Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
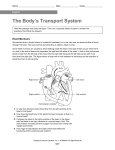
Page 1 of 5 Clinical Anatomy Critical review Clinical anatomy of the fourth ventricle foramina Abstract Introduction The three foramina of the fourth ventricle of the human brain were first described during the 19th century. The primary purpose of this article was to review the anatomy of the foramina of the human fourth ventricle, as well as the main clinical conditions related to pathology of these neurosurgically important structures. The existing literature regarding the gross and neurosurgical anatomy of the foramina of the human fourth ventricle was reviewed with emphasis on the clinical disorders caused by several pathological conditions of these structures. Neuroanatomical comments on the location of these foramina are also provided. Discussion The fourth ventricle is connected through the foramen of Magendie with vallecula cerebelli and cisterna magna, and laterally through the foramina of Luschka with the cerebellopontine angles. The foramen of Magendie is probably the main path for the outflow of the cerebrospinal fluid from the ventricle. The Luschka foramina are found (at or) above the pontomedullary junction. The right Luschka foramen seems to be located slightly more superior and more posterior as compared to the left. Neuroendoscopy offers a detailed visualisation, particularly of the structures located in the inferior triangle of the fourth ventricle. The main pathological conditions affecting the foramina of the fourth ventricle are usually associated with hydrocephalus (responsible for clinical manifestations) and include occlusion, membrane obstruction, congenital imperforation, idiopathic *Corresponding author Email: [email protected] 1 Department of Neurology, ‘K.A.T.-N.R.C.’ General Hospital of Attica, Athens, Greece stenosis, arachnoid adhesions and cystic dilation. Conclusion The foramina of the fourth ventricle, anatomically delicate and neurosurgically crucial apertures, have close relations with several important structures of the brainstem and cerebellum. Slight differences seem to exist between the two sides regarding the location of the Luschka foramen. Pathological conditions affecting the foramina of the fourth ventricle usually produce clinical manifestations due to obstruction of the cerebrospinal fluid normal flow. Microsurgical treatment of such rare but challenging lesions is nowadays feasible. Introduction The three foramina of the fourth ventricle of the human brain were first described during the 19th century1,2. The foramen of Magendie is named after the French physiologist François Magendie (1783-1855) who is considered a pioneer of experimental physiology1. The foramina of Luschka are named after the German anatomist Hubert von Luschka (1820-1875) who lent his name to several structures2. In 1931, Rogers and West3 described the anatomy and relations of the foramen of Magendie, presenting it as a complete defect in the lower part of the ventricular roof through which the fourth ventricle is in free communication with the cisterna magna3. In 1948, Barr4 reported observations on the foramen of Magendie in a series of human brains4. Half century later, Rhoton5 provided detailed descriptions of the neurosurgical anatomy of the fourth ventricle and its foramina5. The primary purpose of this article was to review the anatomy of the foramina of the human fourth ventricle, as well as the main clinical conditions related to pathology of these neurosurgically important structures. The existing literature regarding the gross and neurosurgical anatomy of the foramina of the human fourth ventricle was reviewed with emphasis on the clinical disorders caused by several pathological conditions affecting these structures. Neuroanatomical comments on the location of these foramina are also provided. Discussion The author has referenced one of his own studies in this review. This referenced study has been conducted in accordance with the Declaration of Helsinki (1964) and the protocols of this study have been approved by the relevant ethics committees related to the institution in which it was performed. Anatomy and morphometry The fourth ventricle is a broad, tentshaped midline cavity located between cerebellum and brainstem. It is connected rostrally through the cerebral aqueduct (of Sylvius) with the third ventricle, caudally with the spinal canal and through the foramen of Magendie with vallecula cerebelli (a cleft between the cerebellar tonsils) and cisterna magna, and laterally through the foramina of Luschka with the cerebellopontine angles. It has a roof, a floor and two lateral recesses5. The roof expands laterally and posteriorly from its narrow rostral end just below the aqueduct to the level of the fastigium and lateral recess, the site of its greatest height and