Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
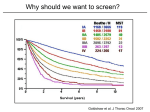
National Lung Screening Trial Design Specifications Ella A. Kazerooni, M.D. Professor & Director Cardiothoracic Radiology Associate Chair for Clinical Affairs University of Michigan Lung Cancer Screening Outline Background NLST Design NSLT Results What’s next? Lung Cancer Screening Background Leading cause of cancer death in both men & women Estimated Cancer Cases & Deaths ACS Facts & Figures 2010 New Cases Deaths Breast 209,060 (14%) 40,230 (7%) Prostate 217,730 (14%) 32,050 (6%) Colorectal 142,570 (9%) 51,370 (9%) Lung 222,520 (15%) 157,300 (28%) All Sites 1,529,560 569,490 5-Year Relative Survival Rates by Stage 1999-2005 (NCI/SEER) All Local Regional Distant Breast 89% 98% 84% 23% Colorectal 65% 91% 70% 11% Prostate 100% 100% 100% 31% Lung/Bronchus 16% 53% 24% 4% Pancreas 6% 22% 9% 2% Esophagus 17% 37% 19% 3% Lung Cancer Screening Background Large population at risk due to cigarette smoking and second hand smoke exposure • ≈ 60 million current smokers (19.3% of U.S. adults in 2010; 3 million fewer than 20.9% in 2005 • ≈ 30 million former smokers • Tobacco: leading cause of preventable death & illness; responsible for 1 in 5 deaths Smoking in the U.S. CDC. Vital Signs: Current Cigarette Smoking Among Adults Aged ≥ 18 Years ― United States 2005-2010. Morbidity and Mortality Weekly Report 2011;60(35):1207-1211 Low: Utah & California High: Kentucky & West Virginia Smoking in the U.S. 90% of new smokers begin as teenagers every day ≈ 3500 kids aged 12-17 smoke for the first time American Academy of Pediatrics Source: CDC Office of Smoking and Health; National Center for Tobacco-Free Kids Second Hand Smoke in U.S. 2006 US Surgeon General Report: The Health Consequences of Involuntary Exposure to Tobacco Smoke; and ACS Facts & Figures 2010 • > 126 million are exposed to SHS • 3,400 lung cancer deaths / year • 46,000 heart disease deaths / year • SHS exposure is declining • 84% in 1988-94 to 46% in 1999-2004 • 74% of population is covered by smoke free policies in work places and restaurants/bars Lung Cancer Screening Background Many single arm prospective cohort studies using low dose helical CT have demonstrated: − Smaller size and lower stage of screen detected cancers (stage shift) compared to symptom detected cancer CT Lung Cancer Screening Trials Prevalence Results Kaneko Sone ELCAP Swensen Diederich Fl/Moffitt Japan N nodules 1369 5483 1000 1520 817 1150 7956 13.1% 12.3% 23% 51% 43% 35% 26% cancer stage I 0.38% 0.48% 2.7% 1.3% 1.3% 3.0% 0.4% 93% 84% 85% 71% 58% 44% 86% CT Lung Cancer Screening Trials Prevalence Results N Sone ELCAP Swensen Diederich Nawa 5483 1000 1520 817 7986 cancers (≤ 1cm) 23 (6; 27%) 31 (15; 56%) 27 (9; 34%) 12 (0; 0%) 37 (6; 16%) mean size 15 mm 15 mm 17 mm 25 mm 17 mm Lung Cancer Screening Background Many single arm prospective cohort studies using low dose helical CT have demonstrated: − Smaller size and lower stage of screen detected cancers (stage shift) compared to symptom detected cancer − Improved survival I-ELCAP 10-Year Survival I-ELCAP Investigators; NEJM 2006;355:1763-1771 31,567 persons screened 1993-2005 27,456 repeat screenings 1994-2005 7-18 m after baseline 484 lung cancers 412 (85%) stage I lung ca 88% 10 yr survival 302 stage I lung ca resected within 1 m of dx 92% 10 yr survival Biases of Early Detection lead time (earlier diagnosis) length (less rapid progression) over diagnosis (pseudodisease) Natural History of Cancer Preclinical Clinical DPCP disease detectable onset by test signs & sx death DPCP = detectable preclinical phase Lead Time Bias disease disease Test + s/sx death s/sx death lead time false calculation of improved survival Length Bias slowly progressive disease more amenable to detection than disease that develops and progresses quickly between screenings screened cases less aggressive than sx cases diagnosis disease DPCP indolent aggressive diagnosis DPCP death death Pseudodisease – Overdiagnosis Bias Inherent in screening disease that would have remained subclinical if not detected at screening − does not progress to symptomatc disease (DCIS) − patient dies of something else (prostate ca) autopsy prevalence of