Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
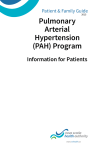
Is Methamphetamine Use Associated With Idiopathic Pulmonary Arterial Hypertension? Kelly M. Chin, Richard N. Channick and Lewis J. Rubin Chest 2006;130;1657-1663 DOI 10.1378/chest.130.6.1657 The online version of this article, along with updated information and services can be found online on the World Wide Web at: http://chestjournal.org/cgi/content/abstract/130/6/1657 CHEST is the official journal of the American College of Chest Physicians. It has been published monthly since 1935. Copyright 2007 by the American College of Chest Physicians, 3300 Dundee Road, Northbrook IL 60062. All rights reserved. No part of this article or PDF may be reproduced or distributed without the prior written permission of the copyright holder (http://www.chestjournal.org/misc/reprints.shtml). ISSN: 0012-3692. Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians CHEST Original Research PULMONARY HYPERTENSION Is Methamphetamine Use Associated With Idiopathic Pulmonary Arterial Hypertension? Kelly M. Chin, MD; Richard N. Channick, MD, FCCP; and Lewis J. Rubin, MD, FCCP Background: Amphetamine, methamphetamine, and cocaine are suspected of being pulmonary hypertension risk factors based on a small number of case reports along with pharmacologic similarities to fenfluramine, a diet drug associated with pulmonary arterial hypertension (PAH). We sought to determine whether rates of stimulant use are increased in patients believed to have idiopathic PAH compared with patients with PAH and known risk factors and patients with chronic thromboembolic pulmonary hypertension (CTEPH). Methods: In this retrospective study, rates of stimulant use were determined for 340 patients with idiopathic PAH, PAH and known risk factors, or CTEPH seen between November 2002 and April 2004. “Stimulant” use was defined as any reported use of amphetamine, methamphetamine, or cocaine. Odds of stimulant use were calculated using a polychotomous logistic regression model. Results: A history of stimulant use was found in 28.9% of patients with a diagnosis of idiopathic PAH, compared with 3.8% of patients with PAH and a known risk factor, and 4.3% of patients with CTEPH. After adjustment for differences in age, patients with idiopathic PAH were 10.14 times (95% confidence interval, 3.39 to 30.3; p < 0.0001) more likely to have used stimulants than patients with PAH and known risk factors, and 7.63 times (95% confidence interval, 2.99 to 19.5; p < 0.0001) more likely to have used stimulants than patients with CTEPH. Conclusions: Patients with idiopathic PAH are significantly more likely to have used stimulants than patients with other forms of pulmonary hypertension. (CHEST 2006; 130:1657–1663) Key words: illicit drugs; methamphetamine; pulmonary hypertension; risk factors Abbreviations: CTEPH ⫽ chronic thromboembolic pulmonary hypertension; PAH ⫽ pulmonary arterial hypertension arterial hypertension (PAH) is a lifeP ulmonary threatening and potentially fatal disorder. While some risk factors for PAH have been identified, many cases remain idiopathic. Amphetamines, cocaine, and other stimulants have been considered *From the Department of Internal Medicine (Dr. Chin), Division of Pulmonary and Critical Care Medicine, St. Paul University Hospital, Dallas, TX; and Department of Internal Medicine (Drs. Channick and Rubin), Division of Pulmonary and Critical Care Medicine, University of California, San Diego, San Diego, CA. The authors have no conflicts of interest to disclose. Manuscript received March 28, 2006; revision accepted May 27, 2006. