Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
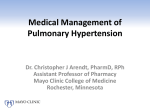
Tadalafil Therapy for Pulmonary Arterial Hypertension Nazzareno Galiè, Bruce H. Brundage, Hossein A. Ghofrani, Ronald J. Oudiz, Gerald Simonneau, Zeenat Safdar, Shelley Shapiro, R. James White, Melanie Chan, Anthony Beardsworth, Lyn Frumkin, Robyn J. Barst and on behalf of the Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group Circulation published online May 26, 2009; DOI: 10.1161/CIRCULATIONAHA.108.839274 Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX 72514 Copyright © 2009 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org Data Supplement (unedited) at: http://circ.ahajournals.org/cgi/content/full/CIRCULATIONAHA.108.839274/DC1 Portions of this reprint may contain information that is not within the full prescribing information for ADCIRCA® (tadalafil) tablets. Subscriptions: Information about subscribing to Circulation is online at http://circ.ahajournals.org/subscriptions/ Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Fax: 410-528-8550. E-mail: [email protected] Reprints: Information about reprints can be found online at http://www.lww.com/reprints Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 Hypertension Tadalafil Therapy for Pulmonary Arterial Hypertension Nazzareno Galiè, MD; Bruce H. Brundage, MD; Hossein A. Ghofrani, MD; Ronald J. Oudiz, MD; Gerald Simonneau, MD; Zeenat Safdar, MD; Shelley Shapiro, MD; R. James White, MD; Melanie Chan, PhD; Anthony Beardsworth, MD; Lyn Frumkin, MD, PhD; Robyn J. Barst, MD; on behalf of the Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group* Background—Treatment options for pulmonary arterial hypertension target the prostacyclin, endothelin, or nitric oxide pathways. Tadalafil, a phosphodiesterase type-5 inhibitor, increases cGMP, the final mediator in the nitric oxide pathway. Methods and Results—In this 16-week, double-blind, placebo-controlled study, 405 patients with pulmonary arterial hypertension (idiopathic or associated), either treatment-naive or on background therapy with the endothelin receptor antagonist bosentan, were randomized to placebo or tadalafil 2.5, 10, 20, or 40 mg orally once daily. The primary end point was the change from baseline to week 16 in the distance walked in 6 minutes. Changes in World Health Organization functional class, clinical worsening, and health-related quality of life were also assessed. Patients completing the 16-week study could enter a long-term extension study. Tadalafil increased the distance walked in 6 minutes in a dose-dependent manner; only the 40-mg dose met the prespecified level of statistical significance (P 0.01). Overall, the mean placebo-corrected treatment effect was 33 m (95% confidence interval, 15 to 50 m). In the bosentan-naive group, the treatment effect was 44 m (95% confidence interval, 20 to 69 m) compared with 23 m (95% confidence interval, 2 to 48 m) in patients on background bosentan therapy. Tadalafil 40 mg improved the time to clinical worsening (P 0.041), incidence of clinical worsening (68% relative risk reduction; P 0.038), and healthrelated quality of life. The changes in World Health Organization functional class were not statistically significant. The most common treatment-related adverse events reported with tadalafil were headache, myalgia, and flushing. Conclusions—In patients with pulmonary arterial hypertension, tadalafil 40 mg was well tolerated and improved exercise capacity and quality of life measures and reduced clinical worsening. (Circulation. 2009;119:000-000.) Key Words: hypertension, pulmonary P ulmonary arterial hypertension (PAH) is a progressive disease defined by chronic elevation in the pulmonary arterial pressure, often leading to right heart failure and death.1,2 The pathogenesis of PAH is poorly understood, but an imbalance between vascular cell proliferation and apoptosis, an influx of cellular inflammation, excess vasoconstriction, and in situ thrombosis all contribute to the narrowing or obliteration of the pulmonary arteriolar lumens and increased pulmonary vascular resistance.3–5 Clinical Perspective on p There is no cure for PAH; however, the currently approved treatment options (ie, prostanoids, endothelin receptor antag- phosphodiesterase inhibitors tadalafil onists, and the phosphodiesterase type-5 inhibitor sildenafil)6 improve symptoms, exercise capacity, and clinical outcome but are limited by either parenteral or