Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
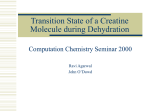
gonadotropin on muscle strength and physical function and activity in older men with partial age-related androgen deficiency. J Clin Endo Metab 2002;87:31253135. over 80 years.3 It has been estimated that a 10% reduction in the prevalence of sarcopenia in the United States could save more than $1 billion per year.4 Resistance training is effective at counteracting sarcopenia, as is testosterone administration.2 However, concerns about the latter’s adverse effects have led to interest in other, safer interventions, with creatine supplementation of major interest. Given the prevalence of sarcopenia, and an aging population, this article will review the available evidence on creatine supplementation to reduce age-related loss of muscle mass and strength. 12. Lijesen GK, et al. The effect of human chorionic gonadotropin (HCG) in the treatment of obesity by means of the Simeons therapy: A criteria-based meta-analysis. Br J Clin Pharmacol 1995;40:237-243. 13. Stein MR, et al. Ineffectiveness of human chorionic gonadotropin in weight reduction: A double-blind study. Am J Clin Nutr 1976;29:940-948. 14. Shetty KR, Kalkhoff RK. Human chorionic gonadotropin (HCG) treatment of obesity. Arch Intern Med 1977;137:151-155. Background Creatine is synthesized in the body from the amino acids arginine, glycine, and methionine. Adults generally make 1-2 g of creatine daily, which is later broken down to creatinine and excreted at a rate of about 2 g per day.2 To provide for additional needs, creatine can be obtained from the diet, especially from meat and seafood.3 After synthesis or ingestion, creatine is transported primarily to skeletal muscle where about 95% of the body’s creatine is stored. About two-thirds of the creatine in skeletal muscle exists as creatine phosphate (CP), with the remainder found as free creatine.1 As muscles work, CP is used to replenish adenosine triphosphate (ATP) (see Figure). ATP is the muscle’s biochemical energy molecule and is converted to ADP as its energy is used. Muscles normally store enough ATP for only a few seconds of exertion, after which CP can provide fuel for an additional 4-6 seconds of intense exercise. This all depends on the muscle’s free creatine concentration. Hence, it has been hypothesized that if supplementation increased the muscle’s creatine levels, more energy would be available during exercise. 15. Bosch B, et al. Human chorionic gonadotrophin and weight loss. A double-blind, placebo-controlled trial. S Afr Med J 1990;77:185-159. Creatine and Age-Related Loss of Muscle Mass and Strength By Dónal P. O'Mathúna, PhD Senior Lecturer in Ethics, Decision-Making & Evidence, School of Nursing & Human Sciences, Dublin City University, Ireland Dr. OMathúna reports no financial relationships relevant to this field of study. C reatine remains one of the most popular supplements for athletes, especially to enhance power and speed. A large body of research evidence supports claims that creatine enhances power output during short maximal bursts of exercise, such as power lifting or sprinting.1 The benefits are noted particularly when short exertions are repeated intermittently in what is called interval training. However, some benefits also have been found for endurance exercise. Although much of the focus on creatine has been on athletes, maintaining muscle mass and strength is also important for older adults. Aging is associated with loss of muscle mass and decreased strength, which can negatively impact activities of daily living and quality of life.2 Such changes can increase the risk of falls, which can be a major problem with aging. Sarcopenia refers to a condition that occurs when fatfree mass is more than two standard deviations below normal.3 Approximately 25% of those older than 70 years of age have sarcopenia, increasing to nearly half of those Alternative Medicine Alert Figure ATP Contraction ADP + Pi Creatine Phosphate Creatine + Pi 17 Table Biomarker % increase in subjects 18-36 years % increase in subjects 52-79 years Total creatine 21.7 14.9 CP 13.3 8.2 Free creatine 39.3 28.6 ATP 4.2 6.8 Mechanism of Action Muscle mass and strength decrease by about 1-2% per year after age 50.3 The number of muscle fibers decreases, but especially type II (or fast-twitch) fibers, which are replaced by intramuscular fat.4 Type II fibers are particularly high in creatine and CP content. Thus, normal aging and muscle loss reduces stored creatine levels, leaving less energy available for exercise. Creatine supplementation in older adults is thought to increase creatine and CP levels