Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
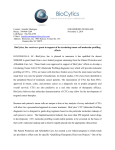
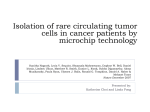
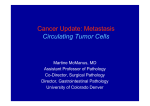
Circulating Stem Cell–Like Epithelial Cell Adhesion Molecule–Positive Tumor Cells Indicate Poor Prognosis of Hepatocellular Carcinoma After Curative Resection Yun-Fan Sun,1* Yang Xu,1* Xin-Rong Yang,1* Wei Guo,1,2 Xin Zhang,1 Shuang-Jian Qiu,1 Ruo-Yu Shi,1 Bo Hu,1 Jian Zhou,1,3 and Jia Fan1,3 Epithelial cell adhesion molecule–positive (EpCAM1) hepatocellular carcinoma (HCC) cells may constitute a tumor-initiating subpopulation in tumorigenic cell lines and HCC specimens. In the present study, EpCAM1 circulating tumor cells (CTCs) were identified prospectively in HCC patients undergoing curative resection, and the prognostic significance and their stem cell–like characteristics were investigated further. Blood samples from 123 HCC patients were tested prior to resection and 1 month thereafter. CTCs were present in 66.67% of patients, and the cell count measured in 7.5 mL of blood (CTC7.5) ranged between 1 and 34. Fifty-one patients had CTC7.5 of 2 preoperatively, and these patients developed tumor recurrence earlier than those with CTC7.5 of <2 CTCs (P < 0.001). A preoperative CTC7.5 of 2 was an independent prognostic factor for tumor recurrence (P < 0.001). Its prognostic significance also applied to patients with alpha-fetoprotein (AFP) levels of 400 ng/mL or subgroups with low recurrence risk (all P < 0.05). A significant decrease of CTC-positive rates (66.67% to 28.15%, P < 0.05) and CTC7.5 values (2.60 6 0.43 to 1.00 6 0.36, P < 0.05) was observed 1 month after resection. Patients with consistent CTC7.5 <2 had lower recurrence rates than those with values consistently 2 (15.5% versus 87.50%, P < 0.001). EpCAM1 CTCs displayed cancer stem cell biomarkers (CD133 and ABCG2), epithelial-mesenchymal transition, Wnt pathway activation, high tumorigenic potential, and low apoptotic propensity. Conclusion: Stem cell–like phenotypes are observed in EpCAM1 CTCs, and a preoperative CTC7.5 of 2 is a novel predictor for tumor recurrence in HCC patients after surgery, especially in patient subgroups with AFP levels of 400 ng/mL or low tumor recurrence risk. EpCAM1 CTCs may serve as a real-time parameter for monitoring treatment response and a therapeutic target in HCC recurrence. (HEPATOLOGY 2013;57:1458-1468) H epatocellular carcinoma (HCC) is one of the most prevalent malignancies worldwide, and associated morbidity and mortality rates have escalated in recent years.1 Despite improvements in surveillance and clinical treatment strategies, the prognosis of HCC remains very poor due to high incidence of recurrence and metastasis.2 Traditional clinicopathological parameters such as tumor morphology, Abbreviations: AFP, alpha-fetoprotein; AUC, area under the curve; BCLC, Barcelona Clinical Liver Cancer; CI, confidence interval; CK, cytokeratin; CSC, cancer stem cell; CTC, circulating tumor cell; DAPI, 4’,6-diamidino-2-phenylindole; EpCAMþ, epithelial cell adhesion molecule–positive; HCC, hepatocellular carcinoma; mRNA, messenger RNA; NOD/SCID, nonobese diabetic/severe combined immunodeficiency; qRT-PCR, quantitative real-time polymerase chain reaction; ROC, receiver operating characteristic; TACE, transcatheter arterial chemoembolization; TTR, time to recurrence. From the 1Department of Liver Surgery, Liver Cancer Institute, Zhongshan Hospital, Fudan University, and Key Laboratory of Carcinogenesis and Cancer Invasion, Ministry of Education, Shanghai 200032, P. R. China; 2Department of Laboratory Medicine, Zhongshan Hospital, Fudan University; 3Institute of Biomedical Sciences, Fudan University, Shanghai 200032, P. R. China Received March 12, 2012; accepted October 27, 2012. Supported by grants from the Major Program of National Natural Science Foundation of China (81030038), the National Key Sci-Tech Project (2012ZX10002011-002, 2013ZX10002011-004, 2012ZX0930100-007, and 2012ZX10002-016), the National Natural Science Foundation of China (81000927, 81071661, 81172277, and 30972949), the Research Fund for the Doctoral Program of Higher Education of China (20100071120064), and the Shanghai New Project for Excellent Youth (XYQ2011020). National Science Foundation for Distinguished Young Scholars of China (81225019); Shanghai Rising-Star Follow-up Program Fundings (10QH1400500). *These authors contributed equally to this work. 1458 HEPATOLOGY, Vol. 57, No. 4, 2013 histopathological features, and tumor staging system offer limited information for predicting postoperative recurrence and fail to monitor the therapeutic response in a real-time manner.3 Therefore, it is imperative to develop novel approaches for discriminating high-risk factors of recurrent patients and continuous surveillance of antitumor treatment response. The spread of circulating tumor cells (CTCs) in the blood plays a major role in the initiation of metastases and tumor recurrence after surgery.3 Recent studies have reported that stem cell markers are frequently overexpressed in CTCs of metastatic breast cancer.4 In addition, clinical observations and animal model studies indicate that although thousands of tumor cells disseminate into the