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal. org/misc/reprints.shtml). Correspondence to: Richard Channick, MD, 9330 Campus Point Dr, MC 7381, La Jolla, CA 92037; e-mail: [email protected] DOI: 10.1378/chest.130.6.1657 www.chestjournal.org “possible” or “very likely” risk factors,1 but evidence supporting this conclusion is limited. There are a small number of case reports implicating cocaine2,3 and methamphetamine4 in the development of pulmonary hypertension, but stimulant use as a PAH risk factor has not been investigated in detail. Over the last decade, the use of stimulants for the treatment of attention deficit disorder has increased approximately threefold.5 Illicit stimulant use has increased as well, with an estimated 5.2% of the population reporting “ever” use of methamphetamine, and 0.6% reporting use in the last year.6 Frequency of methamphetamine and amphetamine use varies by geographic location. Among persons aged ⱖ 12 years, rates of use in the last year in western states (including California) were highest, ranging from 0.98 to 2.21%, while rates in the CHEST / 130 / 6 / DECEMBER, 2006 Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians 1657 northeast were lowest, with most states having rates of use from 0.04 to 0.32%.7 In order to determine whether rates of stimulant use were increased in idiopathic PAH compared with other forms of pulmonary hypertension, we For editorial comment see page 1633 performed a retrospective study evaluating amphetamine, methamphetamine, and cocaine use in patients with pulmonary hypertension seen at a large pulmonary hypertension referral center. A portion of these results were previously published in abstract form.8 Materials and Methods This was a retrospective study conducted at the University of California at San Diego, Thornton Hospital, La Jolla, CA. The study included all patients ⬎ 18 years old with PAH or chronic thromboembolic pulmonary hypertension (CTEPH) seen over an 18-month period (November 2002 to April 2004) in the pulmonary hypertension clinics. Information on demographics, hemodynamics, pulmonary hypertension etiology, race, and prior stimulant drug use was abstracted from medical records. Any use of amphetamine, methamphetamine, or cocaine was considered a positive history of “stimulant” use, as patients were routinely asked about the use of these drugs during the initial history and physical examination. Use of other amphetamine-like drugs was not included, as reliable information was not available for many patients. Patients were categorized by their treating pulmonary hypertension specialist based on the 2003 revised clinical classification,1 and based on this diagnosis they were placed into one of three groups: idiopathic PAH, PAH with known risk factors, and CTEPH. Patients with other forms of pulmonary hypertension such as pulmonary hypertension related to lung disease or left-heart disease were excluded from the study (Table 1). All patients were required to have undergone cardiac catheterization Table 1—Patients Excluded From Analysis Variables Patients, No. Excluded causes of pulmonary hypertension Lung disease Left-heart disease HIV with PAH HIV with CTEPH Portal hypertension with PAH Nonthromboembolic pulmonary artery obstruction* Acute/recent pulmonary embolism No pulmonary hypertension found Normal pressures by catheterization PAH unlikely and catheterization not done Incomplete workup Age ⬍ 18 yr Total 42 42 9 1 5 6 4 39 11 16 8 183 *Included fibrosing mediastinitis, intravascular leiomyomatosis, and pulmonary artery sarcoma. for the initial diagnosis, except those with either a ventricular septal defect or patent ductus arteriosus. For these patients, echocardiographic evidence of the congenital heart abnormality plus pulmonary hypertension was accepted. Patients with either familial PAH or PAH and one of the “associated” conditions listed in the 2003 revised clinical classification1 of pulmonary hypertension were considered to have PAH with known risk factors. This group included familial PAH, PAH associated with collagen vascular disease, PAH associated with congenital systemic-to-pulmonic shunts, and PAH associated with the use of fenfluramine or dexfenfluramine. HIV- and portal hypertension-associated PAH patients were excluded because illicit drug use is a risk factor for HIV and liver disease. Patients with PAH and none of the above risk factors were categorized as having idiopathic PAH. Finally, patients with angiographically proven thromboembolic disease were categorized as having CTEPH. This study received approval by the University of California, San Diego Institutional Review Board, including approval for a waiver of informed consent. This waiver required that there be no disclosure of protected health