Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
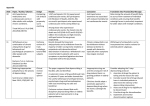
Long-Term Care Updates June 2016 By Daniel Kerner, Pharm D & Yunuo (Enora) Wu, PharmD Proton pump inhibitors (PPIs) are among the top three most commonly prescribed medication classes in the United States and among the top 10 most widely used drugs in the world.1,2 This class of medications works to suppress gastric H+/K+ ATPase by irreversibly inhibiting active proton pumps in the gastrointestinal system.1 Due to their effective acid-suppressing effect, PPIs are approved for a variety of indications. There are currently six different PPIs available on the U.S. market, with no major differences in efficacy. Their FDA-approved indications and recommended duration of therapy are summarized in the table below. Although PPIs have been considered safe and effective medications with few immediate side effects, recent literature suggests that PPIs may be associated with long-term adverse effects, calling into question the appropriate usage and duration of therapy for this medication class.3 This article will describe potential adverse effects associated with long-term use of PPIs and suggest when PPIs should be appropriately recommended. Dexlansoprazole Esomeprazole Lansoprazole Omeprazole Pantoprazole Rabeprazole Eradication of — 10 days 14 days 10-14 days — 7 days Healing of duodenal ulcer — — 4 weeks 4-8 weeks — 4 weeks Healing of gastric ulcer — — 8 weeks 4-8 weeks — — Prevention of NSAIDinduced ulcer — Up to 6 months 8-12 weeks — — — Treatment of dyspepsia — 2 weeks 2 weeks 2 weeks — — Treatment of erosive esophagitis 8 weeks 8 weeks 8 weeks 4-8 weeks 8 weeks 4-8 weeks Treatment of GERD 4 weeks 4-8 weeks 8 weeks 4-8 weeks — 4 weeks Treatment of pyrosis 4 weeks 2 weeks 2 weeks 2 weeks — — — Indefinite Indefinite Indefinite Indefinite Indefinite Treatment of ZES Abbreviations: GERD, gastroesophageal reflux disease; NSAID, nonsteroidal anti-inflammatory drug; ZES, Zollinger-Ellison Syndrome Strong evidence supporting the efficacy and mild side effect profile of PPIs may have contributed to their over-prescription and over-utilization.3 Recent literature suggests that long-term PPI use may be associated with a variety of adverse events, including infections, community-acquired pneumonia, increased risk of bone fractures, nutritional deficiencies, chronic kidney disease, and dementia.3,10-12 The FDA issued a safety announcement in 2012 regarding the association of PPI therapy with associated diarrhea. This included the recommendation that patients should immediately contact their healthcare providers and seek medical care should they develop diarrhea that does not improve while on PPI therapy.13 Additionally, a meta-analysis of 39 observational studies published in 2012 showed a 74% higher risk of developing a infection (CDI) in individuals that were on PPI therapy versus those that were not. A pooled analysis of three studies within the same meta-analysis evaluating recurrent CDI showed a 2.5-fold increase of recurrent CDI associated with PPI use.14 Guidelines from the American College of Gastroenterology published in 2013 recommend using PPIs with caution in patients at high risk for CDI.15 Additionally, the 2015 Beers Criteria strongly recommend, based on a high level of evidence, avoiding long-term PPI therapy in the geriatric population due to an increased risk of CDI.16 Enhanced bacterial colonization in the gastrointestinal tract due to decreased gastric acidity with the use of PPI therapy may explain this increased risk of enteric infections.2 Pharmacists should closely monitor high risk patients (e.g., geriatric, multiple antibiotics, long-term antibiotic use) for CDI if long-term PPI therapy is warranted. Similar to the mechanism previously mentioned for CDI, increased bacterial colonization in the stomach from decreased gastric acidity may also lead to an increased risk of pneumonia with PPI use.17 A systemic review and meta-analysis conducted by Lambert et al. in 2015 examined the association between outpatient PPI therapy and the risk of community-acquired pneumonia (CAP) in adults. This pooled analysis of 26 observational studies and randomized controlled trials showed a 49% increased risk of CAP with PPI therapy, with the highest risk during the first month of therapy, regardless of dose or patient age. The authors concluded that healthcare providers should consider this risk for CAP when initiating PPI therapy, especially when alternative regimens may be utilized.18 PPI therapy has also been linked to reduced intestinal calcium absorption, resulting in decreased bone density and increased fracture risk.17 Based on the results from several epidemiological studies, the FDA issued a safety alert in 2010 regarding the potential for increased risk of fractures of the hip, wrist, and spine with PPI use.19 In 2015, Zhou et al. published an updated meta-analysis of observational studies