Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
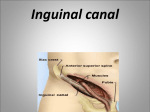
Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Tutors: The PBL case is Gabi and boyfriend. It covers sexual differentiation, male genital development, scrotal and testicular anatomy and function Issues relating to intimate examination are included in this session We will not be covering examination of the hernia orifices in the session, the examination of hernia is included in the SDL section in preparation for T year and clinical attachments. The students can view the video “Examination of the groin, the hernial orifices and the male external genitalia” in their own time. The aim of this session is to encourage a sensitive, thorough and systematic male genital examination. Please try and ensure that the students take this situation seriously. In the practical part of the session we will be practising the male external genital examination, only using a volunteer where appropriate and the manikins for the majority of the examination. Lesson plan 13.30-13.35 (5 mins) 13.35-13.45 (10 mins) 13.45-14.05 (20 mins) 14.05-14.55 (50 mins) 14.55-15.00 (5 mins) Introductions (Relevance, Aims and overview of the session). Sign registers Discuss the principles of intimate examination and issues related to intimate examinations as per your hand out; Please emphasise the importance of informed consent, privacy, respect for patient’s wishes and dignity chaperones supervision for this procedure as a medical student continued communication skills during the examination Run through the examination of the male external genitalia and scrotum on a manikin, using the 4 stage teach. Then go straight onto stage 4 – students perform while they describe the steps (you may need to prompt). During the examination: o The volunteer patient should be standing up for the general inspection, skin and major joints part of the examination o At the point of asking the patient to expose the genital area, hold the manikin in front of the volunteer for the inspection of the groin and scrotal region, and scrotal palpation whilst standing up. o Then place the manikin in a lying down position for the rest of the examination. o Try to get some feedback from the volunteer patient. Split your group. Half the group to practice the full examination on pelvic models. The other half of the group to practice the full scrotal examination on scrotal models. Then swap after 25 min. Use any free cubicles if you wish. Students should practice the introduction and preparation every time. Please give individual constructive feedback to the students. Closure. Encourage the students to practice in the SDL room and watch the video available on Moodle. ‘Examination of the groin, the hernia orifices and the male external genitalia.’ They should read the ‘self directed learning’ in their notes. 15.30-15.35 (5 mins) 15.35-15.45 (10 mins) 15.45-16.05 (20 mins) 16.05-16.55 (50 mins) 16.55-17.00 (5 mins) Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Learning Outcomes In this session you will Perform an examination of the male genitalia on a manikin. Consider issues highlighted by the intimate nature of genital examination, including consent, privacy, chaperones and respect for patient’s wishes and dignity Clinical relevance Male genital examination is an important skill. Unfortunately many doctors find it challenging. It may be indicated in children (especially to assess for descent of the testes, and occasionally for urethral abnormalities), adolescents (to assess for stage of sexual maturity) and in adults (e.g.to look for signs of STI’s (sexually transmitted infections) and other infections, skin problems, and to examine for abnormalities within the scrotum such as testicular cancer.) Links with other learning This session links with future and previous sessions; The principles of examining a lump Male catheterisation (T-year) Abdominal and rectal examination Other intimate examinations – rectal, breast, gynaecological examination Related Basic Sciences - Essential anatomy To help you during this session you should understand and revise the anatomy of the following structures: Penis, prepuce (foreskin) and the scrotal contents. Spermatic cord Inguinal lymph nodes. Anterior abdominal wall, inguinal ligament and femoral canal, Direct and indirect inguinal hernias and femoral hernias The anatomy of hernias is important, and you should learn this carefully alongside a clinical skills text and clinical textbooks. Moodle There is a DVD on Moodle – ‘Examination of the groin, the hernia orifices and the male external genitalia’ which will be useful for you to watch but the content and steps are different to what you will be learning today. Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Principles of an intimate examination This is an intimate examination. Please read the GMC guidance on intimate examinations and chaperones (http://www.gmcuk.org/static/documents/content/Intimate_examinations_and_chaperones.pdf) Please note the following in relation to this intimate examination; When carrying out an intimate examination such as this, it is particularly important to use excellent communication skills to explain the examination/procedure carefully and obtain informed consent. Physical contact with the patient should be kept to a minimum and all contact should be explained to the patient as you go along. Example: “I am just looking around the base of your penis for any warts or skin rashes, and now I am looking at the skin of the shaft. I’m pulling back the foreskin to have a look around the head of the penis”You must respect the patient’s dignity and keep the exposure of them to a minimum. Professional boundaries must be kept both in terms of the way that you perform the examination/procedure and your verbal and nonverbal communication In all intimate examinations you must make it clear to the patient that they will be examined again by your clinical supervisor. This will be the case for most examinations, but is particularly important for intimate examinations as patients may well be uncomfortable and anxious. General notes In clinical practice an examination of the scrotum and male genitalia is carried out after you have gathered information about the patient, the context is usually clearer after the history has been taken. It may form part of a more comprehensive examination. The groin, hernial orifices, scrotum and genitalia may be examined all together or separately. There is a degree of overlap. Often these examinations are performed after an abdominal examination. When examining the scrotum and genitalia you will need to examine the groin and at least inspect the lower abdomen. Following your examination of the scrotum and genitalia it may be necessary (depending on the context and your findings) to perform other examinations as well e.g. the hernial orifices, abdomen, perineum and rectum. Some clinicians will initially examine the patient standing up and some clinicians will initially examine the patient lying down and then stand them up. We will position the patient standing initially - this is because hernia swellings may be more obvious when standing, and varicoceles are rarely palpable when lying flat. It is important to also examine the scrotum. A large indirect hernia can descend into it, and varicoceles originating in the spermatic cord may present with scrotal signs and scrotal pathology may drain to the inguinal lymph nodes. Depending on the your clinical findings it may be necessary to perform other examinations as well. Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan In this examination it is important to explain to the patient what you will be examining and the exposure required. It is also important to be very gentle whilst palpating- note that the frenulum tends to be a particularly sensitive area. Occasionally an erection may develop and if it occurs it is important that the situation is dealt with appropriately. If this happens just explain to the patient in a matter of fact way that this sometimes happens and that you will take a short break from the examination, leaving the patient in private. STEPS Introduction and Preparation Introduce yourself by giving your full name and role Check the name of the patient Explain the nature and purpose of what you are going to be doing using non-technical language, and explain that your supervisor will also examine the patient afterwards. Explain how much exposure is necessary - the patient will need to be exposed from the umbilicus downwards. You also need to able to see the arms and legs if you are performing a genital examination. Attention to patient comfort and dignity is of paramount importance. Obtain consent Offer a chaperone Ask if the patient has any pain, and if so, to show you where it is. Ask the patient to report any pain or tenderness when you are examining them Gather equipment e.g. gloves, pen torch (for transillumination) Clean your hands and put on gloves Inspection with the patient standing Ask the patient to stand up General inspection Does the patient look well? Does he look in pain? Look at his skin – any signs of skin disease which may explain a genital rash e.g. excoriations of scabies, keratoderma blennorrhagica Look at the joints for any signs of inflammation which may be associated with genital conditions e.g. gonorrhoea, reactive arthritis Look at his eyes for any signs of conjunctivitis or uveitis Explain the need to expose the lower abdomen, groin and genital areas Lower abdomen and pubic area. o Look for erythema, swellings, lumps, ulcers, scars o Look for rashes, excoriations, infestations Inguinal and femoral region. o Ask the patient to take a deep breath and bear down – look for any visible swellings to enlarge or new swellings to appear. o Look for any signs of lymphadenopathy, scars Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Scrotum: gently move the scrotum to one side to inspect it thoroughly. Look for any obvious lumps or swellings Ask the patient to bear down and look specifically for a varicocele. Look for erythema, scars, ulcers, superficial lesions. Palpation with the patient standing Scrotum: palpate for a varicocele and ask the patient to bear down