inhaled delivery systems, the need for laboratory monitoring, or frequent dosing schedules. Thus, a convenient and safe oral once-daily therapy could be a significant advance in the treatment algorithm for PAH.7 PAH is associated with impaired release of nitric oxide8 at least in part because of reduced expression of nitric oxide synthase in the vascular endothelium of pulmonary arteries.9 Downstream activation of soluble guanylate cyclase is thus reduced, with less cellular synthesis of cGMP. Phosphodiesterase type-5 inactivates cGMP in the pulmonary vasculature, Received November 30, 2008; accepted April 10, 2009. From the Institute of Cardiology, Università di Bologna, Bologna, Italy (N.G.); Heart Institute of the Cascades, Bend, Ore (B.H.B.); University Hospital, Justus-Liebig University, Giessen, Germany (H.A.G.); Los Angeles Biomedical Research Institute at Harbor–University of California at Los Angeles, Torrance, Calif (R.J.O.); Antoine Béclère University Hospital, Clamart, France (G.S.); Division of Pulmonary and Critical Care Medicine, Baylor College of Medicine, Houston, Tex (Z.S.); Greater Los Angeles Veterans Affairs Healthcare System, David Geffen University of California at Los Angeles School of Medicine (S.S.); Division of Pulmonary and Critical Care Medicine, University of Rochester, Rochester, NY (R.J.W.); Eli Lilly and Company, Erl Wood, United Kingdom (A.B.); Eli Lilly and Company, Toronto, Ontario, Canada (M.C.); ICOS Corporation, Bothell, Wash (L.F.); and Schneider Children’s Hospital North Shore–Long Island Jewish Health System, New Hyde Park, NY (R.J.B.). *Study Group participants are listed in the Appendix. The online-only Data Supplement is available with this article at http://circ.ahajournals.org/cgi/content/full/CIRCULATIONAHA.108.839274/DC1. Clinical trial registration information—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00125918. Correspondence to Nazzareno Galiè, MD, Institute of Cardiology, University of Bologna, Via Massarenti 9, 40138 Bologna, Italy. E-mail [email protected] © 2009 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.108.839274 Downloaded from circ.ahajournals.org 1by TOMMY BROCK on May 27, 2009 2 Circulation June 9, 2009 Figure 1. Numbers of patients enrolled in the 16-week study and in the long-term extension study who underwent screening and randomization. The data cutoff for patients in the long-term extension study was October 4, 2007. and it appears to be upregulated in pulmonary hypertension.10,11 Inhibition of phosphodiesterase type-5 increases cGMP levels, which may mediate the antiproliferative12 and vasodilating13 effects of endogenous nitric oxide. Controlled trials of sildenafil in the treatment of PAH patients have shown improvement in exercise capacity and hemodynamic parameters.14 –16 However, sildenafil did not delay the time to clinical worsening, and these studies provided no information about the efficacy or safety of sildenafil when combined with the endothelin receptor antagonist bosentan. Tadalafil, an orally administered, once-daily dosing, selective inhibitor of phosphodiesterase type-5, is currently approved for the treatment of erectile dysfunction.17 Data on tadalafil for the treatment of PAH are limited to a single-dose hemodynamic evaluation18 or anecdotal clinical use.19 The objectives of our double-blind, placebo-controlled clinical trial were to investigate the efficacy and tolerability of 4 doses of oral tadalafil 2.5, 10, 20, and 40 mg given once daily for 16 weeks in PAH patients with or without background bosentan therapy. Selection of Patients Methods Patients were at least 12 years of age and had symptomatic PAH that was idiopathic/heritable or related to anorexigen use, connective tissue disease, HIV infection, or congenital systemic-to-pulmonary shunts (ie, an atrial septal defect with resting arterial oxygen saturation 88% on room air or at least 1-year postsurgical repair of a ventricular septal defect and/or patent ductus arteriosus). The diagnosis of PAH included resting mean pulmonary artery pressure 25 mm Hg, pulmonary wedge pressure 15 mm Hg, and pulmonary vascular resistance 3 Wood units. Patients with a 6-minute walk distance of 150 m or 450 m were excluded. Treatment with intravenous epoprostenol, intravenous or inhaled iloprost, or subcutaneous treprostinil was prohibited. Patients taking a maximal stable dose of 125 mg bosentan twice daily for a minimum of 12 weeks at the time of