disease higher than clinical prevalence of disease − up to 16% of lung cancer not suspected before death pathologic misdiagnosis (hyperplasia vs. ca) Lung Cancer Screening Background Leading cause of cancer death in both men & women Large population at risk Many single arm prospective cohort studies using low dose helical CT have demonstrated: − Improved survival − Lower stage of screen detected cancers (stage shift) No screening test has been shown to reduce lung cancer mortality N LST National Lung Screening Trial National Cancer Institute Denise R. Aberle, MD Cancer Imaging Program, DCTD | NCI David Geffen School of Medicine at UCLA National PI, ACRIN-NLST American College of Radiology Imaging Network Christine D. Berg, MD Chief, Early Detection Research Group Division of Cancer Prevention | NCI Project Officer, LSS-NLST Lung Screening Feasibility Study of the PLCO Trial ACRIN American College of Radiology Imaging Network Funded in 1998 by NCI as a non-member network Conducts clinical trials of imaging research to lengthen & improve the quality of cancer patient’s lives First 10 years: enrolled > 76,000 subjects, collected > 20 million images & over 50 publications Major trials: − DMIST – Digital Mammographic Imaging Screening Trial 2001 − NLST – National Lung Screening Trial 2002 − National CT Colonography Trial 2005 − RESCUE 2011 PLCO Prostate, Lung, Colorectal & Ovarian Cancer Screening Trial These 4 cancers account for approx. 40% of new cancers diagnosed & 45% of cancer deaths in U.S. 10 site clinical trial to determine if screening reduces mortality; run by NCI’s Cancer Division of Cancer Prevention Half screening tests / half routine health care Enrolled 155,000 men & women aged 55-74 years between 1992 and 2001 Screening ended 2006; 10 year follow up in progress NLST Design NLST Design NLST Research Team. Radiology 2011; 258:243-253 Multicenter, randomized trial Low dose helical CT vs. CXR Current and former heavy smokers (≥ 30 pack-yrs) Age 55-74 years Does early detection reduce lung cancer specific mortality? • 5-year survival stage IA 70% • 5-year survival stage IV 5% • > 75% lung cancer patients present with locally advanced or metastatic disease NLST Design Arms Helical CT vs. CXR Difference in lung cancer-specific mortality 20% α 5% Power 90% Compliance 85% CT | 80% CXR Contamination 5% CT | 10% CXR Size 25,000 / arm NLST: Endpoints Primary: Secondary: Lung cancer specific mortality All cause mortality Lung cancer incidence Lung cancer stage distribution Diagnostic performance Adverse impact of diagnostic evaluation NLST-ACRIN: Substudies Analyses: Cost effectiveness analysis Health care resource use Effect of screening on quality of life T0, T1, T2; SF-36, EQ-5D; 16 sites Effect of (+) screen on anxiety T0, 30 days post screen & q 6 mths SF-36, EQ-5D, STAI Smoking cessation NLST Biorepository 15 ACRIN sites collected serial blood, urine & sputum specimens annually x 3 for validation of biomarkers (n = 10,260) All sites collected lung cancer specimens in paraffin blocks Available to researchers through a peer-review process NLST – 33 Participating Sites LSS si NLST: CXR Technique NLST Research Team. Radiology 2011; 258:243-253 PA Inspiratory CXR CR or DR, some film-screen Average effective dose 0.02 mSv NLST: CT Technique Cagnon CH, et al. Academic Radiology 2006; 13:1431-1441 Target Technique based on − − − − Detect and follow nodules ≥ 4 mm Single breath-hold Avoid edge enhancement at nodule borders Low radiation exposure (av effective dose 1.5 mSv) CT Technique Chart − − − − Standardized 18 parameters 14 different CT scanner platforms 4 manufacturers: 4-64 channel Individualized protocols NLST: CT Technique Chart GE-VCT(64) 64 slice | 0.5 sec Siemens Sensation 64 64 x 0.0.6 Phillips MX8000 16 slice | 0.5 sec 16 x .75 Toshiba Aquillon 16 slice | 0.5 sec 120 120 120 120 Gantry Rotation Time 0.5 sec 0.5 sec 0.5 sec 0.5 sec mA (Regular-Large Patient) 50-100 50-100 75-15- 80-160 mAs (Regular-Large) 25-50 25-50 37.5-75 40-80 Scanner Effective mAs (Reg-Large) 27-53 25-50 25-50 26.7-53.3 0.625 mm 0.6 mm .75 mm 2 mm Number of Active Channels: N 64 32 16 16 Detector configuration: N x T 64 x 0.625 mm 32 x 0.6 mm 16 x 0.75 16 x 2 MODE (Thick/Speed) or