Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
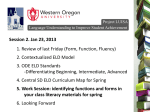
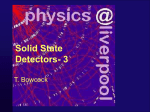
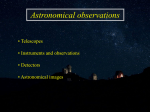
Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 CdTe and CdZnTe detectors in nuclear medicine C. Scheiber* Institut de Physique Biologique Faculte& de Me& decine, 4, rue Kirschleger, 67085 Strasbourg Cedex, France Abstract Nuclear medicine diagnostic applications are growing in search for more disease speci"c or more physiologically relevant imaging. The data are obtained non-invasively from large "eld c cameras or from miniaturised probes. As far as single photon emitters are concerned, often labelled with Tc (140 keV, c), nuclear instrumentation deals with poor counting statistics due to the method of spatial localisation and low contrast to noise due to scatter in the body. Since the 1960s attempts have been made to replace the NaI scintillator by semiconductor detectors with better spectrometric characteristics to improve contrast and quantitative measurements. They allow direct conversion of energy and thus more compact sensors. Room-temperature semiconductor detectors such as cadmium tellure and cadmium zinc tellure have favourable physical characteristics for medical applications which have been investigated in the 1980s. During one decade, they have been used in miniaturised probes such as for inter-operative surgery guidance which is today in a fast growing phase. This material su!ers from charge transport problems which has slowed down imaging applications. Owing to a considerable research work on material, contacts and dedicated electronics small "eld of view compact pixellated c cameras have been prototyped and one already marketed. Although extended clinical evaluation has to be conducted and long-term reliability assesed, the available data already con"rm the expected gain in image contrast. Medical interest for dedicated imaging systems is greater than it was in the 1980s when the "rst mobile c cameras were marketed. The future of CdTe or CdZnTe-based imager for routine use now relies at "rst on industrial costs. 2000 Elsevier Science B.V. All rights reserved. Keywords: Semiconductor detectors; CdTe; CZT; Nuclear camera; Imaging 1. Introduction Nuclear medicine (NM) aims at functional imaging based on radiotracers. Although the 1990s were marked by the rapid development of non-ionising radiation imaging modalities (MRI, US) with high soft tissue contrasts, submillimetric resolution and capable of functional studies as well as morphology, there is still a fast growing demand for more * Tel.: #33-3-88-14-48-56; fax: #33-3-88-37-14-97. E-mail address: [email protected] (C. Scheiber). physiological investigations and/or disease speci"c investigations: the domain of NM expertise. The poor (or even the lack of) anatomical representation in NM studies is not a handicap as multimodal imaging registration and fusion are now clinically available. This is particularly noticeable in neurology, cardiology and oncology, as new highly speci"c tracers have been developed. Today, detection characteristics are still one of the main limiting factors of an even more rapid growth of NM. In general, NM investigations used a stationary device, the c camera, but dedicated devices are actively investigated. This paper will report that 0168-9002/00/$ - see front matter 2000 Elsevier Science B.V. All rights reserved. PII: S 0 1 6 8 - 9 0 0 2 ( 0 0 ) 0 0 2 8 2 - 5 514 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 CdTe and Cd Zn Te (CZT) detectors are good \V V candidates for both approaches. The "eld of CZT NM applications has been regularly reviewed [1}5], we will report only the last technical developments, and, from the NM physician point of view, actual trends in NM, which will naturally, or already have, in#uenced the development of instrumentation. The literature has reported extensively the physical characteristics of these semiconductor detectors working at room temperature and their dedicated electronics which will not be detailed here. 2. Nuclear medicine: general considerations In NM, a c ray emitting radiotracer is injected into the body. Then a device, usually a c camera, is used to image its biodistribution as a function of time or after a chosen delay after injection according to the metabolism of the drug. The basis of NM is that the counting statistics is proportional to the concentration of the radiopharmaceutical. As far as the human body and disease's diagnostic or biological function measurements are concerned, this leads to very di!erent situations regarding the detection problem. At "rst, single photon (SP) studies and positron emission tomography (PET) studies have to be distinguished. PET makes use of coincident detection of 511 keV