in muscles, allowing people to exercise longer and at higher intensities, thus stimulating growth in muscle mass and strength. Changes in these physiological parameters have been measured in several studies of both younger and older subjects after creatine supplementation. The results of a meta-analysis of such studies are presented in the Table showing how creatine supplementation impacts these biomarkers.4 Clinical Studies Creatine was first identified in 1832 and its metabolism was studied extensively over the next century.2 Subsequently, interest faded until the British sprinter, Linford Cristie, revealed in 1992 that he had taken creatine during the preparations that led up to his Olympic gold medal.2 Shortly afterwards, studies demonstrated that creatine supplements did increase muscle creatine levels and exercise performance.5 Since then, several hundred studies have been published on the topic.2 Much of the interest in creatine for older adults is derived from extrapolations from the sports science research. The first double-blind study to examine creatine use with resistance training in elderly, sedentary adults was published in 1998.6 Thirty-two men and women (67-80 years old) were randomized into four groups: creatine with resistance training, placebo with training, creatine without training, and placebo without training. None of the participants did weight-lifting before the study, and all were sedentary-to-moderately active. Creatine dose was 20 g/day for 5 days, followed by 3 g/day for a total of 8 weeks. Resistance training was carried out three times a 18 week. No significant changes in body mass or body fat were found in any group. Training groups had significantly increased strength and endurance compared to those not training (P < 0.02). Creatine supplementation did not provide any additional benefit. Three reviews have recently been published and identified a total of 12 relevant trials.2-4 All 12 studies were randomized, placebo-controlled, and double-blinded. They were similar in enrolling around 20-40 subjects older than age 65 years and either used a creatine protocol similar to that described above or gave subjects 5 g/day for a number of months. The longest study, which lasted 1 year, reported no significant differences between its groups.7 Out of the 12 studies, seven found significant beneficial effects on fat-free muscle mass and/or strength, and five found no beneficial effects on muscle mass or strength. The results of all these studies have not been combined into a meta-analysis. Most studies giving creatine supplements without exercise found beneficial effects on muscle mass and strength, but some found no benefits. About half the studies included resistance training programs, again with the majority showing significant benefits, but some not. All of the reviews concluded that creatine supplementation, particularly with resistance training, can have beneficial effects on muscle wasting in older men and women. However, the effects are not consistent, suggesting that other variables need to be considered. Since resistance training itself is known to have beneficial effects, most reviewers recommend combining creatine supplements with exercise. Some studies have examined the timing of creatine ingestion and suggested that this may be more important than the actual dose of creatine.8 Exercise stimulates muscle protein degradation and synthesis. Synthesis predominates when protein or amino acids are ingested shortly before or after exercise, hence the current popularity of protein shakes being consumed by athletes immediately after workouts. Part of the reason for these effects is increased blood flow to muscles after exercise. This has been hypothesized as a way to more efficiently transport ingested creatine to muscles. A small number of studies have found that ingesting creatine immediately before and after exercise leads to greater gains in muscle mass than when creatine is ingested in the morning and evening, away from training times.3 Adverse Effects Creatine supplementation among athletes frequently leads to a 1-3 kg weight gain, probably due to intramuscular water retention.9 Concerns often are raised about cramping when creatine is taken in conjunction with exercise, although this has not been supported by studies.1 Anecdotal reports claim creatine supplementation can February 2012 cause gastrointestinal problems, though these are not frequently reported in studies. One study with older men found significantly more reports of loose stools during creatine loading than with placebo, and during maintenance dosing, more muscle cramping and strains with