Console Collimation1 .625/.984/39.37 64 x 0.6 mm N/A N/A 39.37 mm 19.2 mm 18 mm 48 mm 0.984 1.0 1.5 1.5 Table speed (mm/second) 78.74 mm/sec 38.4 mm/sec 36 mm/sec 96 mm/sec Scan time (40 cm thorax) 5.1 sec 11 sec 11 sec 4.2 sec Max Nominal Reconstructed Slice Width 2.5 mm 2 mm 2 mm 2 mm Reconstruction Interval 2.0 mm 1.8 mm 1.8 mm 1.8 mm Reconstruction Algorithm STD B30f B or C FC 10 # Images/Data set (40 cm Thorax) 200 223 223 223 2.2-2.4 mGy 1.9-3.8 mGy 1.9-3.8 mGy 2.7-5.4 mGy Parameter kV Detector Collimation (mm): T Table Incrementation (mm/rotation): I Pitch ([mm/rotation]/configuration): I/NT CTDIvol Dose in mGy (Regular-Large) CT Scanners in NLST: # of Detectors Cody DD et al. Americam Journal of Roentgenology 2010;194:1539-1546 NLST: Positive CT Screen Definition nodule 4 mm indeterminate nodule » new nodule 4-10 mm » growing nodule < 7 mm » f/u CT 6, 12, 24 months abnormal » » » » new nodule > 10 mm growing nodule > 7 mm nodule enhancement CT or FDG-PET (+) nodules: definitive biopsy/diagnosis NOTE: no trial wide algorithms for evaluation & treatment NLST Cumulative Accrual NLST Cumulative Accrual 60000 Total (53,464) 50000 Participants 40000 LSS (34,614) 30000 20000 ACRIN (18,850) 10000 0 Aug-02 Nov-02 Feb-03 May-03 Aug-03 Month Enrolled Nov-03 Feb-04 NLST Timeline 6th Interim Analysis 5th Interim Analysis 4th Interim Analysis T2 3rd Interim Analysis T1 2nd Interim Analysis time 9/09 9/10 10/20/10 9/07 9/08 9/06 9/05 9/04 9/03 9/02 1st Interim Analysis T0 National Lung Screening Trial Design Specifications Ella A. Kazerooni, M.D. Professor & Director Cardiothoracic Radiology Associate Chair for Clinical Affairs University of Michigan NLST: Subjects – Age & Gender NLST: Subjects – Race/Ethnicity NLST: Subjects – Smoking History NLST Demographics vs. US Population United States Census Department Tobacco Use Supplement of Continuing Population Survey for 20022004 Information on 240,000 respondents Reviewed subset of respondents aged 55-74, with 30+ pack year smoking, either current smoker or former smoker who quit within the past 15 years Identified smoking status, age, sex, race, ethnicity, marital status, and education NLST Demographics vs. US Population NLST US Census 59.0 58.5 55-59 (%) 60-64 (%) 65-69 (%) 70-74 (%) 42.8 30.6 17.8 8.8 35.2 29.3 20.8 14.7 Race/ethnicity Black (%) Hispanic (%) 4.4 1.7 5.5 2.4 Male (%) Age NLST Demographics vs. US Population Married Education < HS ≥ College Current smoker Median pack years NLST 66.6 US Census 60.0 6.1 31.5 21.3 14.4 48.2 48.0 57.1 47.0 NLST Demographics vs. US Population Compared with similar US population, NLST subjects have: −similar gender distribution and smoking exposure −are younger −better educated −less likely to be current smokers NLST: Family History of Lung Cancer Any first degree relative Two or more first degree relatives CT CXR Total 21.8 % 21.7 % 21.7 % 3.3 3.2 3.3 Screening Exam Compliance & Crossover Helical CT CXR Total Study Year Expected Screened Expected Screened Expected Screened T0 26,713 98.5% 26,722 97.5% 53,435 98.0% T1 26,282 94.0% 26,398 91.3% 52,680 92.6% T2 25,935 92.9% 26,097 89.5% 52,032 91.2% Compliance: 95% CT arm & 93% CXR arm Crossover: 4.3% in LSS CXR arm underwent CT NLST: Screen Positivity* Rate by Screening Round and Trial Arm CT CXR Number screened Number positive % Positive Number screened Number positive % Positive Screening round 1 26,309 7,191 27.3 26,035 2,387 9.2 Screening round 2 24,715 6,901 27.9 24,089 1,482 6.2 Screening round 3 24,102 4,054 16.8** 23,346 1,174 5.0** All 3 rounds 75,126 18,146 24.1 73,499 5,043 6.9 *A positive screen is one that may be suspicious for lung cancer. **A suspicious abnormality that has been stable for 3 rounds may be called negative according to protocol. NLST: Clinically Significant NON lung cancer by Screening Round & Trial Arm CT CXR Number screened Number % Number screened Number % Screening round 1 26,309 2695 10.2 26,035 785 3.0 Screening round 2 24,715 1519 6.1 24,089 429 1.8 Screening round 3 24,102 1408 5.8 23,346 361 1.5 All 3 rounds 75,126 5622 7.5 73,499 1575 2.1 NLST: True and False Positive Screens by Screening Round and Trial Arm CT Total positives With lung cancer Without lung cancer CXR Round 1 N (%) Round 2 N (%) Round 3 N (%) Round 1 N (%) Round 2 N (%) Round 3 N (%) 7,193 (100) 6,902 (100) 4,054 (100) 2,387 (100) 1,482 (100) 1,175 (100) 270 (4) 6,923 (96) 168 (2) 6,734 (98) 211 (5) 3,843 (95) 136 (6) 2,251 (94) 65 (4) 1,417 (96) 78 (7) 1,097 (93) Results of Interim Analysis of Primary Endpoint Reported on Oct. 20, 2010 Person years (py) Lung cancer deaths Lung cancer mortality per 100,000 py Reduction in lung cancer mortality (%) Value of test statistic Efficacy boundary 144,097.6 354 245.7 20.3 –3.21 –2.02 CXR 143,363.5 442 308.3 Arm CT Deficit of lung cancer deaths in CT arm exceeds that expected by chance, even allowing for multiple looks at the data Results of Analysis of All-cause Mortality (Secondary Endpoint) Reported on Oct. 20, 2010 Person years (py) Deaths All-cause mortality per 100,000 py Reduction in all-cause mortality (%) Value of test statistic Value for significance CT 167,389.9 1870 1117.2 6.9 –2.27 –1.96 CXR 166,328.2 1996 1200.0 Arm Deficit of deaths in CT arm exceeds that expected by chance. NLST: Cumulative # of Lung Cancers NLST: Cumulative # of Lung Cancer Deaths Kaplan-Meier Curves for Lung Cancer Mortality Table 11.5.3a Kaplan-Meier Curves for All-Cause Mortality Table 11.5.6a Kaplan-Meier Curves for Lung Cancer Case Survival (Lung Cancer Cause of Death) Table 11.5.3d ACRIN-NLST Sub-Studies Serial specimen collection for validation of biomarkers (N=10,260) − Plasma | buffy coat; sputum; urine annually x 3 yrs − Resected lung cancer specimens − Applications to use specimens for research www.acrin.org Quality of life − Differential impact of screening of QoL at T0, T1, T2 (SF-36, EQ-5D) − Differential impact of [+] screen on anxiety (SF-36, EQ-5D, STAI) Administered at T0, 30 days post [+] screen and Q 6 months) Formal cost effectiveness analysis (in conjunction with RAND) Effects of screening on smoking behaviors | beliefs − Short and long term Cancer or not? Radiation Exposure Brenner DJ et al. Radiology 2004;231:440-445 Radiation Risks Potentially Associated with Low Dose Screening • assumptions: entire US population current/former smokers age 50-75 years annual CT until age 75 (5.2 ± 0.9 mGy to lung; 60mAs) 50% compliance rate atomic bomb survivor cohort for predicting risk • expect 1.9 million lung cancers • 36,000 additional lung cancers attributed to CT • 1.8% increase in lung cancer (95% CI 0.5-5.5%) Lung Cancer Screening – what’s the future? Awaiting data publication of primary end point and importantly cost effectiveness analysis necessary when informing recommendations about screening Screening as a public health recommendation For CMS, screening requires federal legislation Many sites considering or developing high risk screening programs – what’s a best practice? Patient requests for screening CT have not been as large as expected Many interested parties, most taking a cautious approach American Cancer Society, November 4, 2010 So if you are contemplating getting screened for lung cancer—and from what I hear there are a fair number of smokers thinking of doing just that—be certain you understand what we don’t know about the benefits of getting such a test (which means we can’t say that it really saves lives) and what we do know about the downsides, as reported in this study. Remember, just because we doctors can do things doesn’t always means it’s always the best thing to do. So be cautious, and be informed. American College of Radiology As the expert organization in this area of care, the ACR is very encouraged by the NLST results. The College looks forward to working with the U.S. Department of Health and Human Services, the National Cancer Institute, patient advocacy groups, Congress and other stakeholders in addressing challenges to a potential lung cancer screening program. Until and unless a national lung cancer screening program can be put in place, we encourage all physicians to obtain as much information regarding the NLST as possible. We also encourage patients to speak with their doctors regarding the usefulness of CT scanning to screen for lung cancer in their particular cases. Lung Cancer Screening NLST results & next steps Ella A. Kazerooni, M.D. Professor & Director of Cardiothoracic Radiology University of Michigan