positron-annihilation c rays. Clinical applications of positron emission tracers are expanding. A!ordable clinical PET cameras have been presented on the market and new c cameras can be equipped with coincidence detection circuitry. The characteristics of PET detector modules have been updated recently [6], CdTe or CZT detectors are currently being tested to "nd out if they can be useful in the detection of 511 keV photons, yet their e$ciency is rather limited owing to the thickness of the current material and photo memory. This modality will not be discussed in detail here. In SP studies the tracer is typically a biologically relevant molecule labelled with Tc (140 keV, c ray). Although labelling molecules with Tc is di$cult, compared to I (360 keV, c and b) for example, it has more favourable dosimetric characteristics (energy, physical half-life: 6 h) and thus much higher activity (up to 1000 MBq) might be injected intravenously while keeping the dose in an acceptable limit (comparable to radiology) regarding the expected bene"ts for the patient. The counterpart is a high attenuation coe$cient in the body (0.12 cm\) and a high Compton fraction which hampers data quanti"cation and lowers the contrast. Spatial localisation of the primary photon's source in SP studies is achieved by the use of a collimator, basically a slab of lead absorber containing long thin, typically parallel, bores. The bore con"nes the detector's "eld of view to a narrow, forward cone at each position of its surface. The contrast of the lesion is a decreasing function of distance both due to geometrical considerations and to other spatial super-impositions of various biological sources that have physiologically, including circulating blood, or pathologically uptake the tracer. Ampli"cation of the contrast is achieved by the use of the computed tomography principle (single photon emission computed tomography or SPECT) but at the cost of an increased acquisition time (typically 15}30 min). The second cause of a low contrast is the presence of a large scatter fraction in the body. Energy resolution is useful in rejecting those scattered photons which seems to originate from the location of their last scatter. In some situations a single probe is su$cient or a miniature device is requested, during surgery for example, but usually an NM imaging system is preferred. In both cases the detection system is designed for the best compromise between the spatial resolution, which is always rather poor (6}8 mm at 10 cm from the detection plane) and the counting statistics which is typically very low compared to other ionisation methods. In addition, the acquisition time is limited. The size of the useful "eld of view is controlled by the need to follow simultaneously several areas of interest in the body or to complete a whole body screening in an acceptable acquisition time (10}15 min). In some favourable situations the acquisition time is controlled by the patient relative immobility and/or the device occupational time but very often by the dynamics of the physiological process of interest (cardiac motion for example, 40 ms sampling). The compromise will be di!erent according to the clinical problem. For example the localisation of a sub-centimetric tumour deep in the body during C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 surgery requires a high sensitivity nuclear probe, heart perfusion imaging a tomographic system which can get close to the chest, while cardiac ventriculography pass study "rst requires high sensitivity. Imaging a small super"cial organ like the thyroid gland requires a system with a small "eld of view system whereas it is mandatory to use a large "eld double head for whole body scanning seeking bone metastasis. The NM physician is looking for the best spatial resolution and energy resolution (5}7 keV at 140 keV) while keeping the e$ciency (counting statistics) high in the available acquisition time. For practical reasons most of the NM specialists still want to achieve these goals in the NM department with a single device. However, this is not always feasible nor desirable, then dedicated systems are requested. The clinical demand of NM investigations has changed these last 10 years, according to several factors which can be related to the disease (frequency, diagnostic problems, treatment possibilities, etc.), and of the e!ectiveness of NM compared to others competitive medical imaging methods (performances but also costs, availability, etc.). The NM instrumentation has to adapt. 515 Fig. 1. A two-head commercial c camera equipped with large INa scintillator detectors. The detector is cumbersome and required heavy shielding (courtesy of Siemens AG). 