screening continued on bosentan in addition to the study medication. Local institutional review boards or independent ethics committees approved the protocol, and written informed consent (and assent when appropriate) was obtained from all patients. Study Design This was a 16-week, randomized, double-blind, double-dummy, placebo-controlled, multicenter study conducted in 84 centers in Canada, the United States, Europe, and Japan between August 2005 and August 2007. Patients were randomized to groups receiving 1 of 5 treatments (tadalafil 2.5 mg, 10 mg, 20 mg, 40 mg, or placebo once daily). The randomization was stratified for baseline walking distance ( 325 m or 325 m), Type of PAH (idiopathic/heritable and anorexigen use versus other types), and bosentan use. Hemodynamic parameters, by right heart catheterization, were measured at baseline and at week 16 in patients recruited at 26 sites in North America, Europe, and Japan (hemodynamic substudy). All patients who completed the 16-week, double-blind study (or who discontinued because of clinical worsening and who were not receiving tadalafil 40 mg) were eligible for a long-term extension study and received either tadalafil 20 mg (those who received this dose during the 16-week study) or 40 mg (all other doses groups) in a blinded fashion. Outcome Measures The primary efficacy measure was the placebo-corrected change from baseline to week 16 in 6-minute walk distance.20 Secondary efficacy evaluations included World Health Organization (WHO) functional class,21 time from randomization to clinical worsening (defined as death; lung or heart-lung transplantation; atrial septostomy; hospitalization due to worsening PAH; initiation of new PAHapproved therapy; worsening WHO functional class), Borg dyspnea score,20 quality of life by the Medical Outcomes Study 36-item short form version 222 and the EuroQol-5D questionnaire,23 and hemodynamic measurements in a subset of patients. Six-minute walk distance, WHO functional class, and Borg dyspnea score were measured at baseline and at weeks 4, 8, 12, and 16. Safety evaluations included the recording of adverse events, laboratory tests, and vital signs. Statistical Analysis The database and all statistical outputs were retained by the sponsor. All authors had access to the database. The statistician involved in Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 Galiè et al Table 1. Tadalafil in Pulmonary Arterial Hypertension 3 Baseline Characteristics of the Patients Tadalafil Placebo (n 82) 2.5 mg (n 82) 10 mg (n 80) 20 mg (n 82) 40 mg (n 79) 55 15 54 16 54 15 53 16 53 15 Female 65 (79) 64 (78) 67 (84) 62 (76) 59 (75) Male 17 (21) 18 (22) 13 (16) 20 (24) 20 (25) White 72 (88) 65 (79) 64 (80) 61 (74) 64 (81) Asian 3 (4) 9 (11) 5 (6) 9 (11) 8 (10) African descent 7 (9) 7 (9) 8 (10) 8 (10) 4 (5) Other 0 (0) 1 (1) 3 (4) 4 (5) 3 (4) Weight, kg 77 22 76 20 74 21 76 21 74 19 Characteristic Age, y Gender, n (%) Race, n (%) Duration of PAH, n (%) 0 to 2y 49 (60) 41 (50) 47 (59) 46 (56) 41 (52) 2 to 4y 13 (16) 16 (20) 22 (28) 12 (15) 14 (18) 20 (24) 25 (30) 11 (14) 24 (29) 24 (30) 54 (66) 45 (55) 52 (65) 50 (61) 46 (58) 2 (2) 5 (6) 1 (1) 4 (5) 4 (5) 16 (20) 16 (20) 23 (29) 21 (26) 19 (24) 4y Pathogenesis, n (%) Idiopathic/familial Anorexigen use Connective tissue disease Associated with an atrial septal defect 9 (11) 7 (9) 4 (5) 4 (5) 8 (10) Surgical repair of VSD or PDA duration 1 (1) 9 (11) 0 (0) 3 (4) 2 (3) 1-year Concomitant use of bosentan, n (%) Six-minute walk distance, m Borg dyspnea score 45 (55) 43 (52) 41 (51) 45 (55) 42 (53) 343 84 347 71 338 75 338 74 352 78 4 2 4 2 4 2 4 2 4 2 WHO functional class, n (%) Class I 1 (1) 1 (1) 0 (0) 0 (0) 2 (3) Class II 23 (28) 29 (35) 24 (30) 28 (34) 26 (33) Class III 56 (68) 49 (60) 54 (68) 54 (66) 51 (65) Class IV 2 (2) 3 (4) 2 (3) 0 (0) 0 (0) 16 24 18 17 18 Hemodynamic parameters at baseline in the patients enrolled in the hemodynamic substudy n Mean pulmonary artery pressure, mm Hg Cardiac index, L min 1 m 2 Pulmonary vascular resistance, dyne s cm 5 49 12 54 15 51 16 58 13 54 8 2.4 0.5 2.5 0.7 2.6 0.8 2.6 0.4 2.6 0.7 827 399 852 416 843 475 972 392 901 488 Plus-minus values are mean SD. PAH indicates pulmonary arterial hypertension; VSD, ventricular septal defect; PDA, patent ductus arteriosus. the analysis (M.C.) is an employee of the sponsor. The authors assume full responsibility for the completeness and accuracy of the content of the manuscript. Analysis of efficacy end