showing that PPI use was associated with a modestly increased risk of hip, spine, and any-site fracture. Pursuant to inconsistent results from previous studies investigating this risk, this meta-analysis evaluated 18 studies and found a 26% increased risk of hip fractures with PPI versus no PPI use. In addition, there was a 58% increased risk of spine fracture and a 33% increased risk of any-site fracture in PPI users. Furthermore, increased risk of hip fracture was associated with both short-term PPI use (less than 1 year) and long-term use (more than 1 year).20 The 2015 Beers Criteria strongly recommend, based on a high level of evidence, avoiding long-term PPI therapy in the geriatric population due to an increased risk of bone loss and fractures.16 Based on the proposed mechanism of decreased bone density with long-term PPI use, calcium supplementation may be appropriate for some patients. The use of calcium citrate is preferred with PPI therapy because its absorption is not dependent on an acidic environment.21 Some nutritional deficiencies are thought to be associated with long-term PPI use. One potential nutritional deficiency is hypomagnesemia. Although the exact mechanism of this deficiency is unclear, it has been hypothesized that decreased gastrointestinal absorption of magnesium due to PPI therapy may be the cause. Clinical research shows that this deficiency is not due to renal magnesium wasting, as was previously hypothesized.22 In 2011, the FDA released a warning about the risk of low magnesium levels with long-term PPI use. The FDA recommended that healthcare professionals consider drawing serum magnesium levels prior to starting a patient on PPI therapy for patients that are expected to be taking these drugs for an extended period of time or for patients that are taking other medications that may lower magnesium. Healthcare professionals should also consider periodic monitoring of magnesium levels in these patients.23 Patients who present with clinically significant hypomagnesemia may require discontinuation of PPI therapy, magnesium replacement, and/or treatment with an alternative class of medications such as a histamine-2 receptor antagonist.21 Vitamin B12 deficiency is another side effect sometimes seen with acid-suppressive therapy. Gastric acid is needed for the dissociation of vitamin B12 from other proteins. Thus, reducing the amount of available gastric acid through the use of PPIs can lead to a decrease in the dissociation and ultimate absorption of Vitamin B12.22 Currently, there are limited and conflicting data regarding the long term effects of PPI use and vitamin B12 deficiency.24 Some population evidence suggests that long-term PPI therapy is associated with vitamin B12 deficiency while other research does not support this link.25 Despite these inconsistent results, healthcare providers should monitor the elderly population for vitamin B12 deficiency while on long-term PPI therapy. It is also hypothesized that PPI use can lead to a decrease in iron absorption. The mechanism for malabsorption of iron is similar to that of vitamin B12, in which the decrease in gastric acid leads to a decrease in the dissociation of iron salts from food. Again, there are not robust data available to confirm that PPI therapy directly causes iron deficiency, but effects may be seen in patients previously suffering from iron deficiency.24 Pharmacists should be aware that long-term PPI therapy decreases iron absorption in patients with increased iron demands but should not routinely monitor all patients receiving PPI therapy for this side effect. Kidney disease is a newer concern associated with PPI use. PPI therapy causes interstitial nephritis, which is a cause of acute kidney damage.10 This acute kidney damage, coupled with the potential for hypomagnesemia, can lead to an increased risk of chronic kidney damage with PPI use. A 2016 study by Lazarus et al. shows that, after adjusting for potential confounders, use of PPIs is independently associated with a 20% – 50% higher risk of incident chronic kidney disease. This same study showed that the risk for chronic kidney disease was lacking in patients prescribed histamine-2 receptor antagonists, suggesting that the increased risk for chronic kidney disease is specifically associated with PPI use and not all acid-suppressive therapy.11 Additional research on the association between PPI use and chronic kidney disease is warranted. Another new concern with long-term PPI use is the development of dementia. Potential mechanisms for dementia development include vitamin B12 deficiency, which has been associated with cognitive decline, and the possible enhancement of amyloid beta peptide levels in the brain. A recent study by Gomm et al. suggests that long-term PPI use is associated with a 44% increased risk of dementia in patients 75 years of age and older. This risk was highest in patients 75-79 years of age, and the risk of dementia