circulation, only a small population with stem cell–like properties survives migration to establish secondary colonies.5,6 Therefore, CTCs with stem cell properties might be potential sources for cancer relapse and distant metastasis, consistent with the cancer stem cell (CSC) hypothesis.7 The US Food and Drug Administration–approved CellSearch system, which enriches CTCs via anti-EpCAM antibody conjugated to ferrofluid magnetic particles, has been reported to enumerate CTCs in some specific types of malignancies.8 However, there has been no report of applying this method to detection of CTCs in HCC patients, and the prognostic and biological relevance of EpCAMþ CTCs in HCC patients remains unclear. In our previous work, we confirmed that EpCAMþ HCC cells derived from cell lines and tumor specimens were highly invasive and tumorigenic, and EpCAM could serve as a biomarker for tumor-initiating cells in HCC.9,10 Thus, detection of CTCs by EpCAM expression may indicate the more aggressive stem cell–like CTCs in HCC. Further identification of biological characteristics of this CTC subpopulation could lead to development of novel targeted drugs and extract more information on the mechanisms of metastasis in this cancer. In this study, we hypothesized that EpCAMþ CTCs embed CSC properties and were one of the potential sources of HCC recurrence and metastasis, and therefore their detection might correlate with an adverse clinical outcome. To test the hypothesis, we used a standardized CellSearch method to prospectively explore the prevalence, dynamic changes, and prognostic significance of SUN, XU, YANG, ET AL. 1459 these cells in HCC patients undergoing curative resection. In addition, expression of CSC-related molecules, apoptotic propensity, and tumorigenic capacity were investigated in EpCAMþ CTCs. Patients and Methods Patients and Specimens. From July 2010 to June 2011, 123 HCC patients undergoing curative resection were recruited into a prospective study. The entrance criteria were: (1) definitive pathological diagnosis of HCC based on World Health Organization criteria; (2) curative resection, defined as complete macroscopic removal of the tumor11; and (3) no prior anticancer treatment. Tumor stage was determined according to the Barcelona Clinic Liver Cancer (BCLC) staging system,12 and tumor differentiation was defined according to the Edmondson grading system.13 In addition, 10 healthy donors and five patients with benign liver disease were enrolled as negative controls. The time points for blood collection were 2 days before resection (baseline), and a median of 31 days (range, 2748 days) after resection. Samples of 7.5 mL were collected and used for CellSearch analysis. A second blood sample (7.5 mL) for confocal microscopic analysis was obtained prior to surgery from the 82 patients who were positive for preoperative EpCAMþ CTCs. Additional samples were taken from selected individuals for use in quantitative real-time polymerase chain reaction (qRT-PCR) assays (30 HCC patients and 20 healthy volunteers, 10 mL blood per patient) and tumorigenic assays (six HCC patients, 30 mL blood per patient). Ethical approval for the use of human subjects was obtained from the Research Ethics Committee of Zhongshan Hospital consistent with ethical guidelines of the 1975 Declaration of Helsinki, and informed consent was obtained from each patient. Follow-up and Tumor Recurrence. Postoperative patient surveillance was performed as described.14 A diagnosis of recurrence was based on computed tomography scans, magnetic resonance imaging, digital subtraction angiography and raised serum alpha-fetoprotein (AFP) level, with or without histological confirmation. Follow-up was terminated on June 30, 2012. Time to recurrence (TTR) was defined as the interval between resection and the diagnosis of any type of recurrence,15 Address reprint requests to: Jia Fan, M.D., Ph.D., Liver Cancer Institute, Zhongshan Hospital, Fudan University, 136 Yi Xue Yuan Road, Shanghai 200032, People s Republic of China. E-mail: [email protected]; fax: (86)-21-64037181; or Jian Zhou, M.D., Ph.D., Liver Cancer Institute, Zhongshan Hospital, Fudan University, 136 Yi Xue Yuan Road, Shanghai 200032, People s Republic of China. E-mail: [email protected]; fax: (86)-21-64037181. C 2013 by the American Association for the Study of Liver Diseases. Copyright V View this article online at wileyonlinelibrary.com. DOI 10.1002/hep.26151 Potential conflict of interest: Nothing to report. Additional Supporting Information may be found in the online version of this article. 