Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
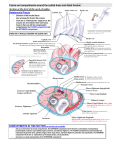
Lecture 9: Forearm bones and muscles Remember, the region between the shoulder and the elbow = brachium/arm, between elbow and wrist = antebrachium/forearm. Forearm bones : ● Humerus (distal ends) ● Radius ● Ulna Forearm regions: ● Cubital fossa ● anterior flexor ● posterior extensor On the humerus, the medial supracondylar ridge (which meets up with the medial epicondyle) and the lateral supracondylar ridge meets up with the lateral epicondyle. These two meet up with condyles, the capitulum (laterally) takes the head of the radius, and the trochlea (medial) takes the olecranon of the ulna. Just above the condyles, there are two fossae. The coronoid fossa and the radial fossa. During elbow flexion, the ulna sits in the coronoid fossa, and the radius sits in the radial fossa. During extension, the olecranon of the ulna sits in the olecranon fossa (a fossa above the condyles on the posterior surface). Ulna, radius and interosseous membrane: Ulna (medial) lies inline with the pinky finger. Starts of quite wide (proximally) and tapers to be quite narrow distally. Unusually, in the ulna, the distal end is the head (usually the proximal end is the head for bones). The proximal end has a curved shaped called the semilunar notch with two bony projections (superiorly the olecranon process & inferiorly the coronoid process). The C shaped notch between these two projections is the semilunar notch. On the lateral side of the ulna there is radial notch (which takes the head of the radius). Slightly inferior to that is the tuberosity of the ulna (which takes the brachialis muscle). Distally (the head), the bony projection is called the styloid process. The radius (is deeply placed in the forearm, harder to palpate than the ulna). The radius has a rounded head (proximal this time, c.f. the ulna) which sits in the radial notch of the ulna. There is a small constriction inferior to the head called the neck. Slightly inferior to the neck is the tuberosity of the radius which takes the biceps. At the distal end the radius widens (c.f. the narrowing of the ulna distally. in some ways they are opposites). There is another styloid process. Note, there are two styloid processes then, and we call them the styloid process of the radius and of the ulna separately. However, these two come together to form an arch shape where the wrist bones will sit. The interosseous membrane forms the syndesmosis joint between the radius and ulna. This allows for the transference of stress between the radius and ulna so that forces are shared. When someone falls on an outstretched hand, is it the radius that projects and takes the force, and will result in a fracture in the distal end of the radius. This is called a Colles’ fracture of the radius. It also results in the posterior displacement of the wrist and hand. Dislocation and fracture of the ulna: Falling on a flexed elbow can cause a fracture in the coronoid process of the ulna and breakaway. This may cause a dislocation of the elbow joint. This is very important because there are several major structures that pass through this region (the anterior side of the elbow = cubital fossa) e.g. median nerve which provides the nerve supply for the anterior anterior/flexor compartment. Also the brachial artery. If the muscles don’t get enough blood supply you can get Volkmann's ischaemia, where the muscles remain tightly flexed and degenerate. Fascial compartments: Muscles are enclosed in fascia. Helps separates functional groups of muscles and exert pressure within the muscle compartment. ● Fascia of the arm (brachial) and forearm (antebrachial) tightly binds down muscles ● Significant rise in pressure (e.g. from bleeding or oedema, inflammation etc.) can lead to compression of contents which can be quite painful called a compartment syndrome (increased pressure within a fascial compartment) In a compartment syndrome, veins and lymphatics are likely to be first affected, then superficial nerves, then arteries, then deep nerves being compressed. Essentially, the vessels/vasculature that have the thinnest body walls will be first affected (hence veins and lymphatics first), then superficial nerves which lie subcutaneous tissue (superficial fascia) then arteries then deep nerves being compressed. At the arm (brachial fascia) you have brachial fascia that separates the flexor compartment from the extensor compartment. That same fascia when it reaches the forearm region is called the antebrachial fascia and separates the flexor muscles of the forearm from the extensor muscles. However, when the same fascia reaches the wrist (palmar and dorsal aspect) the fascia becomes thicker and forms a retinaculum (one flexor and one extensor). These two retinaculum are important because most of the tendons which travel into the hand go through windows formed in the retinaculum. Cubital fossa: The cubital fossa is between the medial and lateral epicondyles of the humerus (so imagine we draw a horizontal line, dotted line in above picture), pronator teres (medially) and brachioradialis (laterally). Sitting on top of the cubital fossa is the bicipital aponeurosis (the roof). Deeply (i.e. the floor) there is the brachialis muscle and supinator muscle (deeper). Several structures lie in this space, which when disrupted can cause damage to the nerve and blood innervation in the antebrachial region (i.e. Volkmann's ischaemia). Superficial veins (cephalic vein laterally, and basilic vein medially) meet in the cubital fossa to form the median cubital vein. This is where blood samples are typically drawn from. These are very much in the skin region (roof) of cubital fossa. On either side of the veins we have the lateral and medial cutaneous nerves of the forearm. These are also in the roof. Deeper, we have the brachial artery which divides distally into the radial and ulnar artery. Along with this, the main nerve supply (median) nerve runs. On the lateral side, going into the supinator muscle we have the radial nerve, on the medial side we have the ulnar nerve. Muscles of the forearm: ● Flexors are more powerful than extensors ● Skin overlying the flexor muscles is more sensitive than that over extensors i.e. more nerve endings running to the skin on the flexor side than extensor side ● Supplied by 3 nerves: median, ulnar and radial. Anterior flexor compartment: Organised into 3 layers (8 muscles): Superficial (‘PFPF’) (4 muscle) Intermediate (FDS) (1 muscle) Deep (FPL, FDP, PQ) (3) 1. Superficial layer (medially to laterally): pronator teres (PT) (does not cross the wrist, ulnar to radius, important in pronation, and has two heads which the median nerve travels between) (so repetitive action of pronation can compress the median nerve) flexor carpi radialis (FCR) (inserts on base of first metacarpal, therefore crosses wrist joint) (important because laterally to the tendon is the radial artery, useful for getting a pulse at the wrist) palmaris longus (PL) (this is the one that is absent in a large percentage of population) (starts from CFO and inserts on palmar aponeurosis, functionally not as important) (sits right on top of the median nerve, meaning in those without the PL the median nerve is slightly exposed) flexor carpi ulnaris (FCU) (ulnar side, inserts on 5th metacarpal) (innervated entirely by the ulnar nerve) (the ulnar artery runs medially, the lateral side is the radial artery, pulse of the ulnar artery is not as well felt because it is deeper) All arise from common flexor origin (CFO) on the medial epicondyle. 2. Intermediate layer Flexor digitorum superficialis (FDS) (this has a long sweeping origin, from CFO and shaft of radius) (median nerve goes deep to the muscle) (travels all the way the medial four digits 4 separate tendons) (each of the 4 digit tendons then split into two and insert on the base of the middle phalanges) (allows for flexion of proximal phalanges and metacarpophalangeal joint) from CFO, radius and ulna 3. Deep layer flexor pollicis longus (FPL) (lateral side, shaft of the radius, inserts on the distal tips of the phalanges of the thumb) (thumb flexion) flexor digitorum profundus (FDP) (travels through carpal tunnel) (distal tendons then travel between and under the space formed by the flexor digitorum superficialis at the phalanges. the tendons then continue to insert on the distal phalanges of the medial 4 digits) (digit flexion, particular of the distal phalanges) pronator quadratus (PQ) (doesn’t cross wrist joint) (between ulnar and radius) (allows for pronation along with pronator teres) all from radius, ulna and/or IO membrane Pronators and supinators: pronator teres pronator quadratus Together these pronate the forearm. Supinators (posterior compartment, so not a flexor): supination is the more powerful action, also produced by the biceps. The radius moves relative to the ulna. That is, during pronation (i.e. from supination to pronation), the radius moves over the ulna, and the ulna stays relatively still. Posterior (extensor) compartment: 11 muscles in the extensor compartment 2 layers: superficial (6) and deep (5) 1. Superficial layer Brachioradialis (it is the exception because whereas most of the muscle start from the common extensor region CEO, the brachioradialis starts from the supracondylar ridge, lateral side) (it doesn’t cross the wrist joint, it goes to the distal end of the radius) (despite the fact that it is a muscle of the posterior compartment and so it is innervated by the nerve of the posterior compartment, the radial nerve, functionally, it works with the anterior compartment) (helps with flexion of wrist) (and is on the anterior side, lateral most muscle) Extensor carpi radialis longus (ECRL) (goes to 2nd metacarpal) (ECRL and ECRB as they get to the wrist their tendons are crossed by the muscles that work on the thumb (EPB, EPL and APL) Extensor carpi radialis brevis (ECRB) (goes to 3rd metacarpal) Extensor digitorum communis (EDC) (goes to medial four digits) (travels through the tunnel deep to the extensor retinaculum which has compartments for each of the 4 tendons) (as it travels to the distal phalanges it forms a extensor expansion hood which refers to the spreading of the tendons over the distal phalanges so that all phalanges extend together) Extensor digiti minimi (EDM) (independent movement of little finger in extension) Extensor carpi ulnaris (ECU) (both the extensor carpi ulnaris and flexor carpi ulnaris can work independently for extension and flexion respectively, but if they work together they operate to perform ulnar deviation movement of wrist towards midline) anconeus (see also arm extensors previously grouped with triceps, some consider it part of the upper arm, others as part of the forearm) Most arise from the common extensor origin (CEO) 2. Deep layer: supinator (doesn’t cross the wrist joint. in the extensor compartment the two muscles that don’t cross the wrist joint are supinator and brachioradialis) (starts from ulna to body of the radius) (radial nerve posterior compartment nerve comes from the posterior compartment and travels to the anterior compartment at the cubital fossa and splits into two divisions, the superficial nerve that travels deep through the brachioradialis, and the deep division of the nerve pierces the supinator. the deep division is the one that provides innervation to the muscles of the posterior compartment. the superficial radial nerve innervates the brachioradialis and is also present in the anatomical snuffbox) abductor pollicis longus (APL) extensor pollicis brevis (EPB) extensor pollicis longus (EPL) (the three APL, EPB and EPL insert on the thumb, and allow for thumb extension extensor indicis (EI) Most arise from the ulna and/or radius and interosseous membrane The APL and the EPB form the lateral border of the anatomical snuffbox and the EPL forms the medial border of the anatomical snuffbox.