again – it may become more obvious. Palpate other lumps/swellings detected on inspection. A detailed examination is required (we will be covering the assessment of lumps in detail in another session) Inspection and palpation with the patient lying down Testes: Techniques vary. Isolate either testis by lifting gently away from the body. You can gently fix the testis toward the bottom of the scrotum with the thumb and first finger of your non-dominant hand. Palpate the entire surface of the testis. The surface should regular and smooth with no lumps or tenderness, and the consistency should be firm (NB: Consistency: Firm = similar to tip of nose, hard = similar to forehead, soft = similar to lip. This will be covered in more depth later). Check for mobility, the testes should lie free and not tethered to the skin or subcutaneous tissue. Note the testicular size for comparison. Epididymis: Palpate the head, body and tail of the epididymis over the superior/posterior aspect of the testes, feel for nodules, swellings or tenderness. Vas Deferens: Trace the Vas Deferens running up superiorly from the epididymis in the spermatic cord, rolling it gently between thumb and index finger. Assess the space above the testis for any mass e.g. an indirect hernia. If a lump /mass is found in the scrotum assess it further: Attempt to palpate above it. If you cannot get above it then the lump has not originated in the scrotum and might possibly be a hernia. If your fingers and thumb can meet above the swelling, then it is scrotal in origin. Does it have a cough impulse or bowel sounds? Is it separate to the testicle? Is it tender? Does it transilluminate? Is it only present on standing? Other features Examine the other testis, epididymis and vas deferens. A slight difference in testicular size is not uncommon. Penis: Inspect all aspects from base to tip. Look for evidence of hypospadias on the ventral aspect. Inspect the skin thoroughly for any ulcers, nodules, rash, masses, skin colour change etc. Foreskin (prepuce): If present explain that the foreskin needs to be drawn back. Some clinicians are more comfortable asking patients to withdraw and replace their own foreskin. Otherwise draw the foreskin back gently to examine the glans. Do not force it the foreskin will not retract if it is stenosed (phimosis). Urethral meatus: Note its position and look for any discharge. Frenulum: This should be present and intact. Corona: Inspect around the corona and look for warts, inflammation, rashes and ulcers. You may see pearly papules which are non pathological. Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Replace the foreskin to prevent a paraphimosis, whilst checking briefly to see if this produces any discharge. Penis: Opinions vary on the need to palpate the penis. For example a history suggestive of Peyronies disease (progressively worsening deviation of the penis on erection) or a malignant looking lesion would necessitate palpation. Some doctors advocate palpation as part of the examination and would palpate the two corpus cavernosum on the dorsal aspect and the urethra on the ventral aspect for any nodules and tenderness. Lymph nodes. Palpate the following areas for any lymphadenopathy with the flat of three fingertips starting away from any reported pain or lumps and then palpate systematically to locate the site of any swelling or lumps. Remember that these nodes drain a wide area of superficial structures. the region of the inguinal ligament inferior to the inguinal ligament upper medial aspect of the thigh. Femoral pulses – palpate in the approximate area of the mid inguinal points and auscultate for bruits. Additional examinations You may wish to consider examining the abdomen, hernial orifices, perineum, anus and rectum depending on the clinical context and your examination findings. Closure Remove your gloves Thank the patient and allow them to get dressed in privacy Ensure that they are comfortable and in a state of dignity Wash your hands Clean your pen torch/stethoscope (if used) Record/report findings Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan SUMMARY OF MALE GENITAL+SCROTAL EXAMINATION INTRODUCTION+PREPARATION Full name + role Check patients name Explain examination + that your supervisor will also examine the patient later Explain exposure necessary Obtain consent Offer a chaperone Ask about pain + to report any pain during the examination Gather equipment (eg. gloves, pen torch) Clean your hands and put on gloves STANDING: INSPECTION General inspection Wellbeing Pain Skin (excoriations of scabies, keratoderma blennorrhagica) Joints (inflammation which may be associated with genital conditions e.g. gonorrhoea, reactive arthritis Eyes (conjunctivitis/uveitis) Lower abdomen+ pubic area o Swellings, lumps, ulcers, scars o Erythema, rashes, excoriations, infestations Inguinal + femoral region o Bear down swellings o Lymphadenopathy o Scars Scrotum Lumps or swellings Bear down varicocele Skin abnormalities: erythema, scars, ulcers, superficial lesions. STANDING: PALPATION Scrotum o Varicocele (bear down) Lumps/swellings LYING DOWN: INSPECTION+PALPATION