1460 SUN, XU, YANG, ET AL. with intrahepatic recurrence and extrahepatic metastasis defined as the end points.16 We defined recurrence within 1 year after surgery as early recurrence.17 CD45 Depletion, Messenger RNA Isolation, Reverse-Transcription, and qRT-PCR. Cells were enriched from blood samples within 8 hours after collection using the RosetteSep Human CD45 Depletion Cocktail (StemCell Technologies, Vancouver, Canada) as described.18 The CD45-depleted fraction was subjected to messenger RNA (mRNA) isolation using the RNeasy Micro Kit (QIAGEN, Valencia, CA). Subsequently, reverse transcription was performed using the Quantitect Reverse Transcription Kit (Qiagen). Analysis by qRT-PCR was done with the Light Cycler 480 system (Roche Diagnostics, Basel, Switzerland). All procedures were performed according to the manufacturer’s instructions. Gene expression levels were calculated according to the following equation: 2DCT [DCT ¼ Ct(target) Ct(bactin)]. PCR conditions were as follows: 10 minutes at 95 C, followed by 45 cycles of 95 C for 10 seconds and 60 C for 60 seconds. Every sample was measured in triplicate. The primers used are listed in Supporting Table 1. Enumeration of CTCs. EpCAMþ CTC analysis was performed using CellSearch (Veridex, Raritan, NJ) as described,19 without knowledge of patient clinical characteristics. Results of CTC enumeration were expressed as the number of cells per 7.5 mL of blood (CTC7.5). Analysis of EpCAM1 CTCs via Confocal Microscopy. Blood samples were processed using the CellSearch Profile kit (Veridex) to isolate and collect EpCAMþ cells,20 and cells in the isolated fraction were prepared by cytospin (Thermo Fisher, Waltham, MA) and subjected to immunofluorescence analysis as described.20 The antibodies used in the study are listed in Supporting Table 2. All samples were analyzed with a Zeiss confocal microscope (Carl Zeiss, Oberkochen, Germany). Isolation of Circulating EpCAM1/CD452 Cells and Tumorigenic Assay. To ensure that enough EpCAMþ CTCs were harvested for tumorigenic assay, we collected 30 mL blood from each of the six patients who had advanced HCC with portal vein thrombosis. Mononuclear cells from whole blood were isolated by density gradient centrifugation using FicollPaque PLUS medium (GE Healthcare,Waukesha, WI) within 1 hour after collection. The isolated cells were then subjected to magnetic-activated cell sorting (Milteny Biotec GmbH, Bergisch Gladbach, Germany), to purify EpCAMþ/CD45 CTCs by CD45 depletion and EpCAM selection. All procedures were performed according to the manufacturer’s instructions. Four-week-old nonobese diabetic/severe combined immunodeficiency (NOD/SCID) mice were purchased HEPATOLOGY, April 2013 from the Shanghai Laboratory Animal Commission of the Chinese Academy of Science, Shanghai, China. Cells to be tested were suspended in 100 lL of Dulbecco’s modified Eagle’s medium and Matrigel (1:1). Approximately 300 EpCAMþCD45 or 1 104 EpCAMCD45 cells were injected subcutaneously into the flank of each NOD/SCID mice. The size and incidence of subcutaneous tumors were recorded every week. These procedures were approved by The Animal Care and Use Committee of Fudan University. Statistical Analysis. The cutoff value used in prognosis was estimated using X-tile 3.6.1 software (Yale University, New Haven, CT).21 The results indicated that in blood, a threshold CTC7.5 value of 2 showed the most significant power to predict patient outcome (Supporting Fig. 1); therefore, it was used in all further analyses. Receiver operating characteristic (ROC) analysis confirmed that this level was the optimal cutoff. Statistical analyses were performed with SPSS version 19.0 for Windows (IBM). Data are presented as the mean 6 SEM. A chi-squared test, Fisher’s exact test, and Student t test were used for comparison between groups where appropriate. The relationship between the TTR and CTC counts was analyzed using Kaplan-Meier survival curves and a log-rank test. Univariate and multivariate analyses were based on the Cox proportional hazard regression model. P < 0.05 was considered statistically significant. ROC curve analysis was used to determine the predictive value of the parameters, and the differences in the area under the curve (AUC) were detected using Stata version 10 (StataCorp, College Station, TX). Results High Expression Levels of EpCAM mRNA in CD45-Depleted Peripheral Blood Mononuclear Cells. The mRNA levels of four putative hepatic CSC biomarkers (EpCAM, CD133, CD90, and ABCG2) were determined via qRT-PCR analysis in CD45depleted peripheral blood mononuclear cells of 30 HCC patients and 20 healthy volunteers. The expression of EpCAM was significantly higher in cells of HCC patients versus healthy controls (P < 0.05), whereas there was no significant difference in the expression of CD133, CD90, or ABCG2 between the groups (P > 0.05) (Fig. 1A). These data suggested that EpCAM might be a reliable biomarker to identify circulating CSCs in HCC. Detection of EpCAM1 CTCs. Because the mRNA level of EpCAM was highly expressed in CD45depleted peripheral blood mononuclear cells of HCC HEPATOLOGY, Vol. 57, No. 4, 2013 SUN, XU, YANG, ET AL. 1461 Fig. 1. Identification and some CSC characteristics of EpCAMþ CTCs. (A) mRNA expression levels of four putative cancer stem cell markers in CD45-depleted blood samples of healthy volunteers (n ¼ 20) and HCC patients (n ¼ 30). (B) Typical images of EpCAMþ CTCs identified with the CellSearch system. CTCs are defined as cells staining positively for CK and DAPI and negatively for CD45. Circulating tumor microemboli (CTM) are defined as CTC clusters. Apoptotic CTCs are defined as CTCs with fragmented, condensed DAPI-stained nuclei morphology. (C) Expression of CSCs and epithelial-mesenchymal transition–related markers in EpCAMþ CTCs. (D) Representative NOD/SCID mice tested for tumorigenicity of subcutaneously injected EpCAMþ/CD45 or