information and that patient information be “de-identified” at the earliest possible date. Statistical Analysis Statistical analysis was performed using a logistic regression model that included all three groups (polychotomous logistic regression). Age, gender, and race were included in the model as potential confounders due to associations between these variables and type of pulmonary hypertension and the possibility that they may also be associated with stimulant drug use.6 Interaction between stimulant drug use and age, gender, and race was tested using the log likelihood method. After testing for interaction, these potential confounders were removed from the model through backward elimination if the association (odds ratio) between stimulant use and type of pulmonary hypertension changed by ⬍ 10%. Statistical software (NCSS 2004; NCSS; Kaysville, UT) was used for the analysis including tests for collinearity; p ⬍ 0.05 was considered significant. Results Six hundred fourteen patients with a diagnosis of possible or definite pulmonary hypertension were seen over an 18-month period. One hundred eightythree patients were excluded from the analysis because inclusion criteria were not met, including 42 patients with left-heart disease, 42 patients with lung disease, 25 patients with other forms of pulmonary hypertension, 39 patients with normal hemodynamics at catheterization, and 35 patients excluded for other reasons; additional details are given in Table 1. Of the remaining 431 patients with PAH or CTEPH, 91 patients (21%) were excluded due to incomplete or missing stimulant use histories. Rates of complete stimulant use histories were significantly higher in the idiopathic PAH group (87%) than in the group with PAH and a known risk factors (79%), and in the CTEPH group (74%). The final sample of 340 patients included 97 patients with idiopathic PAH, 106 patients with PAH and known risk factors, and 137 patients with CTEPH. 1658 Original Research Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians More women than men were seen in all patient groups, with women making up 56.2% of the CTEPH group, 72.2% of the idiopathic PAH group, and 88.7% of the group with PAH and known risk factors (Table 2). Patients in the CTEPH group were oldest, with a mean age of 53.0 years, compared with 49.1 years for those with PAH and known risk factors, and 47.1 years for those with idiopathic PAH. Thirty-eight patients reported exposure to a stimulant-type drug, including 28 patients with a diagnosis of idiopathic PAH, 6 patients with CTEPH, and 4 patients with PAH and known risk factors (Table 3; Fig 1). Methamphetamine use was reported most frequently, with 23 patients reporting methamphetamine use alone and 8 patients reporting use of both methamphetamine and cocaine. Three patients had taken amphetamines illicitly, and two others reported amphetamine use as a diet pill (although one patient had also used cocaine). Cocaine use alone was uncommon, with only three patients describing cocaine use without methamphetamine or amphetamine use. Route of exposure was described for 11 patients, including 2 patients who had used stimulants IV, and 9 patients who had used stimulants through non-IV routes (inhaled, smoked, or oral). Patients with reported stimulant use were significantly younger than patients without reported use (mean age, 44.5 years vs 50.9 years; p ⫽ 0.006), but no significant differences in rates of use by race or gender were seen. Duration of use was not available in all cases and was reported only as “long term” or “frequent” in others, but 15 patients did report a general duration of use ranging from 6 months to 25 years; Tables 4, 5 provide additional details. Two patients had positive toxicology screen results at diagnosis, and two other patients required hospitalizations for PAH exacerbations after resuming drug use despite initial improvement with treatment. Table 3—Specific Stimulants Taken by Pulmonary Hypertension Group* Variables Methamphetamine alone Amphetamine alone Cocaine alone Methamphetamine plus cocaine Amphetamine plus cocaine Total Idiopathic PAH (n ⫽ 97) PAH With Known Risk Factors (n ⫽ 106) CTEPH (n ⫽ 137) 16 3 1 7 4 0 0 0 2 