width, and from there it tapers to a narrow caudal apex at the level of the foramen of Magendie5. The floor has a rhomboid shape. Its cranial apex is at the level of the cerebral aqueduct; its caudal tip, the obex, is located at the rostral end of the remnant of the spinal canal, anterior to the foramen of Magendie; and its lateral angles open through the lateral Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY) FOR CITATION PURPOSES: Mavridis IN. Clinical anatomy of the fourth ventricle foramina. OA Anatomy 2014 Apr 09;2(1):9. Competing interests: None declared. Conflict of interests: None declared. All authors contributed to conception and design, manuscript preparation, read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. IN Mavridis1* Page 2 of 5 Critical review The choroid plexus of the fourth ventricle consists of several segments. Its lateral segments extend laterally through the foramina of Luschka (protruding into the cerebellopontine angle below the flocculus and behind the glossopharyngeal, vagus and accessory nerves) and its medial segments extend longitudinally through the foramen of Magendie. The medial segments stretch from the level of the nodule, anterior to the cerebellar tonsils, to the level of the foramen of Magendie. The tonsillar parts of the choroid plexus are located anterior to the tonsils and extend inferiorly through the foramen of Magendie5. Ciołkowski et al.6 described the median aperture (foramen) of Magendie as the largest of the three openings of the fourth ventricle and thus forming the main path for the outflow of the cerebrospinal fluid (CSF) from the ventricle. The Magendie foramen makes a natural corridor for neurosurgical approach and inspection of the fourth ventricle and its floor6. According to the same authors6, this foramen is limited by the following structures: obex and gracile tubercles inferiorly and tela choroidea with choroid plexus superolaterally. Obex tubercles usually have the form of a piece of neural tissue bridging two halves of the brainstem above the entrance to the central canal. Gracile tubercles together are 8.15 mm wide and the maximal width of the foramen is 6.53 mm. Tela choroidea attaches laterally at both sides to the inferior medullary velum. In most cases the right and left choroid plexuses are connected to each other with a triangular membrane of tela choroidea, which protrudes through the median foramen and attaches to the vermis at a highly variable level6. Sharifi et al.7 studied 40 human cerebella and distinguished two compartments of the foramen of Luschka, namely the choroidal and patent part. Interestingly, 7.5% of the foramina were closed. The mean distance between the foramen of Luschka and the anterior inferior cerebellar artery was 3.9 mm. The distance from the posterior inferior cerebellar artery was 7.08 and 5.81 mm to the left and right foramina of Luschka, respectively. In ten cases, tortuous vertebral artery was occupying the left cerebellopontine angle space and the foramen of Luschka7. The Magendie foramen is, to the author’s gross anatomical experience, located 12 mm (9-15 mm) inferior to the pontomedullary junction, while the Luschka foramen is located 1.4 mm (0-11 mm) superior to this junction. The fourth ventricle extends ≥ 9 mm inferior and the Luschka foramina are located superior to this junction (37% placed exactly at this level). The Magendie foramen is located 0.3 mm (0-2 mm) posterior to the fourth ventricle floor, while the Luschka foramen is located 1.3 mm (0-4 mm) posterior to this floor (16% of the Luschka and 83% of the Magendie foramina were found at the level of this floor). Interestingly, the right Luschka foramen seems to be located 1.5 mm more superior from the pontomedullary junction and 0.7 mm more posterior from the fourth ventricle floor as compared to the left. Longatti et al.8 examined the access to the fourth ventricle achieved by the endoscopic transaqueductal approach, to enumerate and describe the anatomically identifiable landmarks and to compare them with those described during microsurgery. Twenty anatomical structures could consistently be identified by exploring the fourth ventricle with a fiberscope, including the foramina of Luschka and Magendie. Neuroendoscopy offers a quite different outlook on the anatomy of the fourth ventricle, and compared with the microsurgical descriptions it seems to provide a superior and detailed visualisation, particularly of the structures located in the inferior triangle8. Clinical conditions There are several pathological conditions of the fourth ventricle foramina, congenital or acquired, which usually cause hydrocephalus (principally responsible for clinical manifestations), mainly due to obstruction of the normal CSF flow. Occlusion of the foramen of Magendie (e.g. by a plexus ependymal cyst) can cause hydrocephalus9. In