EpCAM/CD45 CTCs (upper panels) and hematoxylin and eosin (H&E) staining of subcutaneous nodules (lower panels). Scale bar, 100 lm. patients, we investigated the prevalence of EpCAMþ CTCs in HCC patients using the CellSearch system. CTCs detected with the CellSearch system were defined as nucleated intact cells that were positive for cytokeratins and negative for CD45 (Fig. 1B).8 Apoptotic CTCs, defined as CTCs with fragmented, condensed 4’,6-diamidino-2-phenylindole (DAPI)-stained nuclear,22 were also enumerated and examples were shown in Fig. 1B. The apoptotic cells were excluded from the CTC counts and recorded separately. Preoperatively, EpCAMþ CTCs were detected in 82 of 123 HCC patients at CTC7.5 levels within a range of 1-34, and 51 patients had counts of 2. No CTCs were detected in 41 HCC patients or in any of the 1462 SUN, XU, YANG, ET AL. HEPATOLOGY, April 2013 Table 1. Expression Profile of Stem Cell–Like and EpithelialMesenchymal Transition Markers in Nucleated EpCAM1/ CK1/CD452 CTCs From HCC Patients Positive for EpCAM1 CTCs Markers CD133 ABCG2 CD90 b-Catenin Vimentin/E-cadherin Vimentinþ/E-cadherin Vimentin/E-cadherinþ Vimentinþ/E-cadherinþ Patients with Marker-Positive CTCs 14/17 12/16 0/16 10/17 (82.35) (75.00) (0.00) (58.82) 10/16 (62.5) 3/16 (18.75) 4/16 (25.00) Marker-Positive CTCs 54/65 43/59 0/51 37/69 (83.07) (72.88) (0.00) (53.62) 38/59 (64.41) 6/59 (10.17) 8/59 (13.56) Columns on the right represent the number of patients with at least one CTC that stains positive for a given marker and number of CTCs scoring positive for each marker. Data are presented as no. (%). blood samples derived from healthy volunteers or patients with benign liver disease. Stem Cell–Like Phenotypes Found in EpCAM1 CTCs. Eighty-two blood samples from patients with positive preoperative EpCAMþ CTCs were processed using the CellSearch Profile procedure and divided into five triple-staining panels according to random numbers generated by SPSS, including panel 1 for CD133/cytokeratin (CK)/CD45 (n ¼ 17), panel 2 for ABCG2/CK/CD45 (n ¼ 16), panel 3 for CD90/CK/ CD45 (n ¼ 16), panel 4 for b-catenin/CK/CD45 (n ¼ 17), and panel 5 for vimentin/E-cadherin/CD45 (n ¼ 16) (Fig. 1C, Supporting Fig. 2, and Table 1). CD133þ/CKþ/CD45 cells were identified in 14 of 17 patients, and accounted for 54 of 65 EpCAMþ CTCs from these patients. Twelve of 16 patients had ABCG2þ/CKþ/CD45 cells, and ABCG2 was expressed in 43 of 59 detectable CTCs. None of 16 patients had detectable CD90þ/CKþ/CD45 cells (Supporting Fig. 2). We found evidence of cytoplasmic/nuclear b-catenin accumulation of EpCAMþ CTCs in 10 of 17 patients, and 37 of 69 cells observed showed b-catenin accumulation (cytoplasmic versus nuclear: 37 versus 15). Among 16 patients staining for vimentin/E-cadherin/CD45, three patients had vimentin/E-cadherinþ/CD45 CTCs, 10 had vimentinþ/E-cadherin/CD45 cells, and four coexpressed vimentin and E-cadherin on CD45 cells. Vimentin/E-cadherinþ/CD45, vimentinþ/Ecadherin/CD45, and vimentinþ/E-cadherinþ/ CD45 cells accounted for 6, 38, and 8 EpCAMþ CTCs, respectively, of the total of 59 observed. The details are shown in Table 1. EpCAM1 CTCs in HCC Patients Might Have a Survival Advantage. Apoptotic status of CTCs was investigated in the cohort of 123 HCC patients. CTCs with apoptotic morphology were observed in 19 of 82 patients who had positive preoperative CTCs, and apoptotic cells accounted for 29 of 348 overall EpCAMþ CTCs (nonapoptotic and apoptotic) that were examined. The apoptotic ratio of total EpCAMþ CTCs in HCC (8.3%) in our study is lower than reported for other tumor types (20%-54%).22,23 Table 2. Clinical Characteristics of HCC Patients and Correlation With EpCAM1 CTC Counts Clinical Characteristics Age, years 50 >50 Sex Male Female HBsAg Negative Positive Child-Pugh score A B Liver cirrhosis No Yes ALT, U/L 75 >75 AFP, ng/mL 400 >400 No. of tumors Single Multiple Tumor size, cm 5 >5 Tumor encapsulation Complete None Satellite lesion No Yes Vascular invasion No Yes Edmondson stage I-II II-IV BCLC stage 0þA BþC Recurrence No Yes No. of Patients (N ¼ 123) CTC7.5 <2 CTC7.5 2 64 59 39 33 25 26 115 8 69 3 46 5 12 111 9 63 3 48 122 1 71 1 51 0 29 94 17 55 12 39 102 21 63 9 39 12 70 53 48 24 22 29 112 11 65 7 47 4 80 43 51 21 29 22 77 46 22 50 24 27 106 17 68 4 38 13 78 45 56 16 22 29 83 40 57 15 26 25 101 22 61 11 40 11 72 51 57 15 15 36 P 0.573 0.212* 0.223* 0.398† 0.992 0.109 0.009 0.719* 0.109 0.062 0.002 <0.001 0.001 0.370 <0.001 Abbreviations: ALT, alanine aminotransferase; HBsAg, hepatitis B surface antigen. *Continuous correction. †Fisher’s exact test. HEPATOLOGY, Vol. 57, No. 4, 2013 SUN, XU, YANG, ET AL. 1463 Fig. 2. EpCAMþ CTCs correlate significantly with early recurrence. (A) Distribution of CTCs in early recurrent patients (!), nonrecurrent patients (), healthy volunteers (~), and benign liver disease patients (*) (P ¼ 0.006). (B) Kaplan-Meier analysis for time to recurrence in HCC patients with CTC7.5 <2 or 2 preoperatively. (C) Predictive ability of CTC7.5 2 was compared with other clinical parameters by ROC curves in 123 HCC patients. The AUC with 95% CI for time to recurrence are also shown. *P < 0.05 versus CTC7.5 2. EpCAM1 CTCs Exhibited Tumorigenicity Properties. A total