0 2 1 1 0 1 28 4 6 *Data are presented as No. of patients. Prior to adjustment for potential confounders, patients with idiopathic PAH were significantly more likely to have a history of stimulant use than patients in either of the comparison groups, with an odds ratio of 10.35 (95% confidence interval, 3.47 to 30.8; p ⬍ 0.0001) for idiopathic PAH compared with PAH and known risk factors, and 8.86 (95% confidence interval, 3.5 to 22.4; p ⬍ 0.0001) for idiopathic PAH compared with CTEPH (Table 6). The odds ratios changed only modestly with the addition of age, gender, and race into the model, and no significant interaction between these possible confounders and stimulant drug use was seen. After backwards elimination using the prespecified criteria, gender and race were removed from the model, and age was retained due to a modest decrease in the odds ratio for CTEPH compared with idiopathic PAH patients. The final age-adjusted odds ratios for a prior stimulant history were 10.14 (95% confidence interval, Table 2—Demographics by Diagnosis Group Variables Patients, No. Mean age, yr Mean pulmonary artery pressure, mm Hg Female gender, % Race, % White Black Hispanic Asian/Pacific Island Other or unknown www.chestjournal.org Idiopathic PAH PAH With Known Risk Factors CTEPH 97 47.2 50.2 106 49.1 42.2 137 53.0 46.5 72.2 88.7 56.2 74.2 5.2 11.3 3.1 6.2 75.5 3.8 6.6 8.5 4.7 81.8 13.1 2.1 2.2 0.7 Figure 1. As shown, 28.9% of patients with idiopathic PAH reported prior stimulant use, compared with 3.8% of patients with PAH associated with other risk factors, and 4.4% of patients with CTEPH (p ⬍ 0.0001 for comparison between idiopathic PAH and PAH with known risk factors, and between idiopathic PAH and CTEPH). Graph shows proportion and 95% confidence interval. CHEST / 130 / 6 / DECEMBER, 2006 Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians 1659 Table 4 —Idiopathic PAH: Drug Use Histories Age, yr Gender Uncertain Duration of Use Date of Diagnosis Most Recent Mean Pulmonary Artery Pressure, mm Hg 33 Male 2002 50 36 Female 2003 41 36 37 Female Male 2004 2003 53 56 37 Female 2004 79 38 40 41 42 43 Female Male Male Female Male 1999 1999 2001 2003 2004 68 65 39 44 51 46 47 48 49 Female Female Female Male 2003 2000 2002 1998 53 61 46 45 53 Female 1998 52 60 Female 2003 52 30 34 40 41 42 42 42 45 51 54 57 67 Female Female Male Female Female Male Female Female Female Male Male Female 2003 2000 1999 2004 2001 2003 2002 1999 2004 1999 2004 2003 58 63 33 55 49 39 29 58 45 63 49 40 Probable Duration of Use ⱖ 6 mo Long-term use of multiple drugs including heroin, cocaine (last use 1984), and methamphetamine (last use 1999). Inhaled methamphetamine long term; none for “a few days” prior to diagnosis; possible prior IV drug use. Methamphetamine use from age 18 to 22 yr. Methamphetamine use approximately 12 yr prior to diagnosis over a period of at least 6 mo; none IV. Crystal methamphetamine and cocaine use for 4 to 5 yr during the 1990s. Inhaled methamphetamine use for 17 yr; last approximately 1994. Amphetamines for 20 yr. Methamphetamine use over approximately 7 yr. Methamphetamine “during college years”, none IV. Fifteen years of crystal methamphetamine and cocaine use continuing until 5 d prior to hospital admission and diagnosis. Cocaine and methamphetamine use for 13 yr; none for 5 yr. Methamphetamine use for 15 yr; last use 1998. Crystal methamphetamine “on and off for years”. Cocaine, methamphetamine, and heroin IV for 25 yr; multiple overdose episodes and several arrests; last use 1992. Methamphetamine and cocaine use for 20 yr; in 2002, reported none used “recently”; no history of IV drug abuse. Amphetamine containing diet pills in the 1960s and cocaine use in the 1980s; none since approximately 1997. Methamphetamine use continuing up until diagnosis, none IV.* Methamphetamine use.* Inhaled crystal methamphetamine use.* Methamphetamine and cocaine use, last use 1 yr prior to diagnosis.* Cocaine use.* Methamphetamine use.* Methamphetamine use.* Amphetamine history, none in many years.* Methamphetamine use (snorted) up until ⬍ 1 mo prior to diagnosis.* Methamphetamine use; “none for 4 yr”.* Crystal methamphetamine use.* Amphetamine containing diet pills in her twenties.