Testes: o Surface (smooth, regular) o Consistency (firm) o Mobility o Tenderness o Mobility Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan o Tethering to underlying skin or subcutaneous tissue o Size Epididymis: o Nodules, swellings or tenderness. Vas Deferens: o Assess space above testis for masses / indirect hernia. Lump/mass in scrotum: o Attempt to palpate above it. If you cannot get above it ?hernia. If you can get above it ?from scrotum o Cough impulse o Bowel sounds o Separate to testicle o Tenderness o Transilluminability o Only present on standing o Other features Examine the other testis, epididymis and vas deferens. Penis: o Inspect all aspects from base to tip o Hypospadias o Skin: ulcers, nodules, rash, masses, skin colour Foreskin: o Draw back o Phimosis Urethral meatus: o Position o Discharge. Frenulum Corona o Warts, inflammation, rashes and ulcers. Replace the foreskin. Penis: if indicated Lymph nodes o Inguinal ligament region o Inferior to inguinal ligament o Upper medial aspect of the thigh. Femoral pulses o Palpate o Auscultate for bruits. ADDITIONAL EXAMINATIONS Consider o Abdomen o hernial orifices o Perineum o Anus/rectum Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan CLOSURE Remove gloves Thank patient and allow them to get dressed in privacy Wash your hands Clean your pen torch/stethoscope (if used) Record/report findings Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Self-directed learning From T year onwards you will be examining patients with hernias and other pathology relating to the groin so it would be useful for you to prepare in advance. Note that this will be covered in Tyear, and you will not be asked to do a hernia examination this year. Examination of the groin and hernial orifices Hernia Please refer back to your anatomy preparation in relation to how the different types of hernia in the groin region present (we are not covering any other types of hernias in these notes). Consider what the following terms mean in relation to hernias – reducible, irreducible, obstructed, strangulated. Always seek urgent senior help if a hernia is significantly tender or there are other signs of obstruction/strangulation. The following is a discussion on inguinal and femoral hernias (not any other type). Note: An indirect inguinal hernia will enter the inguinal canal at the internal (deep) inguinal ring (just above the mid-inguinal point, half way between ASIS and symphysis pubis, approximately 1cm above the femoral pulse). If this hernia is reducible, a finger over the internal (deep) ring will prevent the hernia from reappearing. If an inguinal hernia protrudes through the external (superficial) ring, it can be felt to lie above and medial to the pubic tubercle. An indirect hernia may follow the spermatic cord all the way to the scrotum and present as a scrotal swelling. A direct inguinal hernia represents a bulging directly through the posterior wall of the inguinal canal, medially to the internal (deep) inguinal ring. Please note that direct and indirect hernias can be difficult to distinguish from each other clinically. The definite way to tell is through exploration during surgery. A femoral hernia will lead to a cough impulse and swelling over the femoral canal (below inguinal ligament, “below and lateral to the pubic tubercle”) A large indirect inguinal hernia may extend into the upper scrotum, and may be confused with a scrotal lump (see below) General notes This is an intimate examination (see notes above). You should start by carrying out a full abdominal examination. As well as examining the hernial orifices you should also examine the scrotum – this is because a large indirect hernia can descend into the scrotum, varicoceles originating in the spermatic cord may present with scrotal signs and scrotal pathology may drain to the inguinal lymph nodes. Introductions and Preparation Introduce yourself by giving your full name and role Check the name of the patient Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Explain the nature and purpose of what you are going to be doing using non-technical language and explain that your supervisor will also examine the patient afterwards Explain how much exposure is needed. Attention to patient dignity is of paramount importance. Offer a chaperone (see GMC guidance) Obtain consent Ask if the patient has any pain, and if so, to show you where it is. Ask the patient to report any tenderness when you are examining them Gather equipment e.g. gloves, pen torch (for transillumination) Clean your hands Start with the patient lying down Inspection with the patient lying down General inspection of the patient o Do they look unwell/in pain? o Are they vomiting/have been vomiting? Carry out a full abdominal examination. Put on gloves Now explain need for uncovering the groin and genital areas. Inspect the lower abdomen and pubic region for erythema, swellings, lumps, scars etc. Inguinal and femoral region o Look for any erythema, swellings, lumps, scars etc. o Ask the patient to take a deep breath and bear down/cough – look for any visible swellings to enlarge or new swellings