points included all randomized patients who received study medication (intent-to-treat analysis). Step-down testing began with the tadalafil 40 mg dose and then proceeded downward on the basis of achieving a 2-sided significance level of 0.01 for the preceding test for primary end point. If the primary end point for the dose was statistically significant, the secondary end points were then evaluated in this order: WHO functional class, time to first occurrence of clinical worsening, and change in Borg dyspnea score, with no inferential testing beyond a nonsignificant result. The significance level for secondary end points was a 2-sided significance level of 0.05. The primary end point was tested with a permutation test on rank, stratified by randomization factors. For patients who died or clini- cally worsened, the lowest rank was used. No change was assumed when rank was assigned in patients who discontinued the study because of treatment-related adverse events. For all other patients, the change from baseline to last nonmissing observation was used to assign the rank. Treatment difference was estimated by the ANCOVA model with type II sum of squares including terms for randomization factors. Patients in each treatment group who improved, had no change, or worsened from baseline to week 16, as assessed by WHO functional class, were analyzed by Cochran-Mantel-Haenszel test, which controlled for stratification factors. Patients with missing data at week 16 were considered to worsen from baseline. Time from randomization to the first occurrence of clinical worsening was analyzed with a permutation test on the log-rank score stratified by randomization factors. Subjects who completed Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 4 Circulation June 9, 2009 the study or discontinued early without clinical worsening were considered censored at the time of study completion. Frequency of subjects who experienced clinical worsening was tested by Fisher exact test. Borg dyspnea score was analyzed by the same technique used for the 6-minute walk distance. Change from baseline to week 16 in both quality of life surveys was compared with placebo with an ANCOVA model that controlled for randomization factors. Hemodynamic parameters at week 16 were compared with baseline with a paired t test. Permutation test was performed with StatXact with 10 000 Monte Carlo samples.24 Other tests were performed with SAS version 8 (SAS Statistical Software, version 8, 1999; SAS Institute Inc, Cary, NC). A sample size of 400 patients (80 patients per treatment group) provided 90% power at an level (2-sided) of 0.001 to detect a 45-meter placebo-adjusted treatment effect in 6-minute walk distance. Results A total of 405 patients were randomized into 1 of 5 treatment arms and received study medication (Figure 1) between August 2005 and August 2007. Baseline Patient Characteristics Baseline patient characteristics were balanced across treatment arms (Table 1). The majority of patients had symptoms in WHO functional class II or III and had idiopathic/heritable PAH; 53% of patients were receiving background bosentan therapy. Baseline characteristics were generally well balanced across background treatment groups; however, patients on background bosentan tended to be younger, had a longer duration of PAH, and had a slightly higher baseline 6-minute walk distance than those patients not on background bosentan (data not shown). Exercise Capacity Tadalafil 10, 20, and 40 mg (but not 2.5 mg), compared with placebo, significantly improved the distance walked in 6 minutes in a dose-dependent manner at week 16 (Figure 2). Tadalafil 40 mg was the only dose that achieved the prespecified value of statistical significance (P 0.01). The mean placebo-corrected treatment effects among the 392 patients with postbaseline assessment were 14 m among those receiving tadalafil 2.5 mg (n 79; 95% confidence interval [CI], 6 to 33); 20 m for those receiving 10 mg (n 78; 95% CI, 1 to 39); 27 m for those receiving 20 mg (n 82; 95% CI, 11 to 44); and 33 m for those receiving 40 mg (n 79; 95% CI, 15 to 50). In 11 patients, a 6-minute walk distance measured before 16 weeks was used in the analysis (1, 5, 3, 2, and 0 patients in the placebo and tadalafil 2.5, 10, 20, and 40 mg groups, respectively). Treatment Effect Between Patient Subgroups The treatment effects for the primary end point in predefined subgroups were evaluated (Figure 3). Tadalafil 40 mg