Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
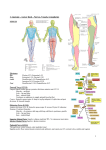
Hip Approach Indication Position Anterior (Smith Petersen) THR Washout of septic hip Open reduction of congential hip dislocation Supine Anterolateral (Watson jones) THR/hemi ORIF NOFs Lateral Direct Lateral (Hardgine) THR Lateral Posterior (Southern) THR/Hemi Dependent drainage of septic hip Lateral Internervous/Inter muscular plane Superficial: Sartorius (femoral) TFL (Sup glut) Incision Superficial dissection Deep dissection Dangers From anterior iliac crest to ASIS Curve inferiorly towards patella for 8-10cm Incise fascia on medial TFL + develop plane Care to avoid lat cut N Ligate ascending branch of lat fem circum artery Identify plane b/w RF _ glut med RF medially Glut med laterally Adduct + ex rot leg T capsulotomy Lateral femoral cut N Femoral nerve Ascending branch of lat fem circumflex artery Curved from 2.5cm post + distal to ASIS incision 10cm centred on post 1/3 GT In line with incision Incise fascia in line w/ fibres Retract Glut med posteriorly Retract TFL anteriorly Release origin of vastus lateralis + retract inferiorly T shaped capsulotomy Intermuscular Split Glut med Split Vastus lateralis Straight centred on GT 5cm above + 8 cm below Split fascia lata + retract anteriorly Detach glut med fibres Intermuscular Glut max split Start 7cm above + post to GT 10-15cm curved 1 inch posterior to GT Incise fasic lata + uncover vastus lateralis Split glut max Split glut med from middle GT 3-5cm Extend through vastus lateralis + take with glut min as anterior flap T capsulotomy Internally rot leg to stretch external rotators Detach Piriformis + obturator internus + reflect back T capsulotomy Femoral N – risk of compression/damaged by retractors in iliopsoas Femoral A+V – damaged by retractors in iliopsoas Abductor limp – disruption of abductor mechanism Femoral shaft # Sup glut N – runs b/w glut med + min 3-5cm superior GT Femoral N – risk of compression Deep: Rectus femoris (Femoral) Glut med (Sup glut) Intermuscular TFL + glut med (sup glut N) Sciatic N – extend hip + knee Inf Glut A 1st perforator of prof. femoris Femoral vessels Sup glut A + N Quadratus femoris Heterotropic ossification Medial Open reduction congenital dislocation Supine + leg flexed, abducted + externally rotated Superficial intermuscular: Add longus + gracilis (Obturator) Deep internervous: Add brevis (Ob) + magnus (sciatic) 3cm below pubic tubercle Longitudinal in line with adductor longus Develop plane b/w gracilis and add longus Develop plane b/w add brevis + magnus Med fem circumplex A Obturator N Deep external pudendal A