Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
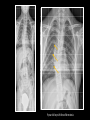
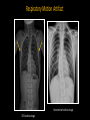
Scoliosis: What you need to know Nancy A. Chauvin, MD Assistant Professor of Radiology Director of Musculoskeletal Imaging The Children’s Hospital of Philadelphia University of Pennsylvania, Perelman School of Medicine IPR, 2016 Learning Objectives • Review pathophysiology and classification of scoliosis • Discuss an imaging Algorithm and approach to interpretation • Explore indications for MRI • Describe treatment options • Evaluate the use Digital Slot Scanning Scoliosis 15° Lateral curvature of the spine > 10 ° as measured by the Cobb method on a standing radiograph Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251 11° 15 year old girl Spinal Asymmetry • Curves less than 10 ° Clinical follow - up Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251 Curve Development Hueter-Volkman law – growth is retarded by mechanical compression on the growth plate and accelerated by growth plate tension Curves progress during periods of rapid spinal growth Kim et al. Radiographics 2010; 30: 1823-1812 Primary (Idiopathic) vs Secondary Scoliosis • Primary (Idiopathic) • Classified according to age 80% • Secondary • Congenital • Neuromuscular • Developmental/Syndromic • Tumor associated Kim et al. Radiographics 2010; 30: 1823-1812 10% 10% Congenital Scoliosis • 2nd most common type • Maldevelopment of vertebral elements (bone and neural tissue) • May not become apparent until later in childhood • Most common • Hemivertebra ~ 40% Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251 Anterior Congenital Scoliosis • Curve progression is related to the vertebral abnormality Posterior • Poorest prognosis – unilateral unsegmented bars with contralateral hemivertebrae Birth Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251 9 month-old www.rad.washington.edu Neuromuscular Scoliosis • Neurologic disorders • e.g. CP, spinocerebellar degeneration • Myopathic causes • e.g. Muscular dystrophies Lack of muscular support of the spinal column – gravity & posturing cause deformity • Characteristic long C-shaped curve • Less commonly S-shaped patterns • Often with severe kyphosis or lordosis El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251 9 year-old girl with Rett syndrome Idiopathic Scoliosis Largest subset 0.5-3/100 children Diagnosis of exclusion -Based on age Type Infantile Age (years) 0-3 Incidence (%) 0.5 Juvenile 4-10 10.5 Adolescent 11-17 89 Age at onset has prognostic significance Early Onset < age 8 years Late Onset > 8 years Riseborough EJ et al. J Bone Joint Sug Am 1973; 55: 974-982 Infantile Idiopathic Scoliosis Male, left sided thoracic curve 75% of curves resolve spontaneously 25% progress rapidly Spine growth Most rapid during the 1st 5 years (2.2 cm/year) Slows 5 – 10 years Peaks again at puberty (1.8 cm/year) El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 17 month-old boy Juvenile Idiopathic Scoliosis Higher rate of cardiopulmonary complications in children who develop large curves before the age of 5 32 ° Alveoli development upto age 7 - 8 years Typically slow progression until age 10, period of accelerated growth El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 Kim et al. Radiographics 2010; 30: 1823-1812 10 year-old girl Adolescent Idiopathic Scoliosis • Risk of progression? • Skeletal maturity • Gender (girls more likely to progress & require treatment • Curve magnitude (increases with skeletal growth) Progresses during growth and ceases when skeletal maturity is reached (provided the curve is not severe) Curves greater than 20 ° in skeletally immature children are at greatest risk for progression El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 Kim et al. Radiographics 2010; 30: 1823-1812 12 year-old girl Terminology Apex Vertebra or disk with the greatest rotation or farthest deveiation from the center of the vertebral column 15 year-old girl Kim et al. Radiographics 2010; 30: 1823-1812 Terminology End Vertebrae Maximal tilt toward the apex of the curve Used to measure the Cobb angle Kim et