of 10 NOD/SCID mice were used in tumorigenicity transplantation experiments, with EpCAMþ/CD45 cells being tested in six mice, and EpCAM/CD45 in four mice. Three months after injection, 50% of the mice injected with EpCAMþCD45 cells developed subcutaneous nodules, while none developed from EpCAMCD45 cells (Fig. 1D). The weights and sizes of subcutaneous tumor nodules are shown in Supporting Fig. 3. Prevalence of EpCAM1 CTC Counts Before Resective Surgery and Their Prognostic Significance. Patient demographics are listed in Table 2. By the time of analysis, early recurrence had occurred in 51 of 123 patients, with a mean follow-up time of 15.1 6 2.3 months (median, 14.6 months; range, 12.3-23.2 months). Among these 51 patients, 39 had intrahepatic recurrence only, five had lung metastasis only, and seven suffered both intrahepatic recurrence and lung metastasis. 1464 SUN, XU, YANG, ET AL. HEPATOLOGY, April 2013 Table 3. Univariate and Multivariate Cox Proportional Regression Analysis of Factors Associated With Recurrence Univariate Analysis Multivariate Analysis Variables HR (95% CI) P HR (95% CI) P Age, >50 years versus 50 years Sex, male versus female HBsAg, positive versus negative Liver cirrhosis, yes versus no Child-Pugh score, B versus A ALT, >75 U/L versus 75 U/L AFP, >400 ng/mL versus 400 ng/mL No. of tumors, multiple versus single Tumor size, >5 cm versus 5 cm Tumor encapsulation, none versus Complete Satellite lesion, yes versus no Vascular invasion, yes versus no Edmondson stage, III-IV versus I-II BCLC stage, BþC versus 0þA Preoperative CTC7.5, 2 versus <2 0.97 (0.56-1.68) 2.02 (0.80-5.10) 3.38 (0.82-13.89) 0.95 (0.50-1.78) 0.05 (0-8,631.53) 1.22 (0.61-2.43) 1.90 (1.09-3.30) 1.07 (0.43-2.70) 2.61 (1.50-4.53) 2.13 (1.23-3.68) 4.01 (2.15-7.72) 2.53 (1.46-4.40) 1.70 (0.97-2.97) 2.39 (1.61-4.37) 5.37 (2.92-9.85) 0.916 0.135 0.092 0.863 0.625 0.577 0.023 0.881 0.001 0.007 <0.001 0.001 0.063 0.005 <0.001 NA NA NA NA NA NA 1.15 (0.63-2.05) NA 2.36 (1.28-4.32) 1.82 (1.01-3.26) 2.70 (1.34-5.44) 0.89 (0.47-1.71) NA NA 5.20 (2.65-10.21) NA NA NA NA NA NA 0.642 NA 0.006 0.045 0.005 0.733 NA NA <0.001 Clinicopathological variables were adopted for their prognostic significance by univariate analyses. Abbreviations: ALT, alanine aminotransferase; HBsAg, hepatitis B surface antigen; HR, hazard ratio; NA, not applicable. CTC counts were significantly higher in recurrent patients than in nonrecurrent ones (mean, 4.1 versus 1.5, respectively; P ¼ 0.006) (Fig. 2A). Recurrence was observed in 36 of 51 patients with preoperative CTC7.5 of 2, whereas only 15 of 72 patients with values of <2 recurred. Among 12 patients who developed lung metastasis, eight patients had CTC7.5 of 2 prior to resection. In addition, patients with preoperative values of 2 were more likely to have satellite lesions (P ¼ 0.002), vascular invasion (P < 0.001), poor tumor differentiation (P ¼ 0.001), and higher serum AFP level (P ¼ 0.009) (Table 2). Using a CTC7.5 of 2 as the cutoff value in univariate analysis, preoperative CTC7.5 counts showed prognostic significance for TTR (P < 0.001) (Table 3). Patients with counts 2 had significantly shorter TTR (median, 4.9 months versus not reached) and higher recurrence rates (70.6% versus 20.8%) than those with CTC7.5 of <2 (P < 0.001) (Fig. 2B). Levels of AFP, tumor size, tumor encapsulation, satellite lesion, vascular invasion, and BCLC stage were also unfavorable prognostic variables for recurrence (P < 0.05) (Table 3). Because BCLC stage was associated with the three clinical categories of tumor characteristics, liver function and performance status, it was not included in multiple analyses to avoid potential bias. In multivariate analysis, a CTC7.5 of 2 was the strongest independent prognostic factor for TTR (hazard ratio, 5.20; 95% confidence interval [CI], 2.65-10.21; P < 0.001) (Table 3). The AUC for a CTC7.5 of 2 was 0.750, with a sensitivity of 70.60% and specificity of 80.00% (P < 0.001; 95% CI, 0.66-0.84). Compared with other clinical indices, a CTC7.5 of 2 prior to resection was the strongest factor for predicting early recurrence in HCC (AUCs with 95% CI for TTR; P < 0.05 versus CTC 2) (Fig. 2C). The prognostic significance of preoperative CTC7.5 within clinical subgroups was further investigated. In patients with AFP 400 ng/mL, we found that patients with a CTC7.5 of 2 had higher recurrence rates (68.20% versus 8.33%) and shorter TTR (median, 5.0 months versus not reached) than those with <2 (P < 0.001) (Fig. 3A). Patients with preoperative CTC7.5 of 2 showed a relatively higher risk of developing postoperative recurrence than those with <2 in low recurrence risk subgroups, including tumor size 5 cm (62.07% versus 13.73%; P ¼ 0.001), single tumor (68.09% versus 21.54%; P < 0.001), absence of satellite lesions (63.16% versus 20.59%; P < 0.001), absence of vascular invasion (68.18% versus 16.07%; P < 0.001), Edmondson stage I-II (73.07% versus 19.30%; P < 0.001), and BCLC stage 0þA (67.50 % versus 14.75%; P < 0.001) (Figs. 3B-H).17,24 The Dynamic Changes of EpCAM1 CTC Counts After Surgery and Their Prognostic Significance. The postoperative levels were measured in 103 patients at 1 month following resection. Both the CTC-positive rates (66.67% to 