* *Uncertain duration of use. 3.39 to 30.3; p ⬍ 0.0001) for idiopathic PAH compared with AH with known risk factors, and 7.63 (95% confidence interval, 2.99 to 19.5; p ⬍ 0.0001) for idiopathic PAH compared with CTEPH. Odds ratios for methamphetamine use were also significant. Amphetamine use and cocaine use alone were too infrequent to evaluate separately. Although HIV and portal hypertension patients were excluded from the study, data on rates of stimulant use were recorded for these groups. Eighty-nine percent (eight of nine patients) with HIV and PAH reported prior stimulant use, and 20% (one of five patients) with portal hypertension had taken stimulants. Due to small numbers as well as the lack of an appropriate control group, formal statistical analysis was not performed. Discussion The central finding of this study was that methamphetamine exposure appears to be strongly associated with idiopathic PAH. Patients with idiopathic PAH were approximately 10 times more likely to have a history of stimulant use than patients with PAH and known risk factors, and almost 8 times more likely to have a history of stimulant use than patients with CTEPH, after adjustment for age. These ratios are similar to those found in studies of fenfluramine use. For example, the Surveillance of North American Pulmonary Hypertension study9 found an odds ratio of 7.5 for ⬎ 6 months of fenfluramine use comparing primary pulmonary hypertension patients to those with secondary pulmo- 1660 Original Research Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians Table 5—PAH With Risk Factors and CTEPH: Drug Use Histories Etiology Most Recent Mean Pulmonary Artery Pressure, mm Hg Date of Diagnosis Female Atrial septal defect 63 2000 Female Female Male Female Female Female Male Male Atrial septal defect Fenfluramine CTEPH CTEPH CTEPH Fenfluramine CTEPH CTEPH 97 63 45 41 53 62 76 41 2003 2003 1997 2003 2004 1997 2003 1999 Age, yr Gender 34 46 41 42 43 46 46 53 57 Probable Duration of Use ⱖ 6 mo Inhaled methamphetamines throughout adolescence and up until a hospital admission when the diagnosis of PAH was made; longest prior drug-free period was 10 d. Methamphetamines from age 18 to 40 yr; diagnosis at age 44 yr. Methamphetamine use 20 yr prior to diagnosis.* Cocaine and methamphetamine use.* Cocaine and amphetamine use in her twenties.* Crack cocaine “intermittently”.* Methamphetamine use.* Prior “rare” cocaine use.* Methamphetamine use.* *Uncertain duration of use. nary hypertension, and the International Primary Pulmonary Hypertension study10 found an odds ratio of 6.3 for “any anorexigen use” in primary pulmonary hypertension patients compared with control subjects. Rates of cocaine use alone were too infrequent to make meaningful conclusions but were included in the primary analysis, as stimulant use was defined prior to data collection. Because of methodologic limitations inherent in a retrospective chart review study, these results must be considered preliminary. Potential limitations include missing data and questions about the acceptability of the control groups. Pulmonary hypertension subtype is generally not known definitively at the time of initial consultation, and we thus expected to find similar rates of missing data. However, 21% of patients with PAH and risk factors and 26% of patients with CTEPH had missing or incomplete stimulant use histories, compared with only 13% of patients believed to have idiopathic PAH. Negative stimulant-use histories may have been more likely to be recorded as “noncontributory” or “unremarkable” (considered incomplete), but this does not completely explain the different rates of missing data. Another concern is that patients with CTEPH may be referred from a wider geographic region, potentially affecting rates of stimulant use. The use of a second control group made up of patients with PAH associated with other risk factors should be reassuring, as the referral pattern in these patients is generally similar to that of patients with idiopathic PAH. Exclusion of individual subgroups within the PAH with risk factors group (for example, excluding those with fenfluramine use) also did not appreciably change the calculated