consistently demonstrated improvements in 6-minute walk distance compared with placebo. The placebo-adjusted change in 6-minute walk distance in treatment-naive patients was 44 m (n 186; 95% CI, 20 to 69; P 0.01) compared with 23 m (n 206; 95% CI, 2 to 48; P 0.09) for patients on background bosentan. The placebo-adjusted change in 6-minute walk distance in WHO functional class I and II patients was 24 m (95% Figure 2. Mean changes from baseline, with 95% CIs, in the 6-minute walking distance at week 16 in the tadalafil and placebo groups. With the use of a permutation test on rank stratified according to baseline walking distance, cause of PAH, and bosentan use, P 0.402, P 0.047, P 0.028, and P 0.001 for the comparison of tadalafil in doses of 2.5, 10, 20, and 40 mg, respectively, with placebo. In this intention-to-treat analysis, 392 patients for whom outcome data were available were included in descriptive statistics. The dosing schedule for all study medications was once daily. CI, 0 to 48; P 0.04) compared with 36 m (95% CI, 11 to 60; P 0.02) in WHO class III and IV patients. WHO Functional Class No statistically significant differences in the proportion of patients with improved WHO functional class and no change in WHO functional class or worsening in WHO functional class were observed with tadalafil compared with placebo. A post hoc exploratory analysis based on background bosentan use was done. In treatment-naive patients, 37.8% improved and 10.8% worsened in the tadalafil 40 mg group; 16.2% of patients improved and 21.6% worsened in the placebo group (P 0.03). In the patients on background bosentan therapy, 9.5% improved and 9.5% worsened in the tadalafil 40 mg group; 24.4% of patients improved and 11.1% worsened in the placebo group (P 0.05). Clinical Worsening Time to clinical worsening was significantly improved in the tadalafil 40 mg group compared with placebo (P 0.041) (Figure 4). Additionally, the incidence of clinical worsening was reduced in the tadalafil 40 mg group (P 0.038; relative risk reduction 68% less than placebo). Individual components of clinical worsening are shown in Table 2; hospitalization and worsening of WHO functional class rates were lower in the tadalafil 40 mg group compared with the placebo group. Borg Dyspnea Score Changes in the Borg dyspnea scale did not differ between patients treated with tadalafil and those receiving placebo. Quality of Life Statistically significant improvements, compared with placebo, from baseline to week 16 were observed in 6 of the 8 domains of the Medical Outcomes Study 36-item short form version 2 Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 Galiè et al Tadalafil in Pulmonary Arterial Hypertension 5 Figure 3. Placebo-corrected effect of treatment on the 6-minute walking distance from baseline to week 16 in patients subgroups. The treatment effects, with 95% CIs, are presented for each tadalafil dose. ITT indicates intention-to-treat; S-P, systemic-to-pulmonary. In this analysis, 392 patients for whom outcome data were available were included. The dosing schedule for all study medications was once daily. Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 6 Circulation June 9, 2009 Figure 4. Kaplan–Meier estimates of the proportion of patients with clinical worsening. With the use of a permutation test on log-rank stratified according to baseline walking distance, cause of PAH, and bosentan use, *P 0.041 for the comparison of tadalafil in dose of 40 mg versus placebo. In this intention-to-treat analysis, all 405 patients who were randomized and treated were included. The dosing schedule for all study medications was once daily. health survey (all P 0.01) and for all sections of the EuroQol-5D questionnaire (all P 0.02) in the tadalafil 40 mg group. Hemodynamic Parameters Hemodynamic data were available for 93 patients. Improvements were observed with tadalafil 20 and 40 mg compared with baseline in mean pulmonary arterial pressure ( 8.5 mm Hg; 95% CI, 13 to 4; n 17, P 0.001; and 4.3 mm Hg; 95% CI, 8 to 1; n 18, P 0.01, respectively) and pulmonary vascular resistance ( 254 dyne · s · cm 5; 95% CI, 388 to 120; n 17, P 0.001; and 209 dyne · s · cm 5; 95% CI, 406 to 13; n 18, P 0.039, respectively). A statistically significant improvement in cardiac index was seen in the tadalafil 40 mg group (0.6 L/min per square meter; 95% CI, 0.1 to 1.6; n 18, P 0.028). No changes were observed on mean systemic blood pressure. Although we