3. General purpose imaging system: c the camera The 1999 c camera is a two-head SPECT system (Figs. 1 and 2). Each head (Fig. 3) is equipped with a large "eld NaI scintillator (40;50 cm). A thickness of 8 mm, a compromise between the e$ciency and the intrinsic spatial resolution, is optimised for the 140 keV photons. Each c-ray interacting in the scintillator produces a #ash of light which is viewed by an array of photo-multiplier tubes (PMTs). Digital circuitry and other localisation schemes might be used instead of the original Anger principle (1958) which consists of a network of calibrated resistances to make an estimate of the interaction position of a c ray in the crystal from the relative responses of the various PMTs. The c-camera has an intrinsic resolution of &3 mm full-width at half-maximum (FWHM) and a 6}8 mm FWHM at 10 cm with the so-called highresolution collimator. In the clinical conditions the collimator controls both spatial resolution and Fig. 2. Schematics of an Anger c camera. The photons emitted by the medical target are spatially localised by the parallel collimator (1,4). The scintillation light resulting from the interaction of a c ray in the NaI(Tl) crystal is viewed and localised by a battery of photomultiplier tubes connected through a resistance network. A good energy resolution is required to reject the scattered photons (3). 516 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 Fig. 3. CdTe typical raw spectrum Co (122 keV, 136 keV), although the energy resolution is improved compared to INa(Tl), there is a signi"cant tail due to poor hole collection and trapping. sensitivity. The energy resolution is rather poor (&11% FWHM), thus a signi"cant fraction of scattered photons contributes to decrease the image contrast. The c-camera is designed for bone whole-body scintigraphy (seeking bone metastasis, 40% of the NM studies) and cardiac SPECT perfusion studies (&25%). The equipment is cumbersome, partly due to the shielding of the detectors and the PMTs. Room-temperature semiconductor detectors have several advantages compared to NaI scintillators: a direct conversion of energy with the corresponding better energy resolution and less cumbersome compared to the NaI-PMT assembly, including less shielding. 4. CdTe and CZT as NM detectors Among the range of solid detectors available for c-ray detection, CdTe [7] and/or CZT [8,9] have a privileged position. They have a high absorption coe$cient (Cd: 48, Te: 52) and their wide band gap (E "1.5}1.7 eV) allows stable counting at body temperature, and their energy resolution is better by a factor two as compared to NaI-based systems (Fig. 3). Unfortunately, until recently, these characteristics were obtained for 2 mm thickness, which result in a low e$ciency. Indeed, these materials su!er from carrier recombination and trapping which lead to incomplete charge collection. When used in the pulse counting mode, the resulting spectra exhibit low-energy `tailinga that reduces the photopeak e$ciency. CdTe : Cl, grown by THM, is now much better known and solutions have been found to polarisation problems. HighPressure Bridgman CdTe or CZT have more favourable characteristics: larger volumes are obtained and higher resistivity (at least one order of magnitude, 10 ) cm). On the negative side, poorer hole collection as well low production yields are observed (industrial costs). Further improvements have been obtained through extensive research on intrinsic properties of the material [10,11]. Better hole collection has been achieved by designing detectors and/or electrodes of various geometry [12}14]. Compensation of charge trapping by signal processing is feasible at the cost of an additional electronic circuitry [15]. However, it is not clear that these methods would be applicable to a large multi-element detector-array such as a routine NM clinical imager, as alternative, ohmic-contact detectors operating in the photo-conductive mode are investigated [16]. Much of the published recent research work was done on CZT but it is still necessary to further improve the material quality to exploit it fully [17]. 5. Small-5eld pixellated CdTe or CZT c camera: an obliged step toward the standard c-camera, or an useful clinical tool? Today, to the best of our knowledge, the 0.1}0.2 m active area per detector head for a large-"eld c-camera will be still too expensive for clinical systems. The "rst prototypes are small-"eld c-cameras. Small "eld of view cameras are attractive: they can get closer to the patient, they are more patient friendly and can be mounted on a mobile cart to reach the operation room and/or the intensive care unit for cardiac and/or pulmonary studies. Marketed in the 1980s, mobile, small-"eld Anger c-cameras have received limited enthusiasm from the medical community. This can be explained partly by "nancial aspects, NM logistics and radioactive sources