odds ratios. A final concern is that other chronic illnesses in the two comparison groups might somehow decrease the rates of stimulant drug use below that of a normal population. This is a potential factor, though the rate of methamphetamine use in our two control populations was only slightly lower than nationally reported rates. Further, in most cases the symptoms and disability from pulmonary hypertension are more severe than the symptoms of any associated condition. Despite these methodologic limitations, the finding that 28 of 97 patients with idiopathic PAH have a history of stimulant use is important and suggestive Table 6 —Odds of Stimulant Use in Idiopathic PAH, PAH With Known Risk Factors, and CTEPH* Variables Idiopathic PAH vs PAH With Known Risk Factors Idiopathic PAH vs CTEPH Any stimulant use Unadjusted Full model (includes age, gender, and race) Final model Methamphetamine, final model 10.35 (3.47–30.8); p ⬍0.0001 10.05 (3.32–30.4); p ⬍ 0.0001 10.14 (3.39–30.3); p ⬍ 0.0001† 7.73 (2.55–23.5); p ⫽ 0.0002‡ 8.86 (3.5–22.4); p ⬍ 0.0001 8.14 (3.14–21.1); p ⬍ 0.0001 7.63 (2.99–19.5); p ⬍ 0.0001† 11.61 (3.34–40.3); p ⬍ 0.0001‡ *Data are presented as odds ratio (95% confidence interval). †Final odds ratios for any stimulant use are adjusted for differences in age; gender and race were not significant confounders and were removed from the model. Patients with idiopathic PAH were significantly more likely to have taken stimulants compared with other pulmonary hypertension patients. Older patients were slightly less likely to have used stimulants; this results in a decrease in the odds ratios after adjustment for age. ‡Age-adjusted odds of any methamphetamine use. Amphetamine and cocaine use were too infrequent to analyze separately. www.chestjournal.org CHEST / 130 / 6 / DECEMBER, 2006 Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians 1661 of an association. The far-lower rates of stimulant use found in the two comparison groups with pulmonary hypertension add strength to this observation and suggest that these findings are not just related to the geographic location or some other aspect of our patient population. While the results of retrospective studies may be considered preliminary and less robust than more formal case-control studies, they can provide some evidence of an association along with the rationale needed to conduct additional studies. For example, the observation by Brenot et al11 of frequent anorexigen use in a population with primary pulmonary hypertension coupled with increasing use of these medications led to the performance of the International Primary Pulmonary Hypertension study,10 definitively linking anorexigen use with the development of PAH. The mechanisms through which methamphetamine use could lead to pulmonary hypertension are unknown, and in vivo studies evaluating the effects of stimulants on the pulmonary vasculature are limited. One small study12 showed increased pulmonary arterial pressures after methamphetamine administration in humans, while another study13 showed that cocaine administration failed to increase pulmonary arterial pressures. Similarities in pharmacology between amphetamines and the diet drug fenfluramine, a known risk factor for PAH, suggest that a common receptor or pathway may exist. Like fenfluramine, amphetamines are “substrate-type” releasers,14 increasing neurotransmitter release via substrate-mediated exchange and through disruption of intracytoplasmic storage vesicles. Fenfluramine is specific for the serotonin transporter protein, while methamphetamine and amphetamine act more potently on norepinephrine and dopamine transporters with modest activity on the serotonin transporter15 (Fig 2). Figure 2. Although all three molecules are structurally similar, amphetamine and methamphetamine are more potent releasers of dopamine and norepinephrine and relatively weak releasers of serotonin, while fenfluramine acts mainly on serotonin release.15 Serotonin and norepinephrine have both been proposed as potential contributors to the development of pulmonary hypertension. Both have vasoconstrictive and growth modulating effects on smooth-muscle cells, and their transporters are present