appeared to decline with increasing age.12 More research evaluating the effect of long-term PPI therapy on cognitive function is needed. The wide-spread use of PPI therapy may be due to overutilization both in the inpatient and outpatient settings. In addition, failure to re-evaluate the need for therapy continuation and insufficient use of step-down therapy all contribute to the abundance of prescription and over-the-counter PPI therapy. Once considered a safe medication class, PPIs are being over-utilized for their gastric acid suppressing efficacy, and adverse effects associated with long-term PPI use are becoming more well-known.3 Overall, PPI therapy should be recommended at the lowest effective dose for the shortest indicated duration. Patients should be monitored for resolution of symptoms warranting PPI usage. Additionally, patients at risk for the PPI-associated side effects described in this article should be monitored and treated as necessary. Risks and benefits should be weighed when evaluating PPI therapy, and patients should be titrated off PPI therapy with other shorter-acting agents, such as histamine-2 receptor antagonists or antacids, when possible. 1. Rane PP, Guha S, Chatterjee S, Aparasu RR. Prevalence and predictors of non-evidence based proton pump inhibitor use among elderly nursing home residents in the US. . 2016; Article in press. 2. Imhann F, Bonder MJ, Vich vila A, et al. Proton pump inhibitors affect the gut microbiome. . 2016;65(5):740-8. 3. Heidelbaugh JJ, Kim AH, Chang R, Walker PC. Overutilization of proton-pump inhibitors: What the clinician needs to know. . 2012;5(4):219-32. 4. Dexilant (dexlansoprazole) package insert. Deerfield, IL: Takeda Pharmaceuticals America, Inc.; January 2016. 5. Nexium (esomeprazole) package insert. Wilmington, DE: AstraZeneca; January 2016. 6. Prevacid (lansoprazole) package insert. Deerfiled, IL: Takeda Pharmaceuticals Inc.; September 2012. 7. Prilosec (omeprazole) package insert. Wilmington, DE: AstraZeneca; February 2016. 8. Protonix (pantoprazole) package insert. Philadelphia, PA: Wyeth Pharmaceuticals, Inc.; December 2014. 9. Aciphex (rabeprazole) package insert. Woodcliff Lake, NJ: Eisai Inc.; April 2016. 10. Antoniou T, Macdonald EM, Hollands S, et al. Proton pump inhibitors and the risk of acute kidney injury in older patients: a population-based cohort study. . 2015;3(2):E166-71. 11. Lazarus B, Chen Y, Wilson FP, et al. Proton pump inhibitor use and the risk of chronic kidney disease. . 2016;176(2):238-46. 12. Gomm W, von Holt K, Thome F, et al. Association of proton pump in inhibitors with risk of dementia: A pharmacoepidemiological claims data analysis. . 2016;73(4):410-6. References continued. 13. FDA Drug Safety Communication: associated diarrhea can be associated with stomach acid drugs known as proton pump inhibitors (PPIs). U.S. Food and Drug Administration Web site. 2012. http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm213259.htm. Accessed April 30, 2016. 14. Kwok CS, Arthur AK, Anibueze CI, Singh S, Cavallazzi R, Loke YK. Risk of infection with acid suppressing drugs and antibiotics: Meta-analysis. . 2012;107(7):1011-9. 15. Surawicz CM, Brandt LJ, Binion DG, et al. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. 2013;108(4):478-98. 16. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 updated Beers criteria for potentially inappropriate medication use in older adults. 2015;63(11):2227-46. 17. Shoenfeld AJ, Grady D. Adverse effects associated with proton pump inhibitors. . 2016;176(2):172-4. 18. Lambert AA, Lam JO, Paik JJ, Ugarte-gil C, Drummond MB, Crowell TA. Risk of community-acquired pneumonia with outpatient proton-pump inhibitor therapy: A systematic review and meta-analysis. . 2015;10(6):e0128004. 19. FDA Drug Safety Communication: Possible increased risk of fractures of the hip, wrist, and spine with the use of proton pump inhibitors. U.S. Food and Drug Administration Web site. 2010. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm213206.htm. Accessed April 30, 2016. 20. Zhou B, Huang Y, Li H, et al. Proton-pump inhibitors and risk of fractures: An update meta-analysis. . 2016;27:339-47. 21. O’Neill LW, Culpepper BL, Galdo JA. Long-term consequences of chronic proton pump inhibitor use. 2013;38(12):38-42. 22. William JH, Danziger J. Proton-pump inhibitor-induced hypomagnesemia: Current research and proposed mechanisms. . 2016;5(2):152-7. 23. FDA Drug Safety Communication: Low magnesium levels can be associated with long-term use. U.S. Food and Drug Administration Web site. 2011. http://www.fda.gov.cuhsl.creighton.edu/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm24 5275.htm. Accessed April 28, 2016. 2009 Mar;104(Suppl 2):S5-9. 24. McColl K. Effect of proton pump inhibitors on vitamins and iron. 25. Ito T, Jensen RT. Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of 2010;12(6):448-57. calcium, vitamin B12, iron, and magnesium. http://creighton.edu/pharmerica