regulations. Nevertheless, in 1999 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 517 Fig. 4. (A) The test object was plunged in a Tc solution and (B) imaged by a commercial HELIX camera (Elscint, Haifa), the 3 mm sector was not resolved. (C) The "rst images obtained with comparable acquisition times by the BIOMEDII module (2.83;2.83 mm CdTe detectors), the contrast is better for the 4 mm. (D) MoireH e!ect is seen on the 3 mm sector. `imaginga patient might require a di!erent approach. An a!ordable high-performance small-"eld dedicated system, could be attractive, for example, for orthopaedics, endocrinology or paediatric services in numerous hospitals which cannot house an NM service. Despite these commercial considerations and industrial issues, which remain to be solved, important and rapid developments are observed in this "eld. Several groups are working in that perspective. The "rst CdTe medical imaging system was presented in 1996 by Eisen et al. [18] who have developed a small-"eld (16;16 cm) camera equipped with 40;32 CdTe : Cl detectors with Pt contacts. Each single detector was attached to a low noise preampli"er and an ampli"er/shaper. The pixel size was 4;4 mm. Images from the heart and the thyroid have been presented. The performances of the NUCAM were comparable to that of Anger camera although with reduced e$ciency [19]. A European Consortium (see dedicated paper this conference) have developed a small-"eld cardiac (BIOMED II project) based on the same approach with a comparable "eld of view (15;15 cm) and an &3 mm pitch. Acquisitions using a 256 pixels module were obtained on test objects [20], they look sharper when compared to that taken from an Helix (formerly Elscint, now General Electric) 518 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 Fig. 5. The Digirad 2020Tc imager (courtesy of Digirad). The small "eld of view 20 cm detector can be placed close to the patient for better geometric conditions. Real clinical interest exists for low cost small-"eld camera: a challenge for CdTe or CZT-based systems. c camera (Fig. 4). Unfortunately, the crystal thickness of 2 mm and tailing result in a lower sensitivity which could hamper cardiac dynamic studies. St GOBAIN industrial Ceramics, US (Division BICRON), CRISMATEC (France) and LETI (CEA, France) are developing an NM device, PEGASE, starting from a CdTe : Cl module (4;4 pixels) with a dedicated ASIC [21] developed in the frame of the INTEGRAL program (CEA, SAGEM, France). The device will be equipped with new CdTe (high-pressure Bridgman) detectors and dedicated electronic signal processing circuitry [15]. In 1997 DIGIRAD Corporation (San Diego, CA, US) has marketed the "rst small "eld of view c camera based on CZT detectors: the 2020tc Imager (Fig. 5). The active area was 216;216 mm made of 64 modules 25;25;5 mm. Each module was composed of a CZT wafer with 8;8 pixels (3;3 mm) and an electronic shaping circuitry. The resolution in energy of these detector equipped with an original electrode (Spectrum Plus2+) was 8% (at 140 keV, but should attain 4%) [22]. Clinical images are available on their web site (www.digirad.com). The system could even perform heart SPECT studies by rotating the patient using a rotating chair with respect to the camera head plane. Another approach consists in assembling several sub-units of monolithic arrays of CdTe or CZT detectors, coupled to MUX circuitry, adapted from infra-red technology [23], through indium bumps. Unlike the Anger camera, the intrinsic spatial resolution of a semiconductor array imager is determined by a well-de"ned element size; lower limits on this size are, generally, established by the readout circuitry and can be signi"cantly (1 mm. The "rst image was presented in 1993 using a 32;32 array of CZT detectors [24]. Another reason to decrease the pixel size is that in multi-elements with pixel dimensions smaller than the detector thickness, the deleterious e!ect of hole trapping can be greatly reduced by taking advantage of the `near "eld e!ecta [25]. The "rst detector array of this kind was a 48;48 MUX coupled to a CZT array [26]. The CZT slab (29;2.9;0.3 mm) was partitioned into 2304 cells (125 lm pitch) by photo-lithography and connected to the MUX for readout. Most of the leader manufactures involved in NM instrumentation have a semiconductor camera project. As an example, the ELGEMS (Haifa, Israel) prototype, presented at the annual meeting of the Society of Nuclear Medicine (June, 1999), is based on IMARAD detectors. IMARAD is a young Israeli company, which markets since 1999, 40;40;4 mm detector modules of CZT indium doped detectors [17] with a 16;16 pixels (2.5 mm pitch) resolution. They claimed a 5% energy resolution (140 keV) and a 70% e$ciency (13% energy window). Images have been made with the same resolution test