Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Larynx Cancer
Laryngeal cancer may also be called cancer of the larynx or laryngeal carcinoma. Most
laryngeal cancers are squamous cell carcinomas, reflecting their origin from the squamous
cells which form the majority of the laryngeal epithelium. Cancer can develop in any part of
the larynx, but the cure rate is affected by the location of the tumour. For the purposes of
tumour staging, the larynx is divided into three anatomical regions: the glottis (true vocal
cords, anterior and posterior commissures); the supraglottis (epiglottis, arytenoids and
aryepiglottic folds, and false cords); and the subglottis.
Most laryngeal cancers originate in the glottis. Supraglottic cancers are less common, and
subglottic tumours are least frequent.
Laryngeal cancer may spread by direct extension to adjacent structures, by metastasis to
regional cervical lymph nodes, or more distantly, through the blood stream. Distant
metastates to the lung are most common.
Risk factors
Smoking is the most important risk factor for laryngeal cancer. Death from laryngeal cancer
is 20 times more likely for heaviest smokers than for nonsmokers Heavy chronic
consumption of alcohol, particularly alcoholic spirits, is also significant. When combined,
these two factors appear to have a synergistic effect. Some other quoted risk factors are
likely, in part, to be related to prolonged alcohol and tobacco consumption. These include
low socioeconomic status, male sex, and age greater than 55 years.
People with a history of head and neck cancer are known to be at higher risk (about 25%) of
developing a second cancer of the head, neck, or lung. This is mainly because in a
significant proportion of these patients, the aerodigestive tract and lung epithelium have
been exposed chronically to the carcinogenic effects of alcohol and tobacco. In this
situation, a field change effect may occur, where the epithelial tissues start to become
diffusely dysplastic with a reduced threshold for malignant change. This risk may be
reduced by quitting alcohol and tobacco.
(1)
Incidence
Incidence is five in 100,000 (12,500 new cases per year) in the USA. The American Cancer
Society estimated that 9,510 men and women (7,700 men and 1,810 women) would be
diagnosed with and 3,740 men and women would die of laryngeal cancer in 2006.
Laryngeal cancer is listed as a "rare disease" by the Office of Rare Diseases (ORD) of the
National Institutes of Health (NIH). This means that laryngeal cancer affects fewer than
200,000 people in the U.S.
Each year, about 2,200 people in the U.K. are diagnosed with laryngeal cancer.
The disease is also rarely seen in Canada. The disease affected only 128 individuals in the
province of British Columbia in 2009, the majority being males.
Symptoms
The symptoms of laryngeal cancer depend on the size and location of the tumor. Symptoms
may include the following
Hoarseness or other voice changes
A lump in the neck
A sore throat or feeling that something is stuck in the throat
Persistent cough
Stridor
Bad breath
Earache ("referred")
Diagnosis
(2)
Diagnosis is made by the doctor on the basis of a medical history, physical examination,
and special investigations which may include a chest x-ray, CT or MRI scans, and tissue
biopsy. The examination of the larynx requires some expertise, which may require specialist
referral.
The physical exam includes a systematic examination of the whole patient to assess general
health and to look for signs of associated conditions and metastatic disease. The neck and
supraclavicular fossa are palpated to feel for cervical adenopathy, other masses, and
laryngeal crepitus. The oral cavity and oropharynx are examined under direct vision. The
larynx may be examined by indirect laryngoscopy using a small angled mirror with a long
handle (akin to a dentist's mirror) and a strong light. Indirect laryngoscopy can be highly
effective, but requires skill and practice for consistent results. For this reason, many
specialist clinics now use fibre-optic nasal endoscopy where a thin and flexible endoscope,
inserted through the nostril, is used to clearly visualise the entire pharynx and larynx. Nasal
endoscopy is a quick and easy procedure performed in clinic. Local anaesthetic spray may
be used.
If there is a suspicion of cancer, biopsy is performed, usually under general anaesthetic.
This provides histological proof of cancer type and grade. If the lesion appears to be small
and well localised, the surgeon may undertake excision biopsy, where an attempt is made to
completely remove the tumour at the time of first biopsy. In this situation, the pathologist
will not only be able to confirm the diagnosis, but can also comment on the completeness of
excision, i.e., whether the tumour has been completely removed. A full endoscopic
examination of the larynx, trachea, and esophagus is often performed at the time of biopsy.