in the pulmonary vasculature.16 –20 The serotonin transporter itself may also be important, as levels of this transporter are increased in idiopathic PAH, its overexpression in mice leads to modest increases in right ventricular systolic pressures, and serotonin transporter antagonists can block serotonin-mediated smooth-muscle cell growth in vitro.21,22 If an association between stimulants and PAH exists, it will be important to determine whether only certain stimulants are associated or whether it is a class effect. In this study, only 2 patients with idiopathic PAH reported prescription amphetamine use, compared with 1 patient reporting illicit amphetamine use, 24 patients reporting illicit methamphetamine use, and 1 patient reporting illicit cocaine use. The majority of illicit methamphetamine users in national surveys report either inhaling or smoking the drug23,24; this direct exposure of drug to the pulmonary vasculature may also be an important determinant of overall risk. The high rate of stimulant use among the nine (excluded) HIV patients with PAH is also intriguing: HIV infection is considered to be a “definite” PAH risk factor,25 but how HIV leads to pulmonary hypertension remains unclear, as neither CD4 count or viral load have correlated well with the development of PAH.26 Higher-than-expected rates of IV drug use have been reported in some series,27 but rates of non-IV stimulant use have not been described. Higher rates of use might have been expected among patients with PAH associated with known risk factors compared with patients with CTEPH, based on pathophysiology in these forms of PAH that is presumably more similar to idiopathic PAH than CTEPH. It is unclear whether the lack of this finding relates to a true lack of added risk vs limitations in study design. In summary, this study found a significant association between stimulant use and idiopathic PAH, and suggests that stimulant use may be a risk factor for PAH. Though preliminary, these results are important because of the widespread and increasing use of both prescription and illicit stimulants. Additional study of a wider spectrum of stimulant drugs is warranted to more clearly define this risk, and particular focus on the HIV-associated PAH subgroup is needed to clarify the role of stimulant use in this patient population. 1662 Original Research Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians ACKNOWLEDGMENT: We thank Cindy Morgan, MS, and Fernando Torres, MD, for assistance in statistical analysis and manuscript preparation. 14 References 1 Simonneau G, Galie N, Rubin LJ, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004; 43:5S– 12S 2 Collazos J, Martinez E, Fernandez A, et al. Acute, reversible pulmonary hypertension associated with cocaine use. Respir Med 1996; 90:171–174 3 Yakel DL Jr, Eisenberg MJ. Pulmonary hypertension in chronic intravenous cocaine users. Am Heart J 1995; 130: 398 –399 4 Schaiberger PH, Kennedy TC, Miller FC, et al. Pulmonary hypertension associated with long-term inhalation of “crank” methamphetamine. Chest 1993; 104:614 – 616 5 Olfson M, Gameroff MJ, Marcus SC, et al. National trends in the treatment of attention deficit hyperactivity disorder. Am J Psychiatry 2003; 160:1071–1077 6 Lifetime use of specific stimulants and prescription diet pills. 2003 national household survey on drug abuse, Appendix G. Available at: http://oas.samhsa.gov/NHSDA/2k3NSDUH/ appg.htm#tabg.2. Accessed November 17, 2006 7 National survey on drug use and health: the NSDUH report. September 16, 2005. Available at: www.oas.samhsa.gov. Accessed November 17, 2006 8 Chin K, Channick R, Kim N, et al. Most patients with PAH have identifiable risk factors and these risk factors vary by gender [abstract]. Am J Respir Crit Care Med 2004; 171:A56 9 Rich S, Rubin L, Walker A, et al. Anorexigens and pulmonary hypertension in the United States: results from the surveillance of North American pulmonary hypertension. Chest 2000; 117:870 – 874 10 Abenhaim L, Moride Y, Brenot F, et al. Appetite-suppressant drugs and the risk of primary pulmonary hypertension. International Primary Pulmonary Hypertension Study Group. N Engl J Med 1996; 335:609 – 616 11 Brenot F, Herve