recognize the limitations of background treatment subgroup analyses for the secondary outcome measures due to the small sample sizes, the data showed uniformly better results in the naive patients compared with the patients on background bosentan therapy. Safety All doses of tadalafil were generally well tolerated, with the most common adverse events being headache, myalgia, and flushing. Most adverse events were reported as mild or moderate (Table 2). Discontinuation rates were 16% and similar across all treatment groups (Figure 1). No clinically significant changes were seen in any laboratory variables evaluated. Fifty-four patients reported 74 serious adverse events, equally distributed across all treatment groups. However, investigators only considered 12 events as possibly related to study medication; these included nausea, vomiting, retinal artery occlusion, dyspnea, priapism, esophageal varices hemorrhage, hypotension, gastritis, menorrhagia, histiocytosis hematophagic syndrome, headache, and drug hypersensitivity. Three deaths occurred during the 16-week study: 1 patient in the placebo group died because of PAH progression, 1 patient in the 10-mg tadalafil group died suddenly, and the third death was due to histiocytosis hematophagic syndrome in a patient on tadalafil 20 mg. Adverse events were not significantly different between the naive patients compared with the patients on background bosentan therapy. Long-Term Extension Study Of the 341 patients who completed the randomized 16week study, 334 entered the long-term prospective extension study; 7 declined enrollment (Figure 1). In addition, 23 patients who prematurely discontinued the placebocontrolled study because of clinical worsening also entered the extension study. Of the 357 patients enrolled in the extension study, 62 patients discontinued (Figure 1). As of October 2007, 213 of 357 patients (60%) enrolled in the extension study had received tadalafil for at least 10 months. After 16 weeks of treatment, the mean change from baseline in the 6-minute walking distance for these patients was 37 m (95% CI, 30 to 44); after 44 weeks, the mean change was 38 m (95% CI, 29 to 47). Discussion The results of this study show that tadalafil improves exercise capacity, as assessed by the 6-minute walk distance, in patients with PAH. Importantly, 53% of patients were on background therapy with bosentan. The placebo-corrected increase in walking distance in the group of patients treated with 40 mg of tadalafil was 33 m (also including patients on background bosentan therapy), and these data are consistent with those observed in other pivotal studies, ranging from 16 to 59 m, on approved PAH medications utilized as monotherapy.15,25–30 In this study, the increase in walking distance Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 Galiè et al Tadalafil in Pulmonary Arterial Hypertension 7 Table 2. Incidence of Clinical Worsening and of Most Frequent Adverse Events in the Placebo and Tadalafil Groups Tadalafil Clinical worsening, n (%)* Placebo (n 82) 2.5 mg (n 82) 10 mg (n 80) 20 mg (n 82) 40 mg (n 79) 13 (16) 10 (12) 7 (9) 9 (11) 4 (5)‡ 1 1§ Death 1 Hospitalization for worsening PAH 2 2 2 1 11 10 6 6 3 Headache 12 (15) 15 (18) 30 (38) 26 (32) 33 (42) Diarrhea 8 (10) 9 (11) 9 (11) 6 (7) 9 (11) Nausea 5 (6) 6 (7) 7 (9) 8 (10) 9 (11) Back pain 5 (6) 5 (6) 5 (6) 10 (12) 8 (10) Dyspepsia 2 (2) 4 (5) 2 (3) 11 (13) 8 (10) Flushing 2 (2) 3 (4) 5 (6) 5 (6) 10 (13) Myalgia 3 (4) 2 (2) 3 (4) 7 (9) 11 (14) Dyspnea 3 (4) 8 (10) 4 (5) 4 (5) 5 (6) Pain in extremity 2 (2) 3 (4) 4 (5) 4 (5) 9 (11) Initiation of new PAH therapy Worsening WHO functional class 3 1 1 Adverse event, n (%)*† Muscle spasms 2 (2) 4 (5) 8 (10) 5 (6) 2 (3) Upper respiratory tract infection 3 (4) 5 (6) 5 (6) 4 (5) 5 (6) Epistaxis 3 (4) 6 (7) 4 (5) 5 (6) 3 (4) Palpitations 2 (2) 5 (6) 7 (9) 3 (4) 1 (1) Arthralgia 1 (1) 4 (5) 7 (9) 2 (2) 2 (3) Chest pain 1 (1) 4 (5) 1 (1) 5 (6) 5 (6) Vomiting 1 (1) 2 (2) 2 (3) 6 (7) 5 (6) Fatigue 3 (4) 4 (5) 1 (1) 4 (5) 5 (6) Nasal congestion 1 (1) 3 (4) 3 (4) 0 (0) 7 (9) Edema 1 (1) 3 (4) 1 (1) 4 (5) 4 (5) Bronchitis 0 (0) 3 (4) 3 (4) 1 (1) 4 (5) Hot flush 2 (2) 4 (5) 2 (3) 2 (2) 3 (4) Insomnia 2 (2) 2 (2) 1 (1) 4 (5) 3 (4) Urinary tract infection 0 (0) 3 (4) 2 (3) 2 (2) 3 (4) Vision blurred 1 (1) 2 (2) 2 (3) 4 (5) 2 (3) *The analysis included all patients who received at least 1 dose of study medication. Some patients reported 1 event. †Adverse events listed