Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
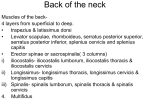
Client Supine: suprahyoid group. The client is supine; you are seated at the head of the table. To palpate the infrahyoids, place 1. 2. Sternocleidomastoid (SCM): The client is supine with your palpating fingers immediately inferior to the hyoid the head and neck contralaterally rotated; you are seated bone and just off center and feel for their contraction as at the head of the table. Before palpating, first visualize the the client is resisted from depressing the mandible at the contraction of the SCM as the client lifts the head from the temporomandibular joints (TM)s). Once felt, palpate these table. Then palpate the contraction of the SCM just supe- muscles toward their inferior attachments on the sternum rior to the sternoclavicular joint as the client again lifts the by strumming perpendicular to the fibers as the client head from the table. Once felt, continue palpating the SCM alternately contracts and relaxes them. The inferior belly to the mastoid process of the temporal bone and the supe- of the omohyoid can be palpated in the posterior triangle rior nuchal line of the occipital bone by strumming per- of the neck by strumming perpendicular to it as the cli - pendicular to the fibers as the client alternately contracts ent is resisted from depressing the mandible at the TMJs . and relaxes the muscle. Note: Look and palpate carefully To palpate the suprahyoids, place your palpating fingers for the clavicular head; it is usually less obvious than the immediately inferior to the mandible and again feel for sternal head. their contraction as the client is resisted from depressing Scalene group: The client is supine; you are seated at the the mandible at the TMJs. Once felt, palpate these muscles head of the table. Locate the lateral border of the clavicu - toward the hyoid bone by strumming perpendicular to the lar head of the SCM (be sure that it is the lateral border fibers as the client alternately contracts and relaxes them. of the clavicular head, not the sternal head that you have Palpate the stylohyoid and superior belly of the digastric located). Place palpating fingers just lateral to the lateral by strumming perpendicular to their fibers from the hyoid border of the clavicular head of the SCM and just superior bone toward the mastoid process of the temporal bone as to the clavicle, and feel for the contraction of the scalenes the client alternately contracts and relaxes them. as the client takes in short, quick breaths through the nose. Once felt, palpate as much of the scalenes as possible in the posterior triangle of the neck by strumming perpen- Client Seated: dicular to the fibers. The transverse processes attachment of the scalenes can usually be palpated by pressing in deep to the SCM if it is first slackened by passively flexing and 5. neck contralaterally rotated; you are standing to the side of ipsilaterally laterally flexing the client's head and neck. the client. Feel for the contraction of the upper trapezius Note: It can be challenging to discern the anterior, middle, at the top of the shoulder as the client is resisted from and posterior scalenes from each other. The best way to extending the head and neck against the resistance of your achieve this is to try to feel for the different direction of support hand on the back of their head (Note: The contrac- fibers that each one has. Remember: the anterior scalene tion of the upper trapezius is often visible and palpable; be goes to C3-C6; the middle scalene goes to C2-C7; and the sure to look for it as well). Continue palpating the upper posterior scalene goes to C5-C7. Also, keep in mind that trapezius toward its medial attachment on the head and the posterior scalene is located in the posterior triangle of neck and its lateral attachment on the lateral clavicle and the neck immediately anterior to the upper trapezius and acromion process by strumming perpendicular to its fibers levator scapulae. 3. as the client alternately contracts and relaxes it. Note: The Longus colli/longus capitis: The client is supine; you are superior aspect of the upper trapezius is actually quite seated at the head of the table. Locate the medial border narrow and only attaches to the medial V 3 of the superior of the sternal head of the SCM, and then drop off it and place palpating fingers immediately medial to that. Sink in toward the anterior surface of the vertebral bodies slowly and gently, but firmly. If you feel a pulse under your fingers, move your fingers to one side or the other and continue palpating for the vertebral bodies. Once you have reached the vertebral bodies, confirm that you are on the longus colli by asking the client to flex the head and neck by lifting the head up off the table. Palpate as much of the longus colli and capitis as possible superiorly and inferiorly by strumming perpendicular to the fibers. Note: The carotid tubercle on the transverse process of C6 (see page 100) is a good landmark for determining the segmental level of the palpating fingers. 4. Hyoid group: For the purpose of palpation, the hyoid group can be divided into the infrahyoid group and the Upper trapezius: The client is seated with the head and nuchal line of the occipital bone. 6. Levator scapulae: Note: The palpation of the levator scapulae can be divided into three parts: when it is deep to the upper trapezius near its scapular attachment, when it is superficial in the posterior triangle of the neck, and when it is deep to the SCM near its spinal attachment. The client is seated with the hand in the small of the back; you are standing behind or to the side of the client. Locate the superior angle of the scapula and place your palpating hand immediately superior and medial to it. Feel for the contraction of the levator scapulae deep to the upper trapezius as the client performs a gentle, short range of motion of elevation of the scapula at the scapulocostal joint. Once felt, continue palpating it until it enters the posterior triangle of the neck (i.e., until it is no longer deep to the upper trapezius) by strumming perpendicular to its fibers as the client alternately gently contracts and relaxes the muscle. Once the levator scapulae that the upper trapezius is relaxed and slackened; it can be is located in the posterior triangle, it is superficial and eas - slackened by passively moving the client's head and neck ily palpable, and sometimes visible as well. It is no longer into extension, contralateral rotation, and/or ipsilateral necessary for the client to have the hand in the small of the lateral flexion. back, and the client can be asked to perform a more forceful contraction (against resistance if desired) of elevation of the scapula. Continue palpating it superiorly by strumming per- Client Supine: pendicular to its fibers as the client alternately con tracts and relaxes the muscle. As it approaches its spinal attachment 8. in the small of the back, and/or the head and neck rotated deep to the SCM. To palpate it all the way to its spinal at- to the same side (ipsilaterally rotated); you are seated at tachments deep to the SCM, the SCM must be slackened by the head of the table. Ask the client to extend the head and passively moving the client's head and neck into flexion and neck at the spinal joints by gently pressing the head into ipsilateral lateral flexion. Note: When following the levator the table and feel for the contraction of the semispinalis scapulae superiorly, be sure that you follow it toward the capitis deep to the upper trapezius, just below the occiput transverse process of Cl, which is located more anteriorly and just lateral to the spine. Once felt, continue palpating than most people realize; the transverse process of Cl is the semispinalis capitis inferiorly as far as possible as the located immediately inferior to the ear. 7. Semispinalis capitis: The client is supine with the hand (transverse processes of C1-C4), the levator scapulae will go Splenius capitis: The client is seated with the head and client alternately contracts and relaxes the muscle. 9. Suboccipital group (rectus capitis posterior major neck ipsilaterally rotated; you are standing behind the [RCPMaj], rectus capitis posterior minor [RCPMin], client. Palpate in the uppermost aspect of the posterior tri - obliquus capitis inferior [OCI], obliquus capitis supe- angle of the neck, just inferior to the occiput and posterior rior [OCS]) : The client is supine; you are seated at the head to the SCM. Now feel for the contraction of the splenius of the table. Begin by palpating the RCPMaj; palpate just su- capitis as the client is resisted from extending the head and perior and slightly lateral to the spinous process of C2 and neck at the spinal joints. Once felt, strum perpendicular to strum perpendicular to it fibers. Once felt, continue palpat- its fibers and try to follow it inferiorly as the client alter- ing the RCPMaj to the occiput by strumming perpendicular nately contracts and relaxes the muscle. Once you are no to its fibers. Palpate the RCPMin in the same manner by longer in the posterior triangle of the neck, the splenius strumming perpendicular to it, beginning just superolateral capitis can be palpated two ways: (1) feel for it through to the posterior tubercle of Cl. Once felt, continue palpat- the upper trapezius by asking the client to extend the head ing the RCPMin to the occiput by strumming perpendicular and neck against gentle resistance; once felt, try to follow it to it. To palpate the OCI, palpate between the spinous as far inferiorly as possible; or (2) feel for it directly: this process of C2 and the transverse process of Cl, strumming requires you to palpate deep (anterior) to the border of perpendicular to the fibers. It may be helpful to have the the upper trapezius and press anteriorly toward the upper OCI contract by gently resisting the client from ipsilaterall y thoracic spinous processes by reaching with your palpating rotating the head. The OCS is extremely challenging to pal - fingers between the upper trapezius and the splenius capi - pate and discern from adjacent musculature. To attempt its tis. To accomplish this, it is best to stand more to the front palpation, feel for it just lateral to the superior attachment of the client so that your finger pads are oriented anterio rly of the RCPMaj; if felt, try to continue palpating it inferiorly toward the splenius capitis. Furthermore, it is important by strumming perpendicular to it.