children, occlusion of the foramen of Magendie is usually the consequence of DandyWalker cysts10 or Arnold-Chiari type I malformation11. In adults, the occlusion is rather acquired than congenital, linked to infection, head trauma, intraventricular haemorrhage, tumours or Arnold-Chiari malformation. In rare cases, in children as well as in adults, obstructive hydrocephalus has been reported due to the occlusion of the foramen of Magendie by a membrane, likely to be an extension of the inferior medullary velum and the tela choroidea. Until now, the diagnosis was suggested on indirect data, confirmed by invasive procedures such as ventriculography or direct surgical exploration10. Cystic malformations in the posterior cranial fossa result from developmental failure in the paleocerebellum and meninges12. Takami et al.12 reported a case of an infant with hydrocephalus associated with cystic dilation of the foramina of Magendie and Luschka. This 7-month-old female infant presented with sudden onset of tonicclonic seizures. Computed tomography (CT) scan revealed quadri-ventricular hydrocephalus. Magnetic resonance imaging (MRI) demonstrated a cyst communicating with the fourth Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY) FOR CITATION PURPOSES: Mavridis IN. Clinical anatomy of the fourth ventricle foramina. OA Anatomy 2014 Apr 09;2(1):9. Competing interests: None declared. Conflict of interests: None declared. All authors contributed to conception and design, manuscript preparation, read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. recesses and foramina of Luschka5. The foramen of Luschka opens into the cerebellopontine angle below the junction of the facial and vestibulocochlear nerves with the lateral end of the pontomedullary sulcus5. The lateral recesses are narrow, curved pouches formed by the union of the roof and the floor. They extend laterally below the cerebellar peduncles. The anterior inferior cerebellar artery is intimately related to the lateral recess and the foramen of Luschka5. Page 3 of 5 Critical review Three weeks later, however, the hydrocephalus recurred. An endoscopic third ventriculocisternostomy was performed to address the possibility of stagnant CSF flow in the posterior cranial fossa, but the hydrocephalus continued. Finally the patient underwent placement of a ventriculoperitoneal shunt, resulting in resolution of the hydrocephalus. The authors speculated that the cystic malformation in their patient could be classified in a continuum of persistent Blake pouch cysts. Hydrocephalus was caused by a combination of obstruction of CSF flow at the outlets of the fourth ventricle and disequilibrium between CSF production and absorption capacity12. A membrane obstruction of the foramina of Magendie and Luschka is an uncommon origin of hydrocephalus characterised by unusual clinical symptoms of rhomboid fossa hypertension. Various surgical approaches have been proposed to alleviate this obstruction, including opening the obstructed foramen of Magendie using suboccipital craniectomy, shunting procedures and more recently, endoscopic third ventriculostomy (ETV). In some cases, however, reshaping of the posterior fossa due to the collapse of the prepontine cistern could make ETV difficult for the surgeon and dangerous to the patient. In these cases, endoscopic opening of the foramen of Magendie by transaqueductal navigation of the fourth ventricle is a suitable and feasible therapeutic option13. Rougier and Ménégon10 reported a case of a 61-year-old man who developed headaches for several months and more recently an unsteady gait. The CT scans showed quadri-ventricular hydrocephalus involving mainly the fourth ventricle with dilated lateral recesses but without an Arnold-Chiari malformation. A membrane occluding the foramen of Magendie was demonstrated on the MRI. At operation, the tonsils appeared normal and were easily separated to expose the vallecula. In the area of the foramen of Magendie the fourth ventricle was hermetically sealed by a strong membrane in continuation with the tela choroidea. The membrane was excised resulting in free flow of CSF. After surgery, the headaches resolved immediately whereas the gait returned to normal within one month. At six months following operation, the ventricular size was normal on the controlled CT scan10. Congenital membranous obstruction of the foramen of Magendie is a rare entity14. Hashish et al.14 reported two cases (35 and 68 year-old) with chronic hydrocephalus due to congenital membranous obstruction of the foramen of Magendie. Both these patients presented with headaches, nausea, and impairment of gait and memory. CT and MRI examination showed a communicating hydrocephalus, with particular enlargement of the fourth ventricle. Both patients were operated on for microsurgical exploration of the outlet of the fourth