28.15%; P < 0.05) and CTC7.5 values (2.60 6 0.43 to 1.00 6 0.36; P < 0.05) dropped dramatically after surgery (Fig. 4A). Based on changes between preoperative and postoperative CTC7.5, 103 patients were divided into four groups: I, persistent levels of 2 CTCs (n ¼ 8) at the two time points; II, preoperatively 2 then postoperatively <2 (n ¼ 31); III, preoperatively <2 then postoperatively 2 (n ¼ 6); and IV, persistent <2 (n ¼ 58). HEPATOLOGY, Vol. 57, No. 4, 2013 SUN, XU, YANG, ET AL. 1465 Fig. 3. Kaplan-Meier analysis of EpCAMþ CTCs in subgroups of HCC patients. The prognostic value of EpCAMþ CTCs was significant in (A) the AFP 400 ng/mL and (B-H) clinical low recurrence risk subgroups, including (B) tumor size 5 cm, (C) single tumor, (D) no satellite lesions, (E) no vascular invasion, (F) Edmondson stage I-II, and (G) BCLC stage 0þA. (H) Recurrent rates of patients with CTC7.5 <2 versus 2 CTCs in the subgroups for tumor size 5 cm, single tumor, no satellite lesion, no vascular invasion, Edmondson stage I-II, BCLC stage 0þA, and AFP 400 ng/mL. The recurrence rates for groups I-IV were 87.50%, 61.3%, 66.7%, and 15.5%, respectively. Patients in group I showed significantly shorter TTR and higher recurrence rates than group IV (median TTR of 2.2 versus not reached; recurrence of 87.5% versus 15.5%; P < 0.001) and a propensity of increased recurrence compared with group II (median TTR, 2.2 months versus not reached; recurrence, 87.50% versus 61.3%; P ¼ 0.073) and while there was no significant difference among recurrence rates of groups I and III (P ¼ 0.241) (Fig. 4B). Compared with group IV, patients in the other three groups had significantly shorter TTR and higher recurrence rates (P < 0.001) (Fig. 4B). Discussion The most effective therapeutic options for HCC offering a favorable prognosis are hepatectomy and liver transplantation. However, even such presumably curative surgery does not guarantee full recovery, and 1466 SUN, XU, YANG, ET AL. HEPATOLOGY, April 2013 Fig. 4. Changes in EpCAMþ CTC load reflect treatment response to HCC resection. (A) Changes in CTC load before versus after surgery. (B) Prognostic significance of CTC load for time to recurrence in patients with persistent CTC7.5 2, conversion of CTC7.5 from 2 to <2, conversion of CTC7.5 from <2 to 2, and persistent CTC7.5 of <2. this failure is due in large part to the high incidence of recurrence (50%-70% at 5 years).2 The most significant reason for the unsatisfactory therapeutic outcome is residual micrometastases formed prior to resection or dissemination of tumor cells during surgical manipulation.25 Unfortunately, routine diagnostic approaches are thus far unable to identify the HCC patient subpopulation at high risk of developing micrometastases preoperatively,17 as well as the tumor cells that escape or invade into peripheral blood during surgery. Recent clinical studies have provided evidence that CTCs may directly participate in the metastasis cascade in various types of malignancies.26 The prognostic significance of CTCs has been widely reported in metastatic breast, colon, and prostate cancers. However, the presence of CTCs in the circulation is a necessary but insufficient condition for the initiation of metastasis, since only a minority of dispersed cells possessing stem cell–like properties is capable of reseeding the tissue of origin or metastasizing to distant organs.3,6 Therefore, identifying the stem cell–like CTC subset with such properties would provide more clinically relevant prognostic information than total CTC counts. In the present study, we found that patients with preoperative CTC7.5 levels of 2 EpCAMþ CTCs suffered significantly earlier recurrence (within 1 year) than patients with lower levels. A preoperative EpCAMþ CTC7.5 2 was significantly associated with aggressive HCC phenotypes. Moreover, EpCAMþ CTCs displayed stem cell–like traits. Based on these data, we inferred that EpCAMþ CTCs with stem cell– like phenotypes might represent a more aggressive subset of CTCs. These cells were more likely to invade the circulatory system, survive, and finally seed in orthotopic or distant sites, leading to local recurrence or distant metastasis. Thus, the preoperative detection of EpCAMþ CTCs might serve as a novel indicator reflecting the micrometastatic status and recurrence risk of HCC patients in a real-time manner, which in turn could provide a therapeutic window and target before the appearance of bona fide recurrence. According to the CSC hypothesis, a small population of cells possessing stem cell–like traits is the driving force of tumor progression and resistance to classical therapies. Their presence in tumor tissues was reported to be associated with a very poor clinical outcome in HCC patients.16,27 Whether CTCs from HCC embed stem cell–like characteristics still requires additional study. Here, we have found that EpCAMþ CTCs preferentially coexpress CSC biomarkers, such as CD133 and ABCG2, or exhibit cytoplasmic and nuclear accumulation of b-catenin, which indicates Wnt pathway activation.28 We also observed that EpCAMþ CTCs in most patients displayed a mesenchymal phenotype with vimentinþ/E-cadherin (Fig. 1B), which is also an important property of CSCs.29 The apoptotic ratio