al. Radiographics 2010; 30: 1823-1812 Terminology Neutral Vertebrae No evidence of rotation Pedicles in normal, symmetric position Kim et al. Radiographics 2010; 30: 1823-1812 Terminology Stable Vertebrae Farthest cephalad that are bisected or nearly bisected by the central sacral vertical line (CSVL) CSVL – Roughly vertical line that is drawn perpindicular to an imaginary tangential line drawn across the top of the iliac crests (bisects the sacrum) Kim et al. Radiographics 2010; 30: 1823-1812 Cobb Angle Angle formed by the intersection of 2 lines, one parallel to the endplate of the superior end vertebra & other parallel to the endplate of the inferior end vertebra Kim et al. Radiographics 2010; 30: 1823-1812 Goal is to create the largest angle possible Cobb Angle Superior endplate of the most angulated upper body endplate 41 ° Inferior endplate of the most angulated lower body endplate Major & Minor Curves Major curve – “primary curve” largest abnormal curves in the scoliotic spine & first to develop Minor curve – “secondary curve” develops afterward, to compensate for perturvation of balance Kim et al. Radiographics 2010; 30: 1823-1812 14 year-old girl Structural vs Non-Structural Curves Structural Curve Not correctable with ipsilateral bending 70 ° 50 ° Cobb angle > 25 ° on ipsilateral side-bending radiographs Rightward bending Kim et al. Radiographics 2010; 30: 1823-1812 Lenke LG et al. J Bone Joint Surg Am 2001; 83-A: 1169-1191 AP standing 12 year-old girl Structural vs Non-Structural Curves Non-structural correctable with bending Usually does not progress unless ligament shortening results from growth retardation on the concave side of the curvature Becomes important when selecting the appropriate level for fusion Kim et al. Radiographics 2010; 30: 1823-1812 29 ° Levocurvature is fully corrected with rightward bending Cobb Angle Pitfalls www.clker.com • Diurnal variation of 5 degrees – increasing in the afternoon • Vertebral rotation – may underestimate angle on frontal radiographs • Prone positioning – decreased / anesthesia, postoperative rebound effect • Radiographic acquisitions/measurement error – 2 to 7 ° • Same endpoints should be used each time • Intraobserver variation – 5 to 10 ° Kim et al. Radiographics 2010; 30: 1823-1812 Vertebral Alignment & Balance Plumb line – vertical line drawn downward from the center of C7 parallel to the lateral edges of the radiograph Coronal balance Distance between the CSVL and plumb line • Plumb line to the right - Positive • Plumb line to the left – Negative > 2 cm, is abnormal Kim et al. Radiographics 2010; 30: 1823-1812 Vertebral Alignment & Balance Plumb line – vertical line drawn downward from the center of C7 parallel to the lateral edges of the radiograph Sagittal balance Distance between the posterosuperior aspect of S1 and the plumb line • Plumb line anterior – Positive • Plumb line posterior - Negative > 2 cm, is abnormal Kim et al. Radiographics 2010; 30: 1823-1812 Imaging Goals • Detect & characterize type of curve & severity • Identify vertebral anomalies • Track curve progression • Monitor treatment related changes www.nhs.uk Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251 Radiography • PA radiograph of the entire spine • Cervicothoracic junction – pelvis • Standing if possible (seated or supine) Feet placed shoulder width apart, looking straight ahead Elbows bent & knuckles in the supraclavicular fossae Khanna G. Pediatr Radiol 2009; 39 (Suppl 2): S247-251. O’Brien et al. Medtronic Sofamor Denek Arms places at 30 – 45 ° Radiography PA radiograph should include iliac crests & triradiate cartilage 4 year-old boy with scoliosis Skeletal Maturity – Risser Stage Patients with significant growth potential possess a greater potential for curve progression 1936; used despite a lack of consensus of reliability Kim et al. Radiographics 2010; 30: 1823-1812 Reem et al. near perfect agreement of Risser stage rating intra-observer raliability (n=100) & substantial inter-observer agreement Other markers: Rib epiphyses, proximal humeri, closure of triradiate cartilage Reem et al. Skeletal Radiol (2009) 38: 371-375 Risser Stage