object than for the BIOMED II module and can be compared (Fig. 6). Clinical data have been obtained as well. The camera is equipped with a modi"ed collimator (6.8 cm FWHM at 10 cm). Siemens Med. Sys. Inc. (Ho!man Estates IL, US), works on an R&D basis with IMARAD, to develop a large "eld c-camera. C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 519 Fig. 6. (A) The same test object as in Fig. 4A and B the thyroid Picker phantom, imaged by the ELGEMS's CZT pixellated small "eld imager prototype compared to the Anger c camera (C and D) showing an improved spatial resolution in these experimental conditions. (Presented at the Annual Meeting of the Society of Nuclear Medicine, Los Angeles, June 1999; courtesy of A. Pansky.) 6. Other approaches to NM stationary devices The spatial resolution/e$ciency compromise is controlled by the collimator and even if it is feasible to improve the intrinsic spatial resolution of the detector it will be necessary to develop another approach to localise the source to take bene"t from it. One approach is illustrated by the ultra-highresolution brain SPECT system from the Division of Nuclear Medicine of the University of Arizona. A camera dedicated to a single organ is more challenging but justi"ed for brain function. In fact, there is a rapid growing demand for brain perfusion studies (psychiatric disease, epileptic foci localisation, etc.) owing to newly-developed blood-#ow (Tc-HMPAO or Tc ECD) or brain-receptors speci"c radio-pharmaceuticals. It has been shown and demonstrated in simulations [27] that a combination of multiple pinhole imaging system and a high-resolution detector can result in substantial improvement in counting e$ciency over conventional systems. The original system was equipped with NaI detectors; a prototype utilising CZT focal-plane arrays is under development [28] (Fig. 7). The system will use 256 modular detectors in a full 3D-SPECT approach. This group has developed an NM speci"c hybrid semiconductor detector array consisting of a 64;64 pixels CZT detector array (1.5 mm thick, 380 lm square pixel electrodes on one side produced by lithography) mated to a multiplexer readout circuit that was custom designed for this NM application [29]. The cost of semiconductor detectors is still the main limitant factor for the achievement of the project. Another completely di!erent approach is the electronically collimated SPECT [30], also known as the Compton camera. Counts in electronic 520 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 Fig. 7. Artist view of the ultra-high-resolution brain imager from the Tucson University (Arizona, US) (courtesy of HB Barber). collimation are acquired in a coincidence counting mode between two positions and energy sensitive detectors from those c rays which scatter from the "rst detector onto the second after depositing a measurable energy in the "rst detector. These informations su$ce to con"ne the c rays origin to a cone in space about the initial interaction position. The uncertainty of location perpendicular to the cone's surface is related to the spatial resolution and energy resolution of the detectors, the "rst system used an array of Ge detectors as a "rst detector and a conventional camera. Recently, feasibility of using CdTe [31] and CZT [32] detectors has been demonstrated. Although the CZT-based detector system e$ciency was a factor of 2.5 lower than the Ge at 140 keV corresponding to a system spatial resolution which is also a factor of two lower, the di!erence will decrease at higher energies. From the physics of Compton scattering it is expected that this Compton camera will work better at higher energies such as 511 keV (positron-annihilation c rays). The department of medical physics and Bioengineering at the UCL (London, UK) has regarded semiconductor detectors to be used in their small prototype for the Compton imaging of annihilation photons produced from positron emitters [33]. Although CdTe has shown a better ratio of geometric e$ciencies compared to Si, the latter was chosen owing to a higher Compton/photoelectric-peak ratio. Some possible clinical implications of the markedly improved sen- sitivity are: shorter imaging times (resulting in faster patient throughput, greater patient comfort, reduced motion blur); reduced patient/worker radiation exposure; and `non-tumour-stunninga diagnostic imaging work-ups for subsequent radiopharmaceutical cancer therapy. Additionally, the proposed system will be completely stationary, more compact than the bulky and heavy rotating cameras in use. Simultaneous measurement of X-ray computed tomography (CT) and SPECT can be used for structural and functional correlation and for improved quantitation of radionuclide uptake as compared to SPECT. This is usually obtained by acquiring transmission imaging using external radioisotope sources. More detailed anatomical information can be obtained by acquiring a real CT image. This can be achieved by coregistration of the two data sets acquired on CT and SPECT systems, respectively, or by the use of hybrid CT}SPECT system, as the new ELGEMS's system which combines on the same gantry an X-ray digital CT system and a dual-head c camera. One would prefer a single detector system such as a pixellated CdZnTe array [34,35] designed to acquire both transmission and emission data simultaneously which is currently evaluated. 