of total EpCAMþ CTCs in HCC (8.3%) in our study was lower than reported in other tumor types (20%-54%).22,23 In addition, we also observed that EpCAMþ/CD45 CTCs had high HEPATOLOGY, Vol. 57, No. 4, 2013 tumorigenic potential, while EpCAM/CD45 cells did not. All of these data indicated that EpCAMþ CTCs in HCC embedded properties of cancer stem– like cells, which might be the ‘‘seeds’’ of tumor metastasis and recurrence.7 In clinical practice, it is challenging to predict tumor relapse in low recurrence risk HCC subgroups.17,24 The present study is the first to show that preoperative EpCAMþ CTC levels retain their prognostic value in those subgroups at risk for which conventional clinicopathological variables offer limited information predicting tumor recurrence. So far, AFP level is the most extensively used diagnostic biomarker and tumor recurrence indicator of HCC in AFP-positive patients.30 Clinical data demonstrated that low serum AFP concentration (e.g., 400 ng/mL) was associated with better clinical outcome. Nevertheless, it is difficult to monitor recurrence in the 30%-40% of HCC patients with low AFP levels.17,31 Here, we have shown that determination of preoperative EpCAMþ CTC level is a promising and feasible tool for recurrence prediction in patients with low AFP concentration. Large cohort studies should be undertaken to further validate the prognostic significance in this specific HCC patient subpopulation. The clinical use of monitoring CTC changes with treatment has been reported in various types of cancers.32,33 However, the influence of surgical resection of the primary tumor on CTC status in HCC remains to be elucidated. In the present study, we report for the first time that a significant decrease of CTC load was observed soon after resection, which may well be attributed to surgical resection of the primary tumor. Patients whose CTC7.5 failed to drop to <2 postoperatively showed a propensity of increased recurrence, and this suggested that CTC detection might be a surrogate indicator for surveillance of the response to the HCC curative resection. Furthermore, in BCLC 0þA patients, those who experienced a drop of CTC7.5 to <2 postoperatively showed lower recurrence risk than those with persistent levels of 2 CTCs (P ¼ 0.044; data not shown). We propose that treatment response surveillance by determination of CTC load may provide a powerful test enabling accurate and early decision making to tailor the most effective therapy according to characteristics of individual tumors. Our previous study indicated that postoperative adjuvant transcatheter arterial chemoembolization (TACE) could improve the survival of patients with risk factors for residual tumor.34 In our study, patients with a high risk of recurrence, evidenced by clinical features such as vascular invasion and microsatellite SUN, XU, YANG, ET AL. 1467 lesions, were given one to three courses of prophylactic TACE (doxorubicin, cisplatin, 5-fluorouracil, and iodized oil) 1 month after surgery.35 We retrospectively collected the data of HCC patients with 2 CTCs who performed the prophylactic TACE and compared the antirecurrence results with those who did not perform TACE, and found that prophylactic TACE was beneficial in preventing recurrence in patients with 2 CTCs (P ¼ 0.006) (Supporting Fig. 4). However, randomized controlled trials are needed for further validation. The limitations of this study are its relatively small cohort size, short follow-up time, and data from a single study center. A prospective, multicenter, randomized clinical trial should be designed to further validate the prognostic significance of CTCs in HCC. To our knowledge, this is the first report to identify the stem cell–like characteristics of EpCAMþ CTCs and their prognostic significance using the standardized CellSearch system in HCC patients. A preoperative EpCAMþ CTC7.5 level of 2 is an independent prognostic indicator for recurrence in HCC patients undergoing curative resection. Monitoring dynamic changes of perioperative CTCs may be a promising predictor of the response of the therapeutic regimen. Eradicating these cells might open a therapeutic avenue toward preventing HCC recurrence. References 1. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010;60:277-300. 2. Cha C, Fong Y, Jarnagin WR, Blumgart LH, DeMatteo RP. Predictors and patterns of recurrence after resection of hepatocellular carcinoma. J Am Coll Surg 2003;197:753-758. 3. Pantel K, Brakenhoff RH, Brandt B. Detection, clinical relevance and specific biological properties of disseminating tumour cells. Nat Rev Cancer 2008;8:329-340. 4. Aktas B, Tewes M, Fehm T, Hauch S, Kimmig R, Kasimir-Bauer S. Stem cell and epithelial-mesenchymal transition markers are frequently overexpressed in circulating tumor cells of metastatic breast cancer patients. Breast Cancer Res 2009;11:R46. 5. Raimondi C, Gradilone A, Naso G, Vincenzi B, Petracca A, Nicolazzo C, et al. Epithelial-mesenchymal transition and stemness features in circulating tumor cells from breast cancer patients. Breast Cancer Res Treat 2011;130:449-455. 6. Kim MY, Oskarsson T, Acharyya S, Nguyen DX, Zhang XH, Norton L, et al. Tumor self-seeding by circulating cancer cells. Cell 2009;139: 1315-1326. 