ventricle, which demonstrated membranous obstruction of the foramen of Magendie. Microsurgical perforation of the foramen of Magendie was performed, and a ventriculo-cisternal shunt was left in place. The two patients were cured14. Despite its rare occurrence, congenital imperforation or membranous obstruction of the foramen of Magendie must be considered as a possible etiology of chronic hydrocephalus in adult, especially in case of non proportioned enlargement of the fourth ventricle, associated to signs of increased intracranial pressure14. According to Hashish et al.14, the best curative surgical procedure consists in a microsurgical exploration of the foramen of Magendie associated to a ventriculo-cisternal shunting (from the fourth ventricle to the cisterna magna) and has more advantages than a simple ventriculo-peritoneal shunting14. Tubbs15 reported a young girl who presented with headache and back pain. Dynamic MRI revealed no cerebrospinal egress from the median aperture (foramen of Magendie) of the fourth ventricle and syringomyelia. A posterior cranial fossa exploration was performed and agenesis of the median aperture was observed. Following surgical penetration of the posterior aspect of the fourth ventricle and at the most recent follow-up examination, this patient's syringomyelia had resolved, as had her symptoms. Agenesis of the foramen of Magendie may be a rare cause of inhibition of normal CSF egress from the fourth ventricle with resultant syringomyelia15. Idiopathic stenosis of the foramina of Magendie and Luschka is a rare cause of obstructive hydrocephalus involving the four ventricles. Like other causes of non-communicating hydrocephalus, it can be treated with ETV16. Karachi et al.16 reported three patients (21, 53 and 68 years of age) presenting with either headaches (with or without raised intracranial pressure) or vertigo, or a combination of gait disorders, sphincter disorders and disorders of higher functions. In each case, MRI demonstrated hydrocephalus involving the four ventricles with no signs of an Arnold-Chiari type I malformation. The diagnosis of obstruction was confirmed using ventriculography and/or MR flow images. All patients presented with marked dilation of the foramen of Luschka that herniated into the cisterna pontis. All patients were Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY) FOR CITATION PURPOSES: Mavridis IN. Clinical anatomy of the fourth ventricle foramina. OA Anatomy 2014 Apr 09;2(1):9. Competing interests: None declared. Conflict of interests: None declared. All authors contributed to conception and design, manuscript preparation, read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. ventricle and projecting to the cisterna magna and the cerebellopontine cisterns through the foramina of Magendie and Luschka. A suboccipital craniotomy was performed for removal of the cyst wall and the transparent membrane covering the foramen of Magendie was removed under a microscope. After the surgery, the patient's hydrocephalus improved and a phase contrast cine MRI study showed evidence of normal CSF flow at the level of the third and fourth ventricles. Page 4 of 5 Critical review Finally, Rahme et al.17 reported a unique case of a 38-year-old male with cervical syringomyelia resulting from spontaneous regeneration of the posterior C1 arch three years after foramen magnum decompression. Neo-ossification of the posterior arch of C1 and thick arachnoid adhesions were found to obstruct cerebrospinal fluid flow through the foramen of Magendie. Foramen magnum decompression, arachnoid dissection and duraplasty were thus performed and CSF flow was reestablished through the foramen of Magendie17. Table 1 summarises the main pathological conditions affecting the foramina of the fourth ventricle. Conclusion The foramina of the fourth ventricle (Figure 1) are anatomically delicate and neurosurgically (neuroendoscopically) crucial parts of the ventricular system of the brain. They have close relations with several important structures of the brainstem and cerebellum. Slight differences seem to exist between the two sides regarding the location of the Luschka foramen. Pathological conditions affecting the foramina of the fourth ventricle (congenital or acquired) usually produce clinical manifestations due to obstruction of the normal flow of the CSF. Microsurgical treatment of such rare but challenging lesions is nowadays feasible. Table 1: Main pathological conditions affecting the foramina of the fourth ventricle 1 Occlusion (e.g. infection, head trauma, intraventricular haemorrhage,spaceoccupying lesions, congenital anomalies) 2 Membrane obstruction 3 Congenital imperforation (agenesis) 4 Idiopathic stenosis 5 Arachnoid adhesions 6 Cystic dilation Figure 1: The location of the foramina of the fourth ventricle (human brain, right hemisphere, fourth ventricle area). 1: arbour vitae, 2: posterior commissure, 3: cerebellar tonsil, 4: lingula, 5: midbrain, 6: superior medullary velum, 7: quadrigeminal cistern (of the great cerebral vein), 8: roof of the fourth ventricle, 9: cerebral aqueduct (of Sylvius), 10: pons, 11: fourth ventricle, 12: cerebellar hemisphere, L: right foramen of Luschka, M: foramen of Magendie 18 (line: intercommissural line) (modified from Mavridis ). Abbreviations list CSF, cerebrospinal fluid; CT, computed tomography; ETV, endoscopic third ventriculostomy; MRI, magnetic resonance imaging. References 1. Wikipedia, the free encyclopedia. François Magendie. Available from: http:en.wikipedia.org/wiki/Fran%C3 %A7ois_Magendie; 2014 [accessed 5 March 2014]. 2. Wikipedia, the free encyclopedia. Luschka. Available from: http:en.wikipedia.org/wiki/Luschka; 2014 [accessed 5 March 2014]. 3. Rogers L, West CM. The Foramen of Magendie. J Anat. 1931 Jul;65(Pt 4):457-67. 4. Barr ML. Observations on the foramen of Magendie in a series of human brains. Brain. 1948 Sep;71(Pt. 3):281-9. 5. Rhoton AL Jr. Cerebellum and fourth ventricle. Neurosurgery. 2000 Sep;47(3 Suppl):S7-27. 6. Ciołkowski M, Sharifi M, Tarka S, Ciszek B. Median aperture of the fourth Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY) FOR CITATION PURPOSES: Mavridis IN. Clinical anatomy of the fourth ventricle foramina. OA Anatomy 2014 Apr 09;2(1):9. Competing interests: None declared. Conflict of interests: None declared. All authors contributed to conception and design, manuscript preparation, read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. uncomplicatedly treated using ETV, became asymptomatic within weeks following surgery and remained stable at a mean follow-up interval of 36 months. Postoperative MRIs demonstrated regression of the hydrocephalus, resolution of dilation of the foramen of Luschka and good patency of the ventriculostomy (flow sequences). These results confirm the existence of hydrocephalus caused by idiopathic fourth ventricle outflow obstruction without an associated Arnold-Chiari type I malformation and the efficacy of ETV for this rare indication16. Page 5 of 5 Critical review foramina of Magendie and Luschka. Report of three cases. J Neurosurg. 2003 Apr;98(4):897-902. 17. Rahme R, Koussa S, Samaha E. C1 arch regeneration, tight cisterna magna, and cervical syringomyelia following foramen magnum surgery. Surg Neurol. 2009 Jul;72(1):835;discussion 85-6. 18. Mavridis IN. [Stereotactic neurosurgical anatomy of the nucleus accumbens]. PhD Thesis, National and Kapodistrian University of Athens (School of Medicine), Athens, Greece, 2012, p 140. Greek. Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY) FOR CITATION PURPOSES: Mavridis IN. Clinical anatomy of the fourth ventricle foramina. OA Anatomy 2014 Apr 09;2(1):9. Competing interests: None declared. Conflict of interests: None declared. All authors contributed to conception and design, manuscript preparation, read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. ventricle revisited. Folia Morphol (Warsz). 2011 May;70(2):84-90. 7. Sharifi M, Ungier E, Ciszek B, Krajewski P. Microsurgical anatomy of the foramen of Luschka in the cerebellopontine angle, and its vascular supply. Surg Radiol Anat. 2009 Jul;31(6):431-7. 8. Longatti P, Fiorindi A, Feletti A, D'Avella D, Martinuzzi A. Endoscopic anatomy of the fourth ventricle. J Neurosurg. 2008 Sep;109(3):530-5. 9. Trummer M, Tillich M, Kleinert R, Unger F, Eustacchio S. Ependymal cyst occluding the Foramen Magendie. Acta Neurochir (Wien). 2000;142(5):601-2. 10. Rougier A, Ménégon P. MRI evidence of membranous occlusion of the foramen of Magendie. Acta Neurochir (Wien). 2009 Jun;151(6):693-4. 11. Santamarta D, Kusak ME, de Campos JM, Sierra JM. Increased cerebrospinal fluid flow through the foramen of Magendie after decompression for Chiari I malformation. J Neurol Neurosurg Psychiatry. 1999 Jun;66(6):799. 12. Takami H, Shin M, Kuroiwa M, Isoo A, Takahashi K, Saito N. Hydrocephalus associated with cystic dilation of the foramina of Magendie and Luschka. J Neurosurg Pediatr. 2010 Apr;5(4):415-8. 13. Longatti P, Fiorindi A, Feletti A, Baratto V. Endoscopic opening of the foramen of magendie using transaqueductal navigation for membrane obstruction of the fourth ventricle outlets. Technical note. J Neurosurg. 2006 Dec;105(6):924-7. 14. Hashish H, Guenot M, Mertens P, Sindou M. [Chronic hydrocephalus in an adult due to congenital membranous occlusion of the apertura mediana ventriculi quartii (foramen of Magendie). Report of two cases and review of the literature]. Neurochirurgie. 1999 Sep;45(3):2326. French. 15. Tubbs RS. Surgical observation of the agenesis of the foramen of Magendie. Folia Morphol (Warsz). 2006 May;65(2):174-7. 16. Karachi C, Le Guérinel C, Brugières P, Melon E, Decq P. Hydrocephalus due to idiopathic stenosis of the