7. Miniaturisated probes and imaging systems In at least two circumstances the NM device has to be further miniaturised: ambulatory monitoring of physiological functions and intra-operative guided surgery. Recent clinical validation of the sentinel-node concept has burst these applications. 7.1. Continuous monitoring of physiological functions In several pathological circumstances the symptoms of malfunctioning of a physiological function are transient and di$cult to quantify or even to recognise without multiple measurements. The most well-known parameters are electrocardiogram, blood pressure, and/or blood glucose. NM investigations allow precise measurements of renal and cardiac function even in ambulatory C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 conditions. Some commercial systems have been proposed, but till now, these applications have been restricted to experimental works and clinical research. CdTe detectors have been used for over 15 years for blood #ow measurements, or in the assessment of the renal or cardiac function (for a review see Refs. [1,3]). The latest developments concern several new CdTe-based multi-probe and/or multidetector systems. Continuous monitoring of the cardiac ventricular function has been successful in patients with coronary artery bypass grafting [36] using a single CdTe-detector probe. The same system has been applied to the measurement of the cardiac functional response to exercise in patients with non-obstructive cardiomyopathy [37]. Ambulatory monitoring can be contemplated, using a dedicated system based on a 16-CdTe detector array (10;10;2 mm) [38] with associated portable autonomous electronics and a self-contained data recording device [39]. 7.2. Intra-operative probes Nuclear probes have been used for a long time as an aid to surgeon in the detection of small amounts of (malignant) tissues [40]. Throughout the past 10 years of practice, radioguided surgery (RGS) applications have been extended to other pathologies (for a review see Refs. [41}43]. Three main factors are involved in the interest of using a probe during surgery: the lesion (or all lesions) has not been identi"ed and/or localised with su$cient precision before the surgery by imaging (any modality), the surgeon wants to be sure that all the malignant tissue has been excised and/or, more recently, to guide the surgeon to "nd involved lymph nodes for lymph node dissection. In the 1980s the main application was radioimmuno-guided-surgery (RIGS) [43] which focused on the high speci"city of the tracer to identify a tumour of previously known origin. The patient is injected prior to surgery with a targeting agent, typically a monoclonal antibody labelled with a low-energy c- or b-ray emitter. The ideal targeting agent binds speci"cally to malignant tissue while the unbound fraction is gradually cleared from the bloodstream and from normal tissues. 521 Colorectal cancer used to be the main target, now, RIGS challenges traditional decision making [44,45]. Besides primary tumour and metastasis, the detection of tumour lymph-nodes (I MoAb CC49) [46], prostate cancer (I B72.3) [47] or gastrinomas (I somatostatin) [48] have been made. Lymphoscintigraphy (LS) aims at the mapping of lymphatic routes using Tc- nanocolloids. There was "rst a clinical boom at the end of the 1970s on the grounds of its use in the evaluation of the internal mammary chain in breast cancer patients. Again LS becomes important today in oncology because of the validation of the `sentinel node concepta [49,50]. Here LS is oriented to identify the "rst appearing lymph node to receive drainage from a primary tumour and the visualisation of an a!erent lumphatic vessel from the primary tumour to this node as the two major criteria in identifying the sentinel node. Once identi"ed a surgical biopsy technique can predict whether cancer has spread into the surrounding lymph nodes, this may result in a change in the surgical plan. This staging procedure is now validated for frequent cancer diseases such as melanoma and breast cancer. Imaging with the c camera is performed after intra-dermal injection of the drug at a location depending on anatomical lymphatic routes draining the tumour site. The probe