For small glottic tumours further imaging may be unnecessary. In most cases, tumour
staging is completed by scanning the head and neck region to assess the local extent of the
tumour and any pathologically enlarged cervical lymph nodes.
The final management plan will depend on the site, stage (tumour size, nodal spread, distant
metastasis), and histological type. The overall health and wishes of the patient must also be
taken into account.
(3)
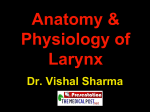
Larynx cancer - endoscopic view
Factors affect prognosis and treatment
options:
Prognosis (chance of recovery) depends on the following:
The stage of the disease.
The location and size of the tumor.
The grade of the tumor.
The patient's age, gender, and general health, including whether the patient is anemic.
Treatment options depend on the following:
The stage of the disease.
The location and size of the tumor.
Keeping the patient's ability to talk, eat, and breathe as normal as possible.
Whether the cancer has come back (recurred).
Smoking tobacco and drinking alcohol decrease the effectiveness of treatment for laryngeal
cancer. Patients with laryngeal cancer who continue to smoke and drink are less likely to be
cured and more likely to develop a second tumor. After treatment for laryngeal cancer,
frequent and careful follow-up is important.
(4)
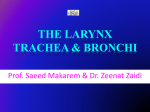
Larynx cancer.
Stages of Laryngeal Cancer
Stage 0 (Carcinoma in Situ)
In stage 0, abnormal cells are found in the lining of the larynx. These abnormal cells
may become cancer and spread into nearby normal tissue. Stage 0 is also called
carcinoma in situ.
Stage I
In stage I, cancer has formed. Stage I laryngeal cancer depends on where cancer
began in the larynx:
Supraglottis: Cancer is in one area of the supraglottis only and the vocal cords can
move normally.
Glottis: Cancer is in one or both vocal cords and the vocal cords can move normally.
Subglottis: Cancer is in the subglottis only.
Stage II
(5)
In stage II, cancer is in the larynx only. Stage II laryngeal cancer depends on where
cancer began in the larynx:
Supraglottis: Cancer is in more than one area of the supraglottis or surrounding
tissues.
Glottis: Cancer has spread to the supraglottis and/or the subglottis and/or the vocal
cords cannot move normally.
Subglottis: Cancer has spread to one or both vocal cords, which may not move
normally.
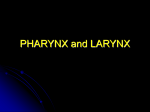
Pea, peanut, walnut, and lime show tumor sizes.
Stage III
Stage III laryngeal cancer depends on whether cancer has spread from the
supraglottis, glottis, or subglottis.
In stage III cancer of the supraglottis:
cancer is in the larynx only and the vocal cords cannot move, and/or cancer is in
tissues next to the larynx. Cancer may have spread to one lymph node on the same
side of the neck as the original tumor and the lymph node is 3 centimeters or smaller;
or
cancer is in one area of the supraglottis and in one lymph node on the same side of
the neck as the original tumor; the lymph node is 3 centimeters or smaller and the
vocal cords can move normally; or
cancer is in more than one area of the supraglottis or surrounding tissues and in one
lymph node on the same side of the neck as the original tumor; the lymph node is 3
centimeters or smaller.
(6)
In stage III cancer of the glottis:
cancer is in the larynx only and the vocal cords cannot move, and/or cancer is in
tissues next to the larynx; cancer may have spread to one lymph node on the same
side of the neck as the original tumor and the lymph node is 3 centimeters or smaller;
or
cancer is in one or both vocal cords and in one lymph node on the same side of the
neck as the original tumor; the lymph node is 3 centimeters or smaller and the vocal
cords can move normally; or
cancer has spread to the supraglottis and/or the subglottis and/or the vocal cords
cannot move normally. Cancer has also spread to one lymph node on the same side of
the neck as the original tumor and the lymph node is 3 centimeters or smaller.
In stage III cancer of the subglottis:
cancer is in the larynx and the vocal cords cannot move; cancer may have spread to
one lymph node on the same side of the neck as the original tumor and the lymph
node is 3 centimeters or smaller; or
cancer is in the subglottis and in one lymph node on the same side of the neck as the
original tumor; the lymph node is 3 centimeters or smaller; or
cancer has spread to one or both vocal cords, which may not move normally. Cancer
has also spread to one lymph node on the same side of the neck as the original tumor
and the lymph node is 3 centimeters or smaller.