to appear. Look to see if any herniasappear and/or spontaneously reduce Inspect the scrotum (you may need to gently move the scrotum to one side to inspect it thoroughly) o Look for skin abnormalities: erythema, swellings, lumps, ulcers, superficial lesions, scars etc. o Look for varicoceles – ask the patient to bear down/cough Palpation with the patient lying down Scrotum – palpate for a varicocele/s in the scrotum, ask the patient to bear down/cough again – it may become more obvious.Carry out a full scrotal examination (as in notes above). Cough impulse o If a hernia is suspected and the history confirms that it can be reduced by the patient, then ask the patient to reduce the hernia (if they can’t then your supervisor may do this). o Once it is reduced, place one finger over the internal (deep) ring (just above the midpoint of the inguinal ligament). Ask the patient to cough. If the hernia is an indirect hernia your finger will prevent the hernia from reappearing. If the hernia reappears it is more likely to be a direct hernia or a femoral hernia (2). In patients without an obvious swelling check for a cough impulse bilaterally over Internal (deep) inguinal ring (just above the mid inguinal point, 1-2cms above the femoral pulse) lateral to the inferior epigastric artery Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan External (superficial) inguinal ring (locate the position relative to the pubic tubercle and then palpate with the index finger from the upper aspect of the scrotum. Inguinal/Hasselbach’s triangle (use the flat of the hand placed medial to the site of the internal (deep) inguinal ring). The borders of the triangle are as follows: o Inferior aspect = inguinal ligament o Superior + lateral border = inferior epigastric vessels o Superior + medial border = lateral aspect of rectus sheath Femoral canal (inferior to the inguinal ligament and lateral to the pubic tubercle) Hernias will not transilluminate, and auscultation may reveal bowel sounds (if it is a large hernia that contains bowel). Seek urgent senior help if a hernia is tender or if there are other signs/symptoms of obstruction/strangulation. A large indirect inguinal hernia may extend into the upper scrotum, and may be confused with a scrotal lump (see below) Other lumps or swellings detected on inspection– a detailed examination is required (we will be covering the assessment of lumps in detail in another session) Lumps, swellings and lymph nodes - palpate the inguinal region (in the region of the inguinal ligament) with the flat of three fingertips starting away from any reported pain or lumps and then palpate systematically to locate the site of any swelling or lumps or lymph nodes. Also palpate inferior to the inguinal ligament and the upper medial aspect of the thigh. Remember that the lymph nodes in these areas drain a wide area of superficial structures. Femoral pulses – palpate in the approximate area of the mid inguinal points and auscultate for bruits. Ask the patient to stand up Stand to the side of the patient when you then examine them and move your head so it is at the same level as the part of their body you are examining. Inspection with the patient standing up Inspect the lower abdomen and pubic region for erythema, swellings, lumps, scars etc. Inguinal and femoral region o Look for any erythema, swellings, lumps, scars etc. o Ask the patient to take a deep breath and bear down/cough – look for any visible swellings to enlarge or new swellings to appear. Look to see if any hernias appear and/or spontaneously reduce Inspect the scrotum (you may need to gently move the scrotum to one side to inspect it thoroughly) o Look for erythema, swellings, lumps, ulcers, superficial lesions, scars etc. o Look for varicocele/s – ask the patient to bear down/cough Palpation with the patient standing up Scrotum – palpate for a varicocele/s in the scrotum, ask the patient to bear down/cough again – it may become more obvious. A large indirect inguinal hernia may extend into the upper scrotum, and may be confused with a scrotal lump. Carry out a full scrotal examination (as in notes above). Cough impulse– repeat these (as above) Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Other lumps or swellings detected on inspection– a detailed examination is required (we will be covering the assessment of lumps in detail in another session) Lumps, swellings and lymph nodes - palpate the inguinal region (in the region of the inguinal ligament) with the flat of three fingertips starting away from any reported pain or lumps and then palpate systematically to locate the site of any swelling or lumps or lymph nodes. Also palpate inferior to the inguinal ligament and the upper medial aspect of the thigh. Remember that the lymph nodes in these areas drain a wide area of superficial structures. Additional examinations You may wish to consider examining the external genitalia, scrotum, perineum, anus and rectum depending on the clinical context and your examination findings. Closure Remove your gloves Thank the patient, tell them that they can get dressed. Ensure that they are comfortable. Wash