creatine.10 Occasional case reports report more serious adverse affects, in particular involving renal and hepatic function, but evidence to support these have not been found in studies.11 However, those with renal disease or at risk of renal dysfunction are usually recommended to avoid creatine supplementation or monitor renal function carefully if creatine is taken.1 to exercise may enhance these effects. Adequate hydration is important to avoid cramping problems. In addition, preliminary results suggest that creatine may have other beneficial effects during aging, particularly a slowing of cognitive decline.2 However, the equivocal nature of the results to date suggest either that only some people benefit from creatine supplementation, or that more needs to be understood about how creatine is administered. It appears that taking creatine immediately before or after exercise may be more important than how much is taken. While creatine supplements are safe, similar benefits may be obtained from dietary creatine, such as by eating a meal with red meat or seafood immediately before or after exercise. n Drug Interactions No drug interactions are known, although concerns about the potential for renal toxicity raise issues about drugs metabolized through the kidneys. References 1. Maughan RJ, et al. Dietary supplements for athletes: Emerging trends and recurring themes. J Sports Sci 2011;29(Suppl 1):S57-S66. Formulation Creatine is readily available from meat and fish (containing roughly 4-5 g/kg), and therefore, is classified as a dietary supplement, not a drug. As a supplement, it is most commonly available as a monohydrate in powder, candy, gum, and liquid. Many synthetic derivatives are available, including creatine malate, creatine pyruvate, creatine citrate, creatine-magnesium chelate, creatine ethyl ester, and many more. Claims that any one of these is more effective than another have not been supported in the few independent assessments available.1 Numerous products combine creatine with vitamins, nutrients, and other supplements, but clinical studies of these were not identified. Athletes usually “load” with 20-25 g creatine per day for 5-7 days (usually 5 g qid), followed by one 2 g daily dose. Studies with older people have used this regimen, or they were given 2-5 g per day. 2. Rawson ES, Venezia AC. Use of creatine in the elderly and evidence for effects on cognitive function in young and old. Amino Acids 2011;40:1349-1362. 3. Candow DG. Sarcopenia: current theories and the potential beneficial effect of creatine application strategies. Biogerontolog 2011;12:273-281. 4. Dalbo VJ, et al. The effects of age on skeletal muscle and the phosphocreatine energy system: Can creatine supplementation help older adults. Dyn Med 2009;8:6. 5. Greenhaff PL, et al. Influence of oral creatine supplementation of muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571. 6. Bermon SP, et al. Effects of creatine monohydrate ingestion in sedentary and weight-trained older adults. Acta Physiol Scand 1998;164:147-155. 7. Eijnde BO, et al. Effects of creatine supplementation and exercise training on fitness in men 55-75 yr old. J Appl Physiol 2003;95:818-828. Conclusion Numerous studies of creatine supplementation by athletes have demonstrated beneficial effects on muscle mass and strength after high-intensity exercise. Such research with older adults is less extensive. Most, but not all, studies support a beneficial effect on muscle mass and strength either with or without resistance exercise. It remains unclear whether muscle creatine storage decreases with age, or whether this is a function of reduced activity and dietary creatine intake. If it is the latter, this may explain some of the variability obtained in the studies conducted to date. 8. Candow DG, Chilibeck PD. Timing of creatine or protein supplementation and resistance training in the elderly. Appl Physiol Nutr Metab 2008;33:184-190. 9. Branch JD. Effect of creatine supplementation on body composition and performance: A meta-analysis. Int J Sport Nutr Exerc Metabol 2003;13:198-226. 10. Chrusch MJ, et al. Creatine supplementation combined with resistance training in older men. Med Sci Sports Exerc 2001;33:2111-2117. 11. Persky AM, Rawson ES. Safety of creatine supplementation. Subcell Biochem 2007;46:275-289. Recommendation Resistance training is beneficial in preventing or reversing the loss of muscle mass and strength that occurs with aging. Creatine supplementation alone or in addition Alternative Medicine Alert 19 Copyright of Alternative Medicine Alert is the property of AHC Media LLC and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.