Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
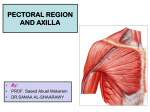
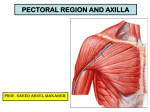
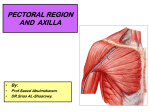
David G. Simpson, Ph.D. PECTORAL REGION, AXILLARY WALLS & VESSELS (Revised 7/08) Text References Moores 3 rd ed. pp 5660, 423429 LEARNING OBJECTIVES: 1. Explain the gross anatomy of the female breast. 2. Understand the lymphatic drainage of the anterior chest wall 2. Discuss the gross anatomy of the pectoral region, naming and describing the major muscles including the innervation, actions, and important attachments. 3. Describe the walls of the axilla. 4. Discuss the contents of the axilla. 5. Draw and label the 3 parts of the axillary artery its branches. Female Breast “The anatomy of the female breast assumes special importance because its distortion provides the clues for diagnosing neoplastic disease.” Breast Cancer Most common cancer for women 188,587 new cases of breast cancer/year or 516/day (men and women) 55,700 in situ (confined) new cases or 152/day 40,954 deaths/year112 per day or 4.6/hour (362 men die/yr) CDC (2004 figures) I. The Anterior Chest is called the Pectoral Region or Breast. The Mammary Gland is a modified sweat gland that develops in the subcutaneous connective tissue layer. Moores 3 rd ed. p5660; Grant's Atlas 12 th ed. 1.3, 1.4. The smooth contours are provided by fat, which makes up the bulk of the breast. The breast is composed of 1520 lobes of glandular tissue. 1. Lactiferous ducts drain the glandular tissue a. One duct per lobe of glandular tissue b. Each duct opens separately on the nipple c. Deep to the areola each duct enlarges to form a lactiferous sinus. Ductograms depicting the structural organization of the ductal system and sinus within a lobe of glandular tissue in the post menopausal (left) and premenopausal breast (right). Contrast media has been injected into the gland. Note the term gland describes a functional unit, not an anatomical unit. The component parts may not necessarily all be located in one small localized domain of the breast. See Grants Atlas 12 th ed 1.5 Connective tissue septa of the breast A. The glandular tissue and more superficial fat in each lobe are separated from adjacent lobes by the retinacula cutis (Grants 12 th ed 1.4). These connective tissue septa extend from the dermis to the fascia that over lies the pectoralis major muscle. The retinacula are more tightly connected to the skin than to the pectoral fascia, this allows the mammary gland to move with the skin over the pectoral muscle. B. The more superior connective tissue septa are called the suspensory ligaments of Cooper (there are other structures called Coopers so the mnemonic here is Coopers Droopers). C. Carcinoma within the lobes may place traction on the suspensory ligaments and produce a characteristic dimpling or retraction of the skin of the breast. Bates, 8th ed. pp. 307309 & 314 Male Breast Principally a landmark However, this region is occasionally subject to neoplastic disease in men. Male Breast Gynecomastia Can be a complication of hormonal or drug therapy, e.g. may be observed in athletes taking steroids, but may be idiopathic. Teenage boys may develop the condition transiently. Lymhatic drainage plays a central role in the spread of breast carcinoma. Moores 3 rd ed. p5660, p59 fig. 1.8. Grant's Atlas 12 th ed. 1.8 A. Axillary lymph nodes receive about 75% of the lymphatic drainage of the breast, they are classified into six groups named by position. B. Parasternal lymph nodes, lie inside the thoracic cavity lie along the internal thoracic artery and receive most of the rest of the deep lymphatic drainage. C. Subcutaneous lymphatic vessels provide only a small part of the drainage, but they cross the midline, and extend up over the clavicle or down onto the abdomen. These vessels also connect with deep lymphatics in the region of the areola. Lymphatic drainage of anterior chest wall. II. Muscles and fascias Clavipectoral fascia attaches to the clavicle above and the fascia of the axilla and lateral thoracic wall (below), surrounding the pectoralis minor. See Moores 3 rd p413 Fig 6.7 Pectoralis Major muscle Moores 3 rd ed. p60. Grant's Atlas 12 th ed. 6.136.18. 1. Innervation, medial & lateral pectoral nerves. 2. Origins (a) medial of clavicle (clavicular head) (b) sternum and upper abdominal region (sternal head) Muscles and Fascias Pectoralis Major •Innervation from Medial and lateral pectoral nerves •Origins from Medial 1/3 of clavicle, Sternum and upper abdominal region •Insertion on crest of greater tubercle of humerus (lateral lip of bicipital groove) 3. Insertion, crest of the greater tubercle of the humerus (lateral lip of the bicipital groove). Pectoralis major muscle Pectoralis Major: Actions (a). Sternal portion is the main adductor of the arm. (b). Cavicular portion flexes arm (c). Medial rotation of the arm. (d). In climbing, this muscle can draw the chest upward and prevents the upward displacement of the humerus and indirectly the scapula in crutch walking. Deltopectoral triangle (groove). Deltopectoral triangle lies between the deltoid and pectoralis major muscles. It contains the cephalic vein. Grant's Atlas 12 th ed. 6.13 & 6.18 Deltopectroal Triangle with Cephalic vein. Pectoralis Minor muscle Pectoralis Minor lies deep to pectoralis major. Grant's Atlas 12 th ed. 6.17, 6.24. 1. Innervation, medial pectoral nerve 2. Origin, from ribs (#3 to #5 usually) 3. Insertion, the coracoid process of scapula Action Acts to depress and downwardly rotate the scapula. ** **Note: cannot demonstrate action or test function of Pectoralis minor in the living independent of Pectoralis major. Pectoralis Minor Muscle (pectoralis major removed) Please Note: Medial Pectoral Nerve Passes through Pectoralis Minor Lateral Pectoral Nerve Passes medial to Pectoralis Minor This naming convention has nothing do with the relative position of the medial and lateral pectoral nerves with respect to the pectoral muscles and has everything to do with the origin of the nerves from the brachial plexus. We will see that in the next few lectures. Subclavius muscle The small Subclavius muscle lies under the medial end of the clavicle, and protects the underlying subclavian artery and vein from the sharp ends of a fractured clavicle. Grant's Atlas 12 th ed. 6.17, 6.24 Innervation is from the subclavius nerve that arises from the brachial plexus. This nerve is really in the neck and we will not see it now. Actions (a). Depresses and rotates clavicle (b). Shunts clavicle anterior during throwing motions Axilla Axilla Significance: A thorough knowledge of the anatomy of this area is required for surgical treatments of breast cancer (i.e., Radical mastectomy, Modified radical mastectomy, Simple mastectomy, Lumpectomy). See clinical insert Moores 3 rd ed. p60. Axilla (I hate this picture but need something to fill this space and can’t find another one) The Axilla is a pyramidal space with and apex above and base below, through which vessels and nerves pass to and from the trunk. Grant's Atlas 12 th ed. 6.20. Moores 3 rd ed p423429 (See p425, Fig 6.11) Boundaries: Anterior: Pectoralis major, forming the anterior axillary fold. Posterior: Subscapularis, teres major, and (forming the posterior axillary fold) the latissimus dorsi. Medial: The chest wall and serratus anterior muscle. Lateral: Intertubercular (bicipital) groove of the humerus. Axilla Axilla Contents HINT: HINT: HINT: Spend time learning this circulatory scheme it will make life easier if you know this before we get into the upper extremity (lots more blood vessels to learn there). LEARN Grants Atlas 12 th ed Table 6.3 and Fig 6.22, 6.7 (carry it around all day if you have too, but learn it). Be able to map out the arterial tree by memory, if you can’t do this you will be in trouble on the tests. 1. Axillary vessels. Grant's Atlas 12 th ed. 6.22, 6.7 & Table 6.3. A. The Axillary Vein is the continuation of the brachial vein at teres major, and in turn continues as the subclavian as it crosses the first rib. We will remove this vessel during the dissection to make a clear field of view for the underlying structures. B. The Axillary Artery "begins" at the first rib as the continuation of the subclavian artery and continues into the upper extremity where it becomes the brachial artery at the lower border of teres major. It is divided by the pectoralis minor muscle into 3 parts: 1. First part or the Proximal 2. Second part or the Deep 3. Third part or the Distal Branches of the Axillary Artery (1) First part: has one branch. Grants Atlas 12 th ed 6.7 (this is a very good image) (I) The supreme thoracic arises from the first part of the axillary artery proximal to pectoralis minor. It passes into the first intercostal space. (2) Second part: has two branches arising deep (behind) to pectoralis minor. (I) Thoracoacromial trunk, has four named branches to the thoracic wall; (A) pectoral, (B) deltoid, (C) clavicular & (D) acromial branches. (II) Lateral Thoracic, which follows the inferior border of pectoralis minor to the thoracic wall. Accompanied by the Long Thoracic nerve, to the serratus anterior muscle. (3) Third part: has three branches arising distal to the pectoralis minor. (I) Anterior humeral circumflex, smaller than the posterior humeral circumflex branch and running anterior to encircle the surgical neck of the humerus. (II) Posterior humeral circumflex may arise from a common trunk with the anterior humeral circumflex. Accompanies the axillary nerve to the posterior surface of the humerus. It is susceptible to injury in a surgical neck fracture. Commonly, there is an anastomosis between the anterior and posterior humeral circumflex arteries. (III) Subscapular, the largest branch of the axillary, gives in turn two terminal branches (Grants 12 th 6.22): (a) Circumflex scapular, passes through the triangular space to ramify in the infraspinatus fossa. (b) Thoracodorsal, continues along the latissimus dorsi muscle in the company of the thoracodorsal nerve (to latissimus dorsi).