M, Rigual N, Marshall J, Gill S, Frustino J, Wilding G, Loree T, Popat S, Sullivan M. Human papillomavirus types 16 and 18 in epithelial dysplasia of oral cavity and oropharynx: a meta-analysis, 1985-2010. Oral Oncol. 2011;47(11):1048-1054. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225249. Johnson NW, Warnakulasuriya S, Gupta PC, Dimba E, Chindia M, Otoh EC, Sankaranarayanan R, Califano J, Kowalski L. Global oral health inequalities in incidence and outcomes for oral cancer: causes and solutions. Adv Dent Res. 2011;23(2):237-246. Kakde S, Bhopal RS, Jones CM. A systematic review on the social context of smokeless tobacco use in the South Asian population: implications for public health. Public Health. 2012;126(8):635-645. Khawaja MI, Shafiq M, Nusrat R, Khawaja MR. Preventing the oral cavity cancer epidemic. Asian Pac J Cancer Prev. 2005;6(3):420. Kujan O, Glenny AM, Duxbury J, Thakker N, Sloan P. Evaluation of screening strategies for improving oral cancer mortality: a Cochrane systematic review. J Dent Educ. 2005;69(2):255-265. Lee CH, Ko AM, Warnakulasuriya S, Ling TY, Sunarjo Rajapakse PS, Zain RB, Ibrahim SO, Zhang SS, Wu HJ, Liu L, Kuntoro Utomo B, Warusavithana SA, Razak IA, Abdullah N, Shrestha P, Shieh TY, Yen CF, Ko YC. Population burden of betel quid abuse and its relation to oral premalignant disorders in South, Southeast, and East Asia: an Asian Betel-quid Consortium Study. Am J Public Health. 2012;102(3):e17-24. 15 Lee CH, Ko AM, Warnakulasuriya S, Yin BL, Sunarjo Zain RB, Ibrahim SO, Liu ZW, Li WH, Zhang SS, Kuntoro Utomo B, Rajapakse PS, Warusavithana SA, Razak IA, Abdullah N, Shrestha P, Kwan AL, Shieh TY, Chen MK, Ko YC. Intercountry prevalences and practices of betel-quid use in south, southeast and eastern Asia regions and associated oral preneoplastic disorders: an international collaborative study by Asian betelquid consortium of south and east Asia. Int J Cancer. 2011;129(7):1741-1751. Lee CH, Ko AM, Yen CF, Chu KS, Gao YJ, Warnakulasuriya S, Sunarjo Ibrahim SO, Zain RB, Patrick WK, Ko YC. Betel-quid dependence and oral potentially malignant disorders in six Asian countries. Br J Psychiatry. 2012;201(5):383-391. Lee PN. Summary of the epidemiological evidence relating snus to health. Regul Toxicol Pharmacol. 2010 Masthan KMK, Babu NA, Dash KC, Elumalai M. Advanced Diagnostic Aids in Oral Cancer. Asian Pacific Journal of Cancer Prevention. 2012;13(8):3573-3576. Moore CE, Warren R, Maclin SDJ. Head and neck cancer disparity in underserved communities: probable causes and the ethics involved. J Health Care Poor Underserved. 2012;23(4 Suppl):88-103. Mroz EA, Forastiere AA, Rocco JW. Implications of the oropharyngeal cancer epidemic. J Clin Oncol. 2011;29(32):4222-4223. Nair U, Bartsch H, Nair J. Alert for an epidemic of oral cancer due to use of the betel quid substitutes gutkha and pan masala: a review of agents and causative mechanisms. Mutagenesis. 2004;19(4):251-262. Noronha V, Jamshed A, Wattegama S, Piya M, Tsomo U, Hai MA, Baral RP, Prabhash K. A fresh look at oncology facts on south central Asia and SAARC countries. South Asian J Cancer. 2012;1(1):1. Olson CM, Burda BU, Beil T, Whitlock EP. Screening for Oral Cancer: A Targeted Evidence Update for the U.S. Preventive Services Task Force. Evidence Syntheses No. 102. Rockville: Agency for Healthcare Research and Quality (US); 2013 Petersen PE. Strengthening the prevention of oral cancer: the WHO perspective. Community Dent Oral Epidemiol. 2005;33:397-399. Petersen PE. Oral cancer prevention and control - The approach of the World Health Organization. Oral Oncol. 2008 Prabhu SR, Wilson DF. Human papillomavirus and oral disease - emerging evidence: a review. Aust Dent J. 2013;58(1):2-10; quiz 125. Ramadas K, Lucas E, Thomas G, Mathew B, Balan A, Thara S, Sankaranarayanan R. A digital manual for the early diagnosis of oral neoplasia. Lyon: International Agency for Research on Cancer (IARC); 2008 Sankaranarayanan R, Sauvaget C, Ramadas K, Ngoma T, Teguete I, Muwonge R, Naud P, Nessa A, Kuhaprema T, Qiao Y. Clinical trials of cancer screening in the developing world and their impact on cancer healthcare. Ann Oncol. 2011;22 Suppl 7:20-28. Shah SMA, Merchant AT, Luby SP, Chotani RA. Addicted schoolchildren: Prevalence and characteristics of areca nut chewers among primary school children in Karachi, Pakistan. J Paediatr Child Health. 2002;38(5):507510. Sobue T, Inoue M, Tanaka H. Cancer Registry and Epidemiological Study Working Group report. Jpn J Clin Oncol. 2010;40 Suppl 1:i76-81. Subramanian S, Sankaranarayanan R, Bapat B, Somanathan T, Thomas G, Mathew B, Vinoda J, Ramadas K. Cost-effectiveness of oral cancer screening: results from a cluster randomized controlled trial in India. Bull World Health Org. 2009;87(3):200-206. van Monsjou HS, Balm AJ, van den Brekel MM, Wreesmann VB. Oropharyngeal squamous cell carcinoma: a unique disease on the rise? Oral Oncol. 2010;46(11):780-785. Vatanasapt P, Suwanrungruang K, Kamsa-Ard S, Promthet S, Parkin MD. Epidemiology of oral and pharyngeal cancers in Khon Kaen, Thailand: a high incidence in females. Asian Pac J Cancer Prev. 2011;12(10):25052508. Vatanasapt P, Thanaviratananich S, Ratanaanekchai T, Thepsuthammarat K. The burden of head and neck cancers in Thailand. J Med Assoc Thai. 2012;95 Suppl 7:S182-9. Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45(4-5):309-316. Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med. 2007;36(10):575-580. WHO South East Asian Regional Office. Formulatung oral health strategy for South-East Asia. Report of a regional consultation. Chian Mai, Thailand, 28-31 October 2008. SEA-NCD-81. Mumbai: WHO-SEARO World Health Organization (WHO), Office for South-East Asia. Noncommunicable Diseases in the South-East Asia Region: Situation and Response 2011. New Delhi: WHO/SEARO; 2011 16