are those reported by 3% of patients and those that were reported more frequently in the tadalafil-treated group than in the placebo group. ‡P 0.038 by Fisher exact test on the frequency of clinical worsening. §The subject who died in the tadalafil 20 mg group was reported after study discontinuation. In the log-rank test, this subject was censored at the time of study discontinuation. with tadalafil 40 mg in the treatment-naive patients (44 m) was higher than that observed in the patients on background bosentan (23 m), although the latter was not statistically significant (Figure 3). In addition, the effects on all secondary end points tended to be better in treatment-naive patients compared with bosentan-treated subjects. These comparative data, observed for the first time within a single study, support the hypothesis that increases in exercise capacity may be blunted in patients already treated with PAH-targeted medications31,32 compared with treatment-naive subjects.15,25–30 The reasons for this observation are not clear but may be related to a ceiling phenomenon33 that limits additional improvements in exercise capacity in patients on background therapy with targeted PAH medications. In addition, tadalafil plasma levels are reduced if the dose of 40 mg is coadministered with bosentan34 because of a pharmacokinetic interaction mediated by the cytochrome P450 3A4, and this might decrease tadalafil pharmacodynamic effects. A similar pharmacokinetic phenomenon is also observed with the coadministration of sildenafil and bosentan.35 Higher doses of phosphodiesterase type-5 inhibitors might theoretically be needed in patients with bosentan background therapy, and specific trials may be required to clarify this issue. The extension study suggests that the favorable effect of tadalafil on exercise capacity is durable for at least 10 months of treatment. The proportion of patients who showed im- Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 8 Circulation June 9, 2009 provement in WHO functional class did not differ between the placebo and the tadalafil 40 mg groups. The reasons for this are unclear and may be due, in part, to the large proportion of patients on background bosentan for whom it may be more difficult to improve WHO functional class compared with those without background therapy. The results from the post hoc exploratory analysis on WHO functional class improvement in the bosentan-naive patients treated with tadalafil 40 mg support this hypothesis. The tadalafil 40 mg group versus placebo significantly decreased the incidence of clinical worsening (Figure 4), in which fewer WHO functional class deteriorations and hospitalizations were observed (Table 2). Delay of clinical deterioration has been reported with PAH treatments either as monotherapy27,29,30,36,37 or in combination trials31,32 but was not observed in the pivotal sildenafil study.15 The reasons for these differing observations among phosphodiesterase type-5 inhibitors are not clear and may include a difference in the definitions used for clinical worsening, differences in trial duration (12 versus 16 weeks), differences in the patient populations studied, differences in the time in history or countries in which the studies were performed, and/or differences in effects of the 2 drugs on this specific parameter. Prevention of clinical deterioration is regarded as clinically important supportive evidence for efficacy with PAH medications and has been suggested as a possible primary end point in future PAH clinical trials provided that a uniform and less subjective definition is used.37–39 The lack of a statistically or clinically significant improvement in Borg dyspnea score despite an improvement in exercise capacity in this study has also been observed in other studies with PAH medications.15,25,27–29,31,32,37 In fact, it is rare to observe treatment effects 0.5 to 1.0 points (out of 10). It is possible that this phenomenon is related to the tendency of the patients to maximize their effort in walking at each study visit, resulting in a similar level of dyspnea regardless of distance walked. The improvement in quality of life indices demonstrated in this study has been reported in previous PAH trials.25,26,29,32,37,40 It is particularly encouraging that the improvements observed in this trial were seen in a population that included a large proportion of patients already on background bosentan treatment, thus providing a rationale