Stage IV
Stage IV is divided into stage IVA, stage IVB, and stage IVC. Each substage is the
same for cancer in the supraglottis, glottis, or subglottis.
In stage IVA:
o cancer has spread through the thyroid cartilage and/or has spread to tissues
beyond the larynx such as the neck, trachea, thyroid, or esophagus. Cancer
may have spread to one lymph node on the same side of the neck as the
original tumor and the lymph node is 3 centimeters or smaller; or
o cancer has spread to one lymph node on the same side of the neck as the
original tumor and the lymph node is larger than 3 centimeters but not larger
than 6 centimeters, or has spread to more than one lymph node anywhere in the
neck with none larger than 6 centimeters. Cancer may have spread to tissues
beyond the larynx, such as the neck, trachea, thyroid, or esophagus. The vocal
cords may not move normally.
(7)
In stage IVB:
o cancer has spread to the space in front of the spinal column, surrounds the
carotid artery, or has spread to parts of the chest. Cancer may have spread to
one or more lymph nodes anywhere in the neck and the lymph nodes may be
any size; or
o cancer has spread to a lymph node that is larger than 6 centimeters and may
have spread as far as the space in front of the spinal column, around the carotid
artery, or to parts of the chest. The vocal cords may not move normally.
In stage IVC, cancer has spread to other parts of the body, such as the lungs, liver, or
bone.
Recurrent Laryngeal Cancer
Recurrent laryngeal cancer is cancer that has recurred (come back) after it has been treated.
The cancer is most likely to come back in the first 2 to 3 years. It may come back in the
larynx or in other parts of the body.
Treatment Option Overview
Different types of treatment are available for patients with laryngeal cancer. Some
treatments are standard (the currently used treatment), and some are being tested in clinical
trials. A treatment clinical trial is a research study meant to help improve current treatments
or obtain information on new treatments for patients with cancer. When clinical trials show
that a new treatment is better than the standard treatment, the new treatment may become
the standard treatment. Patients may want to think about taking part in a clinical trial. Some
clinical trials are open only to patients who have not started treatment.
1) Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of
radiation to kill cancer cells. There are two types of radiation therapy. External radiation
therapy uses a machine outside the body to send radiation toward the cancer. Internal
radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters
that are placed directly into or near the cancer. The way the radiation therapy is given
depends on the type and stage of the cancer being treated.
Radiation therapy may work better in patients who have stopped smoking before beginning
treatment. External radiation therapy to the thyroid or the pituitary gland may change the
way the thyroid gland works. The doctor may test the thyroid gland before and after therapy
to make sure it is working properly.
(8)
2) Surgery
Surgery (removing the cancer in an operation) is a common treatment for all stages of
laryngeal cancer. The following surgical procedures may be used:
Cordectomy: Surgery to remove the vocal cords only.
Supraglottic laryngectomy: Surgery to remove the supraglottis only.
Hemilaryngectomy: Surgery to remove half of the larynx (voice box). A
hemilaryngectomy saves the voice.
Partial laryngectomy: Surgery to remove part of the larynx (voice box). A partial
laryngectomy helps keep the patient's ability to talk.
Total laryngectomy: Surgery to remove the whole larynx. During this operation, a
hole is made in the front of the neck to allow the patient to breathe. This is called a
tracheostomy.
Thyroidectomy: The removal of all or part of the thyroid gland.
Laser surgery: A surgical procedure that uses a laser beam (a narrow beam of intense
light) as a knife to make bloodless cuts in tissue or to remove a surface lesion such as
a tumor.
Even if the doctor removes all the cancer that can be seen at the time of the surgery, some
patients may be given chemotherapy or radiation therapy after surgery to kill any cancer
cells that are left. Treatment given after the surgery, to lower the risk that the cancer will
come back, is called adjuvant therapy.
3) Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either
by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by
mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach
cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed
directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the
drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the
chemotherapy is given depends on the type and stage of the cancer being treated.
4) Chemoprevention
Chemoprevention is the use of drugs, vitamins, or other substances to reduce the risk of
developing cancer or to reduce the risk cancer will recur (come back). The drug isotretinoin
(9)
is being studied to prevent the development of a second cancer in patients who have had
cancer of the head or neck.
5) Radiosensitizers
Radiosensitizers are drugs that make tumor cells more sensitive to radiation therapy.
Combining radiation therapy with radiosensitizers may kill more tumor cells.
Treatment Options by Stage
A link to a list of current clinical trials is included for each treatment section. For some
types or stages of cancer, there may not be any trials listed. Check with your doctor for
clinical trials that are not listed here but may be right for you.
Stage I Laryngeal Cancer
Treatment of stage I laryngeal cancer depends on where cancer is found in the larynx.
If cancer is in the supraglottis, treatment may include the following:
Radiation therapy.
Supraglottic laryngectomy.
If cancer is in the glottis, treatment may include the following:
Radiation therapy.
Cordectomy.
Partial laryngectomy, hemilaryngectomy, or total laryngectomy.
Laser surgery.
If cancer is in the subglottis, treatment may include the following:
Radiation therapy with or without surgery.
Surgery alone.
Stage II Laryngeal Cancer
Treatment of stage II laryngeal cancer depends on where cancer is found in the larynx.
(10)
If cancer is in the supraglottis, treatment may include the following:
Radiation therapy.
Supraglottic laryngectomy or total laryngectomy with or without radiation therapy.
A clinical trial of radiation therapy.
A clinical trial of chemoprevention.
If cancer is in the glottis, treatment may include the following:
Radiation therapy.
Partial laryngectomy, hemilaryngectomy, or total laryngectomy.
Laser surgery.
A clinical trial of radiation therapy.
A clinical trial of chemoprevention.
If cancer is in the subglottis, treatment may include the following:
Radiation therapy with or without surgery.
Surgery alone.
A clinical trial of radiation therapy.
A clinical trial of chemoprevention.
Stage III Laryngeal Cancer
Treatment of stage III laryngeal cancer depends on where cancer is found in the larynx.
If cancer is in the supraglottis or glottis, treatment may include the following:
Surgery with or without radiation therapy.
Radiation therapy with or without surgery.
A clinical trial of radiation therapy.
A clinical trial of chemotherapy combined with radiation therapy, with or without
laryngectomy.
A clinical trial of radiosensitizers.
A clinical trial of chemoprevention.
If cancer is in the subglottis, treatment may include the following:
(11)
Laryngectomy plus total thyroidectomy and removal of lymph nodes in the throat,
usually followed by radiation therapy.
Radiation therapy with or without surgery.
A clinical trial of radiation therapy.
A clinical trial of chemotherapy.
A clinical trial of radiosensitizers.
A clinical trial of chemoprevention.
Stage IV Laryngeal Cancer
Treatment of stage IV laryngeal cancer depends on where cancer is found in the larynx.
If cancer is in the supraglottis or glottis, treatment may include the following:
Total laryngectomy with radiation therapy.
Radiation therapy with or without surgery.
A clinical trial of radiation therapy.
A clinical trial of chemotherapy combined with radiation therapy, with or without
laryngectomy.
A clinical trial of chemotherapy.
A clinical trial of radiosensitizers.
A clinical trial of chemoprevention.
If cancer is in the subglottis, treatment may include the following:
Laryngectomy plus total thyroidectomy and removal of lymph nodes in the throat,
usually with radiation therapy.
Radiation therapy.
A clinical trial of radiation therapy.
A clinical trial of chemotherapy combined with radiation therapy.
A clinical trial of chemotherapy.
A clinical trial of radiosensitizers.
A clinical trial of chemoprevention.
Treatment Options for Recurrent Laryngeal Cancer
(12)
Surgery with or without radiation therapy.
Radiation therapy.
Chemotherapy.
A clinical trial of chemotherapy as palliative therapy to relieve symptoms caused by
the cancer and improve quality of life.