your hands Clean your pen torch/stethoscope (if used) Record/report findings ===================================================================== You may also find the following aspects of basic science useful in your understanding of normal scrotal contents and abnormal swellings. Embryology Essentially the testes develop high up on the posterior abdominal wall. It is necessary for the testes to leave the abdominal cavity since the temperature there retards the normal process of spermatogenesis. During fetal life the testes “descend” behind the peritoneum, dragging their blood supply, nerve supply and lymphatic drainage after them through the inguinal canal into the scrotum. Anatomy Inguinal canal This is an oblique passage through the lower part of the anterior abdominal wall. It is present in both sexes and lies parallel to and immediately above the inguinal ligament. It is 4cm long and passes downwards and medially, and from deep to superficial, from the internal (deep) to the external (superficial) inguinal rings. The inguinal ligament is attached laterally to the anterior superior spine (ASIS) and curves downwards and medially to be attached to the pubic tubercle, a small protuberance along the superior surface of the pubis. The internal (deep) inguinal ring is an opening in the fascia transversalis about 1-1.5cm above the mid point of the inguinal ligament, lateral to the inferior epigastric artery. The external (superficial) inguinal ring is a triangular aperture in the aponeurosis of the external oblique muscle situated above and lateral to the pubic tubercle. Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan A hernia is the protrusion of an organ through a defect in the wall of the cavity containing it, into an abnormal position. In the inguinal region there are inherent weaknesses in the abdominal wall which may result in herniation. There are different types of hernia in the region of the groin, however in the context of scrotal examination, it is a hernia known as an indirect hernia which may present itself as a scrotal swelling. This type of hernia emerges from the abdominal cavity through the internal (deep) ring, passes along the inguinal canal, and, if large enough, emerges through the external (superficial) ring from where it descends into the scrotum. Scrotum This is a pouch of skin containing the testes, the epididymides and lower ends of the spermatic cords The spermatic cord begins at the internal (deep) inguinal ring, emerges from the external (superficial) inguinal ring and descends into the scrotum ending at the testis. It contains many structures including vas deferens, testicular artery, testicular vein and lymph vessels. If the valves inside the testicular (spermatic) veins are defective or the venous drainage of the testicle is compressed, blood will be prevented from flowing properly, the blood will back up, leading to dilatation of the veins in the pampiniform plexus (1). This is called a varicocele - you may be able to feel a non-tender, twisted mass along the spermatic cord (it feels like a bag of worms). NB. There are other reasons why varicoceles may develop which are beyond the scope of this session. The testis is a firm ovoid body surrounded on its lateral, anterior and medial surfaces by the tunica vaginalis – a closed sac invaginated from behind by the testis. Efferent ductules connect the testes to the head of the epididymis, a coiled tube nearly 6m long. It lies posterior to the testis. The vas deferens, a thick walled muscular duct which transports spermatozoa from the epididymis to the urethra, emerges from the tail of the epididymis and ascends medially to enter the spermatic cord. The vas deferens can be palpated between the finger and thumb in the posterior aspect of the cord in the upper part of the scrotum. Penis This consists of a root, body and distal glans. The dorsal surface is located anteriorly, its ventral surface is in contact with the scrotum. The two corpus cavernosum lie dorsally and the urethra is situated ventrally. The base of the glans is encircled by the corona and foreskin attachment which extends onto the ventral aspect of the glans via the frenulum. The normal site of the external urethral meatus is at the tip of the glans. Hypospadias is a common abnormality, occurring as a result of incomplete fusion of the urethral groove producing a urethral meatus located in an aberrant location on the ventral surface of the penis. The meatus can be located anywhere along the ventral penile shaft from the meatus distally to the perineum proximally Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Inguinal lymph nodes There are two types of inguinal lymph nodes located below the inguinal ligament – superficial and deep. The superficial inguinal lymph nodes (about 10 in total) form a chain underneath the inguinal ligament between the borders of the sartorius muscle and the adductor longus muscle. These lymph nodes drain into the deep inguinal lymph nodes. The deep inguinal lymph nodes (between 3 and 5) are located deeply on the medial side of the femoral vein. Clinical reasoning Skin lesions