for additional targeted therapy. In a subgroup of patients, tadalafil significantly improved hemodynamic parameters. The improvements in pulmonary artery pressure and cardiac index in the group treated with tadalafil 40 mg were similar to those observed with other PAH medications either as monotherapy25,30,36,37,41,42 or in combination.31,32 The small number of patients enrolled in this subgroup does not allow a comparison among tadalafil doses. For example, the larger decrease in mean pulmonary arterial pressure observed with the 20-mg dose compared with the 40-mg dose may be due to chance alone because the CIs are largely superimposed. Because hemodynamic variables have been related to survival in patients with idiopathic/ familial PAH, these hemodynamic data add further support to the clinical utility of tadalafil. For all doses of tadalafil, most adverse events were mild to moderate in severity (Table 2); there were no clinically significant changes in laboratory variables measured. Thus, tadalafil, taken once daily, contrasts with the currently approved PAH medications, including those using complex delivery systems,25,30 oral agents with effects on liver function,27–29 and agents requiring frequent dosing regimens.15,26 Although longer-term assessments are needed to confirm the favorable safety profile of tadalafil, the benefit-to-risk ratio of its combination with the endothelin receptor-A selective antagonists (ambrisentan and sitaxsentan) and with prostanoids requires evaluation. On the basis of our results, overall, tadalafil 40 mg appears to be the optimal dose for PAH patients. Tadalafil 40 mg, unlike lower doses of tadalafil, significantly improved exercise capacity, clinical worsening, quality of life, and hemodynamics and had a safety profile similar to that of the lower doses. Of note, the findings of this study are related to the “sequential” addition of tadalafil to patients already treated with bosentan and do not address the possible benefit of the concurrent initiation of the 2 drugs in treatment-naive subjects. In conclusion, this study demonstrates the safety and efficacy of tadalafil for the treatment of patients with symptomatic PAH. The favorable efficacy-to-safety profile of tadalafil 40 mg once daily offers a clinically meaningful addition to the currently approved treatment options. Appendix The members of the Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group were as follows (in order of the number of patients randomized at each center): A. Manes, Bologna, Italy; L. Negro, Bologna, Italy; A. Palazzini, Bologna, Italy; Z. Safdar, Houston, Tex; S. Shapiro, Los Angeles, Calif; R.J. White, Rochester, NY; R.J. Barst, New York, NY; E. Berman Rosenzweig, New York, NY; R. Girgis, Baltimore, Md; F. Grimminger, Giessen, Germany; W. Seeger, Giessen, Germany; J. Feldman, Phoenix, Ariz; G. Simonneau, Clamart, France; J. Klinger, Providence, RI; V. Cottin, Bron Cedex, France; J. Granton, Toronto, Ontario, Canada; N. Nakanishi, Osaka, Japan; G. Stahler, Loewenstein, Germany; S. Mehta, London, Ontario, Canada; G. Coghlan, London, United Kingdom; D. Ostrow, Vancouver, British Columbia, Canada; D. Badesch, Denver, Colo; J. Behr, Muenchen, Germany; L. Bruch, Berlin, Germany; H. Farber, Boston, Mass; C. Lawrence, Atlanta, Ga; C. Markin, Portland, Ore; O. Minai, Cleveland, Ohio; G. Saydain, Detroit, Mich; M. Widmer, Bend, Ore; B. Degano, Toulouse, France; S. Fazio, Napoli, Italy; M. Gomberg-Maitland, Chicago, Ill; D. Langleben, Montreal, Quebec, Canada; J. Meyer, Heidelberg, Germany; J. Michaelson, Decatur, Ga; E. Michelakis, Edmondton, Alberta, Canada; R. Naeije, Brussels, Belgium; A. Peacock, Glasgow, United Kingdom; B. Rayburn, Birmingham, Ala; M. Chakinala, St Louis, Mo; T. De Marco, San Francisco, Calif; F. Fedele, Roma, Italy; R. Frantz, Rochester, Minn; M.A. GomezSanchez, Madrid, Spain; D. Helmersen, Calgary, Alberta, Canada; P. Hernandez, Halifax, Nova Scotia, Canada; A. Hurewitz, Mineola, NY; A. Waxman, Boston, Mass; D. Baratz, Phoenix, Ariz; C. Campana, Pavia, Italy; E. Hachulla, Lille Cedex, France; N. Hill, Boston, Mass; S. Knoper, Tucson, Ariz; K. Kusano, Okayama, Japan; M. Mathier, Pittsburgh, Pa; S. Murali, Pittsburgh, Pa; S. Ogawa, Tokyo, Japan; J. Pepke-Zaba, Cambridgeshire, United Kingdom; J. Barbera, Barcelona, Spain; R.J. Oudiz, Torrance, Calif; Z. Bshouty, Winnipeg, Manitoba, Canada; D. Camanga, Torrance, Calif; M. Colvin-Adams, Minneapolis, Minn; M. Delcroix, