Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
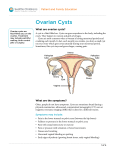
Gynaecological cancers Mr Vivek Nama MD MRCOG Consultant Gynaecological Oncologist Gynaecological cancers Why do we need 2 week wait ? Early/timely diagnosis of cancer Possibly less invasive treatment and better QoL Avoid emergency admissions Planned delivery of care Higher standards and job worthwhile Fewer dissatisfactions, complaints and risk of litigation 16 % of claims at MPS are delayed diagnosis Assessment and examination of patient Challenges Shift from being always right to being safe Low diagnostic yield rates – increase referral – inability of services to cope with it Multiple providers resulting in a complex diagnostic/therapeutic pathway CUH USC performance 20 per week. (Nov 16 to Feb 2017) 62 day treatment – 3 breeches (One each month) Reasons for delays – medical reasons for diagnostic delays, patient choice, other Ovarian Cancer: Ovarian cancer 7029 case in 2012 in the UK and Life time risk 1: 51 Relative 5 year survival rates – 34 %, lower than European average, But stage 1, survival rates of 90 % achieved Not a silent killer, symptoms present No effective screening test – UKCTOCS trial, PLCO trial, ROcKets ongoing Screening history- ovarian cancer – BRCA – Genetic tree Ovarian cancer detection in Primary care Women presenting with symptoms to GP Examination shows ascites and/or mass (exc. Fibroids) refer urgently. Perform CA 125 and USS. any woman of 50 or over who has experienced symptoms within the last 12 months that suggest irritable bowel syndrome (IBS) OR if symptoms are concerning for ovarian cancer but no physical features – Based on Symptom Index Perform serum CA 125 Unexplained weight loss, Fatigue, Change in bowel habits Perform CA125 Raised CA125 & Normal Examination USC Arrange USS USS Abnormal Refer USS Normal Repeat CA125 in few weeks Refer? RMI Repeat CA125 > 200 Discuss at RMH < 200 Operate at CUH Decreasing Increasing CT Scan Discharge Abnormal Normal Lap and Biopsy Risk of Malignancy index CA 125 levels in U/ml × menopausal score × ultrasound score Ultrasound features: Multi-loccular cyst Evidence of solid areas Evidence of metastasis Presence of ascites Bilateral lesions 0 – none, 1 – one abnormal feature, 3 – 2 or more abn. Menopausal score – pre – 1 , post -3 Sensitivity – 78 %, specificity 87 % Problem with tests - CA 125 and USS CA 125 also elevated in fibroids medical liver problems such as heart failure disease and other cancers Endometriosis Ovarian masses in pre-menopausal group IOTA – International Ovarian Tumour Analysis Group M-features and B-features Reported sensitivity 95 % and specificity 91 % M-rules •Irregular solid mass with irregular B-rules component 80 % of the tumour •Unilocular cysts •Presence of ascites •Solid components <7 mm •At least 4 papillary structures with •Presence of acoustic shadowing a height >= 3mm •Smooth multilocular tumour with a •Irregular multi-locular solid tumour •largest diameter <100mm with a max diameter > 10cm •No blood flow •Strong vascularity Case Scenario Clinical assessment 70 y old with persistent bloating and abdominal pain Abdominal and pelvic examination – no masses/ascites Normal CA125 USS Normal CA125 with Symptoms Difficult to convince patients Return if Symptoms Persist Consider Evaluation for Bowel Cancer OVA1 and HE4 Ovarian Cysts with normal CA125 Post-menopausal ovarian masses Cysts 2-5 cms, unilateral, unilocular and echo-free with no solid parts or papillary formations Risk of malignancy is less than 1%. In addition, more than 50% of these cysts will resolve spontaneously within three months. Thus, it is reasonable to manage cysts of 2–5 cm conservatively. 4 monthly scan and CA 125 x one year, no change discharge. Other options Lap SO Pre-menopausal cyst The following cysts should be treated as simple cysts: Ovarian/para-ovarian cyst, cysts containing daughter cysts Cysts with one thin septation (<3mm, with no vascularity) Cysts with small calcification in wall. If there is an obvious area of calcification; consider whether this may be a dermoid cyst. Cyst criteria apply even if cysts are multiple (cysts completely separate from each other) or bilateral. Pre-menopausal cyst - management Less than 5cm No follow up required unless there is clinical concern. Findings are likely to be physiological in nature and almost always resolve within 3 menstrual cycles. Pre-menopausal cyst - management 5 - 7cm - Suggest rescanning in four months. If smaller or resolved no further follow up required. If larger or persisting suggest further gynaecological review. Ovarian cysts that persist or increase in size are unlikely to be functional and may warrant surgical management. If symptomatic, for benign gynaecological review. > 7 cm – suggest benign gynaecological team review with a view to surgical removal. Summary Ovarian cancer management is multi-modal CA 125 and TV US scan Move to increase surgical efforts Vs quality of life Cervical cancer – fertility preservation HPV vaccination 2 WW Referral criteria - PMB 2 WW referral – criteria changed in 2015 2 ww referral age (55) as a factor, Other non-PMB symptoms and tests if aged 55 and over with PMB Consider 2 WW in under 55 with PMB [new 2015] Suspected cancer: Recognition and referral NICE Guideline June 2015 2 WW Referral criteria - PMB Consider direct access USS if > = 55 with unexplained vaginal discharge for first time or with thrombocytosis or report haematuria visible low haematuria with haemoglobin levels or thrombocytosis or high blood glucose levels. [new 2015] Suspected cancer: Recognition and referral NICE Guideline June 2015 PMB 1 Clinic/USS/OPH 1 Clinic/USS 2 Outpatient Hysteroscopy Pathology Failed Hysteroscopy Surgery Pathology Discharge Surgery Discharge 3 GA Hysteroscopy Surgery Discharge Discharge Scan results and outcomes 5mm or thicker endometrium Irregular endometrium Unable to comment on all of the endometrium Negative scan 40% ( negative exam) Endometrial cancer 5-10% Hyperplasia 5% Benign pathology ~15% Atrophic or benign 30% Secondary Care Laparoscopic Hysterectomy and BSO Enhanced Recovery 24-36 hour discharge CNS phone call after 7-10 days and discuss results Case. 42 y old 4 weeks of IMB Stopped the POP one year ago Normal vaginal examination Would you refer on 2WW? NO – IMB has been taken out of 2WW referral criteria Questions ? Croydon University Hospitals Email – [email protected] or 0779525157