and rashes will be covered elsewhere in the course. Some conditions and infections are more common in the genital area than others. Urethral discharge usually relates to infection (Chlamydia, Gonorrhoea and others) and warrants further investigation and management. An undescended testicle is at increased risk of malignant change (so always check that there are two), even once it has been surgically brought down to the scrotum (so a particularly careful examination is recommended in these patients, and it would be very relevant to ensure that they are able to examine themselves). Scrotal swellings /masses Scrotal masses can be categorized by the origin of the mass: Origin Testicle Testicle (with marked tenderness) Mass Malignancy Testicular torsion Testicular infection (Orchitis/ Features Nodules that you are not able to feel as separate from the testis are malignant until proven otherwise. May be tender or non-tender, overlying skin may be normal or erythematous. Remember that the lymphatic drainage of the testes is principally to the intra-abdominal paraaortic nodes. Occasionally small testicular lumps may represent old scarring or adherent epididymal cysts. An urgent ultrasound is essential A surgical emergency (leads to necrosis). Very tender, often a sudden onset, abdominal pain, nausea and vomiting, absent cremester reflex. Often red scrotal skin and elevated horizontal lie of the affected testis Tenderness, sometimes quite marked, often more insidious onset and may or may not be related to urinary symptoms. Always think torsion and be sure Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan epidimoorchitis) Various origins (Inability to feel testicle because of scrotal mass) Hydrocele Epididymal cysts Epididymis Epididymal thickening Varicocele Above the testis Indirect inguinal hernia you have excluded it. The testis may be embedded within a tense sack of fluid called a hydrocele, which may be congenital or acquired. Transillumination may help with this diagnosis, but an ultrasound is recommended to exclude testicular malignancy. These small cysts originate from either the anterior or posterior head of the epididymis. They are palpated as separate from the testis, and generally have very little clinical significance. A normal epididymis feels rather like a plastic bag between your fingers, thin, non-tender and slightly slippery. Tender thickening of the epididymis may represent active infection (“epididymitis”). Non-tender thickening may represent old infection or trauma. These classically feel like a “bag of worms” and tend to disappear on lying flat. Usually idiopathic and slow to develop. They are more common in men aged 15-25 and occur more commonly on the left. Always consider secondary causes of varicoceles e.g. a renal tumour, a retroperitoneal tumour – you should read about the clinical presentation of these varicoceles. Varicoceles are often the cause of infertility in men. Usually reducible (unless incarcerated), can’t get above it (originates in abdomen), may have bowel sounds, likely to have a cough impulse unless strangulated. If any features of strangulation, then urgent review required. Skill: Male genital and scrotal examination MBBS4 Year 1: Tutor Notes 2015-16. Lead Lecturer: Dr Hamed Khan Further Reading & References STD’s: Adler, M. W. (2004). ABC of sexually transmitted infections. London, BMJ Books. Wisdom, A. (1989). A colour atlas of sexually transmitted diseases, Wolfe. Surgery Ellis H, Calne R, Watson C (2006) Lecture Notes General Surgery 11th Edition, Blackwell, Oxford. McLatchie G, Borley N, Chikwe J (ed) (2007) Oxford Handbook of Clinical Surgery 3rd Edition, Oxford University Press, Oxford Chaperones & Consent for intimate examination GMC guidance on intimate examinations and chaerones http://www.gmcuk.org/static/documents/content/Intimate_examinations_and_chaperones.pdf Coldicott, Y., Pope, C., Roberts, C., Nesheim, B.-I. & Macdougall, J. 2003. The ethics of intimate examinations---teaching tomorrow's doctors * Commentary: Respecting the patient's integrity is the key * Commentary: Teaching pelvic examination---putting the patient first. BMJ, 326, 97-101. Stott, D. 2008. Chaperones for intimate examinations. Student BMJ, 16. Other references 1. Varicocele. Department of Urology James Buchanan Brady Foundation available athttps://www.cornellurology.com/clinical-conditions/male-infertility/generalinformation/varicocele/ [Accessed 30/7/2013] 2. Palpation of the hernia available at http://www.gpnotebook.co.uk/simplepage.cfm?ID=731512836&linkID=9797&cook=yes [Accessed 30/7/2013] Acknowledgements This resource was adapted from a skills sheet “The systematic male genital examination” by Dr. Dason Evans, and the MBBS4 skills sheet “Principles of intimate examination Scrotal and male genital examination” by Deborah Horton and ‘Examination of the groin, the hernia orifices and the male external genitalia’ by Scarpa Shoeman and the DVD “Examination of the groin, the hernial orifices and the male external genitalia” by Scarpa Schoeman. With thanks to Dr. Laura Tincknell for reviewing the hernia examination part of the notes.