Risser stage 0 -1: Risk of curve progression is up to 60-70% Risser stage 3: Risk of curve progression is 10% 12 year-old girl Triradiate cartilage usually closes before the iliac crest apophyses appear 4 year-old boy Radiography Lateral radiograph not required at screening - used to assess sagittal balance Normal Thoracic Kyphosis 20 – 50 ° between T1 – T12 Stitch/ Motion Artifacts Digital methods Separate imaging of the thoracic and lumbar spine are acquired Can result in false diagnosis if the source images are not evaluated Supakul et al. 16% of studies had stitching errors that could result in false diagnosis (n = 86) Patient moved between exposures Supakul et al. Pediatr Radiol 2012; 42: 584-598 Stitch/ Motion Artifacts Digital methods Separate imaging of the thoracic and lumbar spine are acquired Can result in false diagnosis if the source images are not evaluated Supakul et al. 16% of studies had stitching errors that could result in false diagnosis (n = 86) Patient moved between exposures Supakul et al. Pediatr Radiol 2012; 42: 584-598 Stitch Artifact Stitched incorrectly, simulating a vertebra plana MRI – Indications for Presumed Idiopathic Scoliosis Age < 10 years Onset between 4 – 12 years, 26 % had abnormal MRIs* Chairi I with syrinx most common Increase Cobb angle by more than 1° / month * Evans et al. J Bone Joint Surg Am 1996; 78: 314-317. Abnormal neurologic examination Foot deformity Rapid progression Back pain, neck pain, head Not ‘generalized’ back pain 560/2442 idiopathic scoliosis, 9% had underlying pathologic condition** **Ramirez et al. J Bone J Surg Am 1997; 79(3): 364-368. Kim et al. Radiographics 2010; 30: 1823-1812 MRI – Indications for Presumed Idiopathic Scoliosis Curve type commonly associated with neuropathy (left thoracic, double thoracic, triple major, short segment, long right thoracic curve, severe curvature after skeletal maturity) Wide spinal canal, thin pedicle, wide neural foramina, features of lesion Kim et al. Radiographics 2010; 30: 1823-1812 25 ° 18 ° Chiari I and syrinx 8 year-old boy with early onset idiopathic scoliosis Congenital Scoliosis Osteoid Osteoma Asymmetric location of the lesion within the neural arch is the most significant factor that leads to scoliosis For scoliosis to develop, muscle spasm must be unilateral Davies et al. Skeletal Radiol 2009; 38: 207-223 Scoliosis with abnormal sagittal balance on exam 7 year-old boy Osteoblastoma 40% of all osteoblastomas are located within the spine 2/3 cause cortical destruction Davies et al. Skeletal Radiol 2009; 38: 207-223. Osteoblastoma 40% of all osteoblastomas are located within the spine 2/3 cause cortical destruction Davies et al. Skeletal Radiol 2009; 38: 207-223. Aneurysmal Bone Cyst Posterior elements are always involved with frequent extension to the vertebral body or rib(s) 9 year old girl Scoliosis associated with ABCs is from unilateral vertebral collapse Davies et al. Skeletal Radiol 2009; 38: 207-223 Langerhans Cell Histiocytosis 12 year-old girl with scoliosis and back pain Davies et al. Skeletal Radiol 2009; 38: 207-223 Most common cause of vertebra plana in children Neurofibromatosis 8 year-old boy 9 year-old boy with Neurofibromatosis Chronic Non-bacterial Osteomyelitis 14 year-old boy with scoliosis and intermittent back pain Treatment – Idiopathic Scoliosis Surgeon preference Curve severity Likelihood of curve progression over time Patient’s perception of deformity & symptoms Observation Adolescent Idiopathic Scoliosis Skeletally immature - Cobb angle < 20 - 25 ° (Risser 0-1) Skeletally mature - Cobb angle < 30 ° (Risser 3) Follow-up at 4 to 12 month intervals El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 Kim et al. Radiographics 2010; 30: 1823-1812 Bracing Adolescent Idiopathic Scoliosis Goal – to avoid surgery Cobb angle of 20 – 45 degrees For curves 20 – 30 degrees, bracing commenced only when progression of 5 degrees or more between 2 consecutive visits Skeletally immature (Risser grade 2 or lower) initial presentation with curve of 30 – 45 ° ~ 75% success rate reducing curve progression Artlet et al. Neurosurg Clin Am 2007; 18: 255-259 Kim et al. Radiographics 2010; 30: 1823-1812 Braces Thoracolumbosacral orthosis (TLSO) www.hangerclinic.com Boston Brace www.sunshinepando.com Charleston Brace www.sunshinepando.com Providence Brace Cosmetic deformity is unlikely to improve Surgery Adolescent Idiopathic Scoliosis Goal – to prevent curve progression by achieving solid bone fusion of involved segments Avoid any neurologic complication Curve correction Trunk balance restoration Sagittal contour preservation Leaving as many mobile segments in the lumbosacral spine as possible Curves greater than 45 ° who are Risser < 2 Curves greater than 50 ° who are Risser > 3 Artlet et al. Neurosurg Clin Am 2007; 18: 255-259 Kim et al. Radiographics 2010; 30: 1823-1812 Each lumbar vertebra provides 15° of flexion & extension – preserving distal motion is critical to maintaining function Treatment – Early Onset Goal – Stop progression of spine deformity & allow for continued growth of the spine, thoracic cavity and lungs Observation Non-surgical treatment with bracing, serial casting Growth-friendly surgery El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 Surgery - Early Onset Goal – Based on the underlying cause Restore seating balance Ease wheelchair use Control pain Support trunk to reinforce respiratory function Growth friendly options to avoid pulmonary insufficiency syndrome/restrictive lung disease El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 Kim et al. Radiographics 2010; 30: 1823-1812 Surgery - Early Onset Complication rates are high! 4 year-old girl Spinal growing rods Spine-based distraction El-Hawary et al. Pediatr Clin N Am 2014; 61: 1223-1241 1 year-old girl Rib based distraction VEPTR Surgery - Early Onset Magnetic Controlled Growing Rods (MCGRs) Non-invasive lengthening via magnet system External remote controller in outpatient setting without need for anesthesia or sedation www.ellipse-tech.com www.eandt.theiet.org Teoh KH et al. The Spine Journal, Accepted 12/28/2015 Biplanar Digital Slot-Scanning Acquisition of concurrent orthogonal radiograph images Narrow radiograph fan beam (no grid needed) Patient stands in the center of the scanner PA and lateral images taken at the same time, so no change in patient position Exposure is ~ 15 seconds – remain still with single breath hold Hull et al. AJR 2015; 205: W124-132 Blumer et al. Pediatr Radiol 2014; 44: 871 – 882 EOS Imaging Operator Manual Biplanar Digital Slot-Scanning Advantages Lower radiation dose (50-60% dose reduction in ED*) Better total spine visualization (obese patients) No geometric magnification Improved work-flow (one expsure without need for stitching) Calculation applications – considering pelvic rotation for Cobb angle calculations Ability to create 3D images (standing position) *Hull et al. AJR 2015; 205: W124-132 Blumer et al. Pediatr Radiol 2014; 44: 871 – 882 10 year-old girl with 32 ° levocurvature Biplanar Digital Slot-Scanning Disadvantages Extensive post-processing (90-120 minutes) Artifacts due to relatively long acquisition times (15 sec) (motion artifacts, edge enhancement, off-center artifact) Cost (Machine with set-up training: $400,000-600,000*) *Hull et al. AJR 2015; 205: W124-132 Blumer et al. Pediatr Radiol 2014; 44: 871 – 882 Cardiac Pulsation Artifact EOS scoliosis image Conventional scoliosis image Incorrect Centering Artifact EOS scoliosis image Conventional scoliosis image Respiratory Motion Artifact Conventional scoliosis image EOS scoliosis image Pseudopneumopericardium Artifact EOS scoliosis image Motion Wavy Fusion Rod Artifact EOS scoliosis image Conventional scoliosis image Motion Wavy Fusion Rod Artifact EOS scoliosis image Conventional scoliosis image Take Home Points • Scoliosis is a common problem in pediatric patients • Cobb angles, vertebral alignment & balance, congenital osseous abnormalities and skeletal maturity should be described • The underlying cause of scoliosis has tremendous impact on prognosis and treatment options • Radiologists should be aware of the indications for advanced imaging • EOS is a low dose technique with very good quality; radiologists should be aware of common artifacts