P, Petipretz P, et al. Primary pulmonary hypertension and fenfluramine use. Br Heart J 1993; 70:537– 541 12 Kneehans S, Sziegoleit W, Krause M, et al. Clinical-pharmacological studies on the effect of mephantermine and methamphetamine on the hemodynamics of the lung circulation [in German]. Z Gesamte Inn Med 1975; 30:227–230 13 Kleerup EC, Wong M, Marques-Magallanes JA, et al. Acute www.chestjournal.org 15 16 17 18 19 20 21 22 23 24 25 26 27 effects of intravenous cocaine on pulmonary artery pressure and cardiac index in habitual crack smokers. Chest 1997; 111:30 –35 Rothman RB, Ayestas MA, Dersch CM, et al. Aminorex, fenfluramine and chlorphentermine are serotonin transporter substrates: implications for primary pulmonary hypertension. Circulation 1999; 100:869 – 875 Rothman RB, Baumann MH. Therapeutic and adverse actions of serotonin transporter substances. Pharm Ther 2002; 95:73–78 Tseng YT, Padbury JF. Expression of a pulmonary endothelial norepinephrine transporter. J Neural Transm 1998; 105: 1187–1191 Marcos E, Fadel E, Sanchez O. Serotonin-induced smooth muscle hyperplasia in various forms of human pulmonary hypertension. Circ Res 2004; 94:1263–1270 Belohlavkova S, Simak J, Kokesova A, et al. Fenfluramineinduced pulmonary vasoconstriction: role of serotonin receptors and potassium channels. J Appl Physiol 2001; 91:755–761 Erami C, Zhang H, Ho JG, et al. ␣(1)Adrenoceptor stimulation directly induces growth of vascular wall in vivo. Am J Physiol Heart Circ Physiol 2002; 283:H1577–H1587 Salvi SS. ␣1-Adrenergic hypothesis for pulmonary hypertension. Chest 1999; 115:1708 –1719 Marcos E, Fadel E, Sanchez O, et al. Serotonin-induced smooth muscle hyperplasia in various forms of human pulmonary hypertension. Circ Res 2004; 94:1263–1270 MacLean MR, Deuchar GA, Hicks MN, et al. Overexpression of the 5-hydroxytryptamine transporter gene: effect on pulmonary hemodynamics and hypoxia-induced pulmonary hypertension. Circulation 2004; 109:2150 –2155 The Dasis Report: Primary methamphetamine/amphetamine treatment admissions: 1992–2002. Available at: http://oas. samhsa.gov/2k4/methTX/methTX.htm. Accessed October 10, 2004 Wu LT, Pilowsky DJ, Wechsberg WM, et al. Injection drug use among stimulant users in a national sample. Am J Drug Alcohol Abuse 2004; 30:61– 83 Humbert M, Nunes H, Sitbon O, et al. Risk factors for pulmonary arterial hypertension. Clin Chest Med 2001; 22: 459 – 475 Mehta NJ, Khan IA, Mehta RN, et al. HIV-related pulmonary hypertension: analytic review of 131 cases. Chest 2000; 118:1133–1141 Nunes H, Humbert M, Sitbon O, et al. Prognostic factors for survival in human immunodeficiency virus associated pulmonary arterial hypertension. Am J Respir Crit Care Med 2003; 167:1433–1439 CHEST / 130 / 6 / DECEMBER, 2006 Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians 1663 Is Methamphetamine Use Associated With Idiopathic Pulmonary Arterial Hypertension? Kelly M. Chin, Richard N. Channick and Lewis J. Rubin Chest 2006;130;1657-1663 DOI 10.1378/chest.130.6.1657 This information is current as of April 13, 2008 Updated Information & Services Updated information and services, including high-resolution figures, can be found at: http://chestjournal.org/cgi/content/full/130/6/1657 References This article cites 17 articles, 9 of which you can access for free at: http://chestjournal.org/cgi/content/full/130/6/1657#BIBL Citations This article has been cited by 1 HighWire-hosted articles: http://chestjournal.org/cgi/content/full/130/6/1657 Permissions & Licensing Information about reproducing this article in parts (figures, tables) or in its entirety can be found online at: http://chestjournal.org/misc/reprints.shtml Reprints Information about ordering reprints can be found online: http://chestjournal.org/misc/reprints.shtml Email alerting service Receive free email alerts when new articles cite this article sign up in the box at the top right corner of the online article. Images in PowerPoint format Figures that appear in CHEST articles can be downloaded for teaching purposes in PowerPoint slide format. See any online article figure for directions. Downloaded from chestjournal.org on April 13, 2008 Copyright © 2006 by American College of Chest Physicians