is used prior to surgery to locate the site with the higher count in the lymphatic basin and is marked as the spot where the incision will be made. The device consists of a hand-held probe which is used as a homing device (Fig. 8). The probe must have a high absolute sensitivity, a good side shielding, a high-energy resolution, good spatial localisation (angular sensitivity), ergonomic characteristics and must be adapted to work in the operating room (Fig. 9). The RGS probes have been compared based on basic physical characteristics [51] seven commercially available probes (CdTe, CZT, NaI, CdTe or CsI) showed the same relative performance in a perspex phantom. The CZT and NaI based probes were preferred owing to their higher sensitivity in the 300}400 keV range (I, 360 keV). A more practical approach is to allow comparison of probe performance in terms related to the task of sentinel lymph node localisation in melanoma and 522 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 environment. New probes devoted to laparoscopy or endoscopy are under investigation. LS combined with the gamma probe and/or blue dye for adequate sentinel node biopsy will become an important part of a clinical work in NM and surgical oncology in the next few years [54]. As stated by Ell [55] at the First International Congress on the Sentinel Node in the diagnosis and treatment of cancer (Amsterdam, April 1999): `there appear to be real added value in the application of this methodology in the investigation but also in the management of large numbers of patients with operable cancera. 8. Conclusion Fig. 8. An example of a miniaturised probe used for radioguided surgery. Fig. 9. The RGS system is handled by the surgeon during the surgery in the search for the lymph node(s) draining the primary tumour directly: the sentinel node. breast cancer [52] which used Tc tracer; the best probe tested allows SLN localisation between 20}30 mm closer to the injection site than the poorest performing probe. CdTe and CZT probes currently available are single-detector systems, but miniature multi-detector devices are being tested such as 25-CdTe (2;2 mm) detector imaging device (10;10;13 mm) [53] suitable for surgical The clinical demand of improved systems is growing as NM applications are expanding. Owing to extensive research and industrial work conducted by teams of solid state physicists, engineers and medical physicists CdTe/CZT detectors are now widely accepted and used. There is still some further improvement of the material to be expected which is mandatory in the perspective of commercial products at reasonable costs. CdTe/CZT based surgery probes will have a large impact on patient management in surgical oncology. Although a large "eld c camera is still a dream, mainly due to the cost of the multi-element detector array, small-"eld cameras with improved energy resolution have been developed. First, clinical images are promising. From the NM physician point of view, the future of these systems might depend on both their cost which should clearly be below that of a large"eld system and also on the capability of NM investigations to spread to other environment rather than the NM service where they will have a large clinical use. References [1] C. Scheiber, J. Chambron, Nucl. Instr. and Meth. A 322 (1992) 604. [2] H.B. Barber, J. Electron. Mater. 25 (1996) 1232. [3] C. Scheiber, Nucl. Instr. and Meth. A 380 (1996) 385. [4] L. Verger, J.P. Bonnefoy, F. Glasser, P. Ouvrier-Bu!et, J. Electron. Mater. 26 (1997) 738. C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 [5] H.B. Barber, B.A. Apotovsky, F.L. Augustine, H.H. Barrett, E.L. Dereniak, F.P. Doty, J.D. Eskin, W.J. Hamilton, D.G. Marks, K.J. Matherson, J.E. Venzon, J.M. Woolfenden, E.T. Young, Nucl. Instr. and Meth. A 395 (1997) 421. [6] W.W. Moses, S.E. Derenzo, T.F. Budinger, Nucl. Instr. and Meth. A 353 (1994) 189. [7] P. Si!ert, Nucl. Instr. and Meth. A 253 (1978) 1. [8] E. Raiskin, J.F. Butler, IEEE Trans. Nucl. Sci. NS-35 (1988) 81. [9] F.P. Doty, J.F. Butler, J. Schetina, K. Bowers, in: D.E. Seiler (Ed.), Proceedings of the 1991 US Workshop on the Physics and Chemistry of HgCdTe and Other II}VI Compounds J. Vac. Sci. Technol. B 10 (1992) 1418. [10] K. Chattopadhay, H. Chen, K.T. Chen, A. Burger, J.P. Flint, H.L. Glass, R.B. James, Mater. Res. Soc. Symp. Proc. 487 (1998) 123. [11] K.G. Lynn, M. Weber, H.L. Glass, J.P. Flint, C.S. Szeles, Mater. Res. Soc. Symp. Proc. 487 (1998) 229. [12] J.F. Butler, Nucl. Instr. and Meth. A 396 (1997) 396. [13] Z. He. G.F. Knoll, D.K. Wehe, Y.F. Du, Nucl. Instr. and Meth. A 411 (1998) 107. [14] J.A. Heanue, J.K. Brown, B.H. Hasegawa, IEEE Trans. Nucl. NS-44 (1997) 701. [15] L. Verger, J.P. Bonnefoy, A. Gliere, P. Ouvrier-Bu!et, M. Rosaz, Mater. Res. Soc. Symp. Proc. 487 (1998) 171. [16] U. Lachish, Nucl. Instr. and Meth. A 403 (1998) 51. [17] R.B. James, J. Lund, E. Cross, M. Schieber et al., J. Electron. Mater. 