(13)
Laryngeal papillomatosis
Laryngeal papillomatosis, also known as recurrent respiratory papillomatosis or glottal
papillomatosis, is a rare medical condition (2 per 100,000 adults and 4.5 per 100,000
children), caused by a HPV infection of the throat. Laryngeal papillomatosis causes
assorted tumors or papillomas to develop over a period. Without treatment it is potentially
fatal as uncontrolled growths could obstruct the airway. Laryngeal papillomatosis is caused
by HPV types 6 and 11, in which benign tumors form on the larynx or other areas of the
respiratory tract. These tumors can reoccur frequently, may require repetitive surgery, and
may interfere with breathing. The disease can be treated with surgery and antivirals
Transmission
In general, doctors are not sure what causes some people to contract laryngeal
papillomatosis while others who have been exposed to HPV types 6 and 11 do not contract
the disease. Since the disease is most commonly found in children the disease may be
caused by an infant contracting HPV from the mother during vaginal child birth . There is
no evidence that it is transmitted through oral sex, and it is not considered sexually
transmitted disease.
Symptom
(14)
Adults
In adults the symptoms Laryngeal papillomatosis are hoarseness, or a strained or breathy
voice. Size and placement of the tumors dictate the change in the person's voice. Breathing
difficulties may occur but more commonly are found in children.
Children
In babies and small children the symptoms include a weak cry, trouble swallowing, noisy
breathing, and chronic cough. Noisy breathing may be a stridor, which can sound like a
whistle or a snore, and is a sign that the laryngeal or tracheal parts of the airway are
narrowing.
Diagnosis
A doctor may diagnose laryngeal papillomatosis by placing a mirror into a patient's mouth
to reflect light onto the vocal cords and examining the larynx. More often, a doctor or a
trained speech-language pathologist diagnoses laryngeal papillomatosis by an indirect
laryngoscopy in the office. This procedure involves the placement of a flexible, fiber optic
camera through the patient's nose to view the vocal folds in the throat or the use of a
straight, rigid camera placed through the mouth to view the vocal folds.
The most accurate way to diagnose laryngeal papillomatosis is for a biopsy to be conducted
and for the lesion to be tested for HPV. This procedure takes place in an operating room
with the patient under general anesthesia. This is sometimes the best option for small
children. This disease is most often misdiagnosed as asthma, croup, or chronic bronchitis.
The consequences may be serious, as papillomas are at least partially obstructing the airway
to cause these symptoms and should be removed immediately.
Treatment
Traditional surgery and carbon dioxide laser surgery, a "no touch" removal of affected
tissue, are forms of treatment for laryngeal papillomatosis. Carbon dioxide laser removal is
the most common removal method.The carbon dioxide laser must be used precisely to
prevent scarring, fibrosis, and laryngeal web malformation. In children, carbon dioxide laser
is effective for removing papillomas on the larynx. Photodynamic
therapy controls tumors by using targeted dyes and bright light to illuminate tumors.In this
procedure, a doctor injects a light sensitive dye that is only absorbed by the tumors. Then
the doctor activates the dye using a bright light, and the tumors are eliminated. This
procedure has also been able to decrease the number of tumors that reoccur.Another method
(15)
istracheotomy, which reroutes air around the affected area. An incision is made in the front
of the patient's neck, and a breathing tube is inserted through a hole (stoma) into the
windpipe. The patient is then able to breathe through the tube. Although this is usually
temporary, some patients must use the tube indefinitely.This method should be avoided if at
all possible, since insertion of a breathing tube may cause the tumors to form as far down as
the lungs.Many Antiviral drugs like Cidofovir have been used to treat laryngeal
papillomatosis, but none completely stops the tumors from growing. Most antivirals are
injected to control the frequency of tumor growth. The efficacy of the same is debated and
subject to research. Some side effects of antivirals include dizziness, headaches, and body
aches. Regardless of the treatment used, the tumors will reoccur. In severe cases, tumors
may occur once or twice a month. In less severe cases, tumors may occur once or twice a
year.
References
(16)
Ridge JA, Glisson BS, Lango MN, et al. "Head and Neck Tumors"
in Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ (Eds)
Cancer Management: A Multidisciplinary Approach. 11 ed. 2008.
Laryngeal cancer at Mount Sinai Hospital
Samuel W. Beenken, MD. "Laryngeal Cancer (Cancer of the
larynx)". Laryngeal Cancer (Cancer of the larynx). Armenian Health
Network, Health.am. Retrieved 2007-03-22.
"Annual Report on the Rare Diseases and Conditions Research".
National Institutes of Health. Retrieved 2007-03-22.
"Causes of laryngeal cancer". Cancerbackup-cancerbackup.org.uk.
Retrieved 2007-03-22.
(17)