7. Clevers H. The cancer stem cell: premises, promises and challenges. Nat Med 2011;17:313-319. 8. Allard WJ, Matera J, Miller MC, Repollet M, Connelly MC, Rao C, et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin Cancer Res 2004;10:6897-6904. 9. Yamashita T, Ji J, Budhu A, Forgues M, Yang W, Wang HY, et al. EpCAM-positive hepatocellular carcinoma cells are tumor-initiating 1468 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. SUN, XU, YANG, ET AL. cells with stem/progenitor cell features. Gastroenterology 2009;136: 1012-1024. Yamashita T, Forgues M, Wang W, Kim JW, Ye Q, Jia H, et al. EpCAM and alpha-fetoprotein expression defines novel prognostic subtypes of hepatocellular carcinoma. Cancer Res 2008;68:1451-1461. Poon RT, Ng IO, Lau C, Yu WC, Yang ZF, Fan ST, et al. Tumor microvessel density as a predictor of recurrence after resection of hepatocellular carcinoma: a prospective study. J Clin Oncol 2002;20: 1775-1785. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. HEPATOLOGY 2011;53:1020-1022. Wittekind C. Pitfalls in the classification of liver tumors [in German]. Pathologe 2006;27:289-293. Yang XY, Xu Y, Shi GM, Fan J, Zhou J, Ji Y, et al. Cytokeratin 10 and cytokeratin 19: predictive markers for poor prognosis in hepatocellular carcinoma patients after curative resection. Clin Cancer Res 2008;14: 3850-3859. Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst 2008;100:698-711. Yang XR, Xu Y, Yu B, Zhou J, Qiu SJ, Shi GM, et al. High expression levels of putative hepatic stem/progenitor cell biomarkers related to tumour angiogenesis and poor prognosis of hepatocellular carcinoma. Gut 2010;59:953-962. Shah SA, Greig PD, Gallinger S, Cattral MS, Dixon E, Kim RD, et al. Factors associated with early recurrence after resection for hepatocellular carcinoma and outcomes. J Am Coll Surg 2006;202:275-283. Reinholz MM, Kitzmann KA, Tenner K, Hillman D, Dueck AC, Hobday TJ, et al. Cytokeratin-19 and mammaglobin gene expression in circulating tumor cells from metastatic breast cancer patients enrolled in North Central Cancer Treatment Group trials, N0234/336/436/437. Clin Cancer Res 2011;17:7183-7193. Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 2004;351:781-791. Kallergi G, Markomanolaki H, Giannoukaraki V, Papadaki MA, Strati A, Lianidou ES, et al. Hypoxia-inducible factor-1alpha and vascular endothelial growth factor expression in circulating tumor cells of breast cancer patients. Breast Cancer Res 2009;11:R84. Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res 2004;10:7252-7259. Mehes G, Witt A, Kubista E, Ambros PF. Circulating breast cancer cells are frequently apoptotic. Am J Pathol 2001;159:17-20. HEPATOLOGY, April 2013 23. Larson CJ, Moreno JG, Pienta KJ, Gross S, Repollet M, O’Hara SM, et al. Apoptosis of circulating tumor cells in prostate cancer patients. Cytometry A 2004;62:46-53. 24. Tung-Ping Poon R, Fan ST, Wong J. Risk factors, prevention, and management of postoperative recurrence after resection of hepatocellular carcinoma. Ann Surg 2000;232:10-24. 25. Shah SA, Cleary SP, Wei AC, Yang I, Taylor BR, Hemming AW, et al. Recurrence after liver resection for hepatocellular carcinoma: risk factors, treatment, and outcomes. Surgery 2007;141:330-339. 26. Sun YF, Yang XR, Zhou J, Qiu SJ, Fan J, Xu Y. Circulating tumor cells: advances in detection methods, biological issues, and clinical relevance. J Cancer Res Clin Oncol 2011;137:1151-1173. 27. Kim H, Choi GH, Na DC, Ahn EY, Kim GI, Lee JE, et al. Human hepatocellular carcinomas with ‘‘Stemness’’-related marker expression: keratin 19 expression and a poor prognosis. HEPATOLOGY 2011;54: 1707-1717. 28. Takahashi-Yanaga F, Kahn M. Targeting Wnt signaling: can we safely eradicate cancer stem cells? Clin Cancer Res 2010;16:3153-3162. 29. Polyak K, Weinberg RA. Transitions between epithelial and mesenchymal states: acquisition of malignant and stem cell traits. Nat Rev Cancer 2009;9:265-273. 30. Chan SL, Mo FK, Johnson PJ, Hui EP, Ma BB, Ho WM, et al. New utility of an old marker: serial-fetoprotein measurement in predicting radiologic response and survival of patients with hepatocellular carcinoma undergoing systemic chemotherapy. J Clin Oncol 2009;27: 446-452. 31. Wang CC, Iyer SG, Low JK, Lin CY, Wang SH, Lu SN, et al. Perioperative factors affecting long-term outcomes of 473 consecutive patients undergoing hepatectomy for hepatocellular carcinoma. Ann Surg Oncol 2009;16:1832-1842. 32. Cohen SJ, Punt CJ, Iannotti N, Saidman BH, Sabbath KD, Gabrail NY, et al. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J Clin Oncol 2008;26:3213-3221. 33. Liu MC, Shields PG, Warren RD, Cohen P, Wilkinson M, Ottaviano YL, et al. Circulating tumor cells: a useful predictor of treatment efficacy in metastatic breast cancer. J Clin Oncol 2009;27:5153-5159. 34. Ren ZG, Lin ZY, Xia JL, Ye SL, Ma ZC, Ye QH, et al. Postoperative adjuvant arterial chemoembolization improves survival of hepatocellular carcinoma patients with risk factors for residual tumor: a retrospective control study. World J Gastroenterol 2004;10:2791-2794. 35. Yang XR, Xu Y, Yu B, Zhou J, Li JC, Qiu SJ, et al. CD24 is a novel predictor for poor prognosis of hepatocellular carcinoma after surgery. Clin Cancer Res 2009;15:5518-5527.