27 (1998) 788. [18] Y. Eisen, A. Schor, C. Gilath, M. Tsabarim, P. Chouraqui, C. Hellman, E. Lubin, Nucl. Instr. and Meth. A 380 (1996) 474. [19] Y. Eisen, A. Shor, J. Crystal Growth 185 (1998) 1302. [20] C. Scheiber, B. Eclancher, J. Chambron, V. Prat, A. Kazandjan, A. Jahnke, R. Matz, S. Thomas, S. Warren, M. Hage-Ali, R. Regal, P. Si!ert, M. Karman, Nucl. Instr. and Meth. A 428 (1999) 138. [21] N. Arques, N. Ba!ert, D. Lattard, J.L. Martin, G. Masson, F. Mathy, A. Noca, J.P. Rostaing, P. Trystram, P. Villard, J. Cretolle, F. Lebrun, J.P. Leray, IEEE Trans. Nuc. Sci. 46 (1999) 181. [22] J.F. Butler C.L. Lingren, S.J. Friesenhahn, F.P. Doty, W.L. Ashburn, R.L. Conwell, F.L. Augustine, B. Apotovsky, B. Pi, T. Collins, S. Zhao, C. Issacson, IEEE Trans. Nucl. Sci. NS-45 (1998) 359. [23] F.L. Augustine, Nucl. Instr. and Meth. A 353 (1994) 201. [24] J.F. Butler, S.J. Friesenhahn, C. Lingren, B. Apotovsky, R. Simchon, F.P. Doty, Proceedings of the IEEE Transactions of Nuclear Science, San Francisco, CA, November 2}6, 1993, p. 345. [25] J.D. Eskin, H.H. Barrett, H.B. Barber, J.M. Woolfenden, Phys. Rev. Lett. 5 (1994) 156. [26] F.P. Doty, H.B. Barber, F.L. Augustine, J.F. Butler, B.A. Apotovsky, E.T. Young, W. Hamilton, Nucl. Instr. and Meth. A 353 (1994) 356. 523 [27] M.M. Rogulski, H.B. Barber, H.H. Barrett, R.L. Shoemaker, J.M. Woolfenden, IEEE Trans. Nucl. Sci. NS-40 (1993) 1123. [28] H.B. Barber, H.H. Barrett, E.L. Dereniak, N.E. Hartsough, D.L. Perry, P.C.T. Roberts, M.M. Rogulski, J.M. Woolfenden, E.T. Young, IEEE Trans. Nucl. Sci. NS-40 (1993) 1140. [29] K.J. Mattershon, H.B. Barber, H.H. Barrett, J.D. Eskin, E.L. Dereniak, D.G. Marks, J.M. Woolfenden, E.T. Young, F.L. Augustine, IEEE Trans. Nucl. Sci. NS-45 (1998) 354. [30] M. Singh, Med. Phys. 10 (1983) 421. [31] P.H. Kramer, P. Kind, S. Gaspers, Phys. Med. 14 (1998) 31. [32] M. Singh, F.P. Doty, S.J. Friesenhahn, J.F. Butler, IEEE Trans. Nucl. Sci. NS-42 (1995) 1139. [33] M.G. Scannavini, R.D. Speller, G.J. Royle, I. Cullum, M. Raymond, G. Hall, G. Iles, IEEE NSS-MIC conference records, 1998. [34] L. Cirignano, K.S. Shah, P.R. Bennett, M. Klugerman, Y. Dmitryev, M.R. Squillante, T. Narita, P. Bloser et al., Nucl. Instr. and Meth. A 422 (1999) 216. [35] K. Iwata, B.H. Hasegawa, J.A. Heanue, P.R. Bennett, K.S. Shah, C.D. Boles, B.E. Boser, Nucl. Instr. and Meth. A 422 (1999) 740. [36] J. Taki, A. Muramori, K. Nakajima, H. Bunko, M. Kawasuji, N. Tonami, K. Hisada, J. Nucl. Med. 33 (1992) 441. [37] J. Taki, K. Nakajima, M. Shimizu, N. Tonami, K. Hisada, J. Nucl. Med. 35 (1994) 1937. [38] C. Scheiber, M. Karim, C. Draman, P. Attali, P. Si!ert, J. Chambron, Proceedings of the IEEE-EMBS 14th Annual Conference, Paris, October 29}31, 1992, p. 707. [39] K. Karim, C. Scheiber, C. Draman, P. Attali, P. Si!ert, J. Chambron, Proceedings of the IEEE-EMBS 14th Annual Conference, Paris, October 29}31, 1992, p. 711. [40] W.G. Myers, J.C. Vanderleeden, J. Nucl. Med. 1 (1960) 149. [41] X. Marchandise, D. Huglo, H. Bedoui, C. HosseinFoucher, J. Rousseau, Ann. Chir. 4 (1995) 317. [42] A. Perkins, Eur. J. Nucl. Med. 20 (1993) 573. [43] M.O. Thurston, in: E.W. Martin (Ed.), Radioimmunoguided surgery in the detection and treatment of colorectal cancer, Landes Company 42, 1994. [44] M.W. Arnold, S. Schneebaum, A. Berens, C. Mojzicik, G. Hinkle, E.W. Martin, Surgery 112 (1992) 624. [45] E. Martin, D.A. Martinez, M.S. O'Dorisio, T.M. O'Dorisio, D.R. King, R.C. Orahood, G.H. Hinkle, J.A. Barnes, M.O. Thurston, in: E.W. Martin (Eds.), Radioimmunoguided Surgery in the detection and treatment of colorectal cancer, Landes Company, 172, 1994. [46] P.L. Triozzi, J.A. Kim, W. Aldrich, D.C. Young, J.W. Sampsel, E.W. Martin, Cancer 73 (1993) 580. [47] R.A. Badalament, J.K. Burgers, L.R. Petty, C.M. Mojzisik, A. Berens, Cancer 71 (1993) 2268. [48] E.A. Wotering, R. Barrie, T. O'Dorisio, M.S. O'Dorisio, R. Nance, D.M. Cook, Surgery 116 (1994) 1139. 524 C. Scheiber / Nuclear Instruments and Methods in Physics Research A 448 (2000) 513}524 [49] N.P. Alasraki, D. Eshima, L.A. Eshima et al., Semin. Nucl. Med. 27 (1997) 55. [50] D.L. Morton, D.R. Wen, J.H. Wong, J.S. Economus, L.A. Cagle, F.K. Storm et al., Arch. Surg. 127 (1992) 392. [51] T. Tiourina, B. Arends, H. Rutten, B. Lemaire, S. Muller, Eur. J. Nucl. Med. 25 (1998) 1224. [52] A.J. Britten, Eur. J. Nucl. Med. 26 (1999) 76. [53] H. Bedoui, J. Rousseau, P. Masquelier, X. Marchandise, Proceedings of the IEEE -EMSBS Conference, Montreal, 1995, p. 34. [54] R.A. Valdes Olmos, C.A. Hoefnagel, O.E. Nieweg, L. Jansen, E.J. Rutgers, J. Borger et al., Eur. J. Nucl. Med. 26 (1999) S3. [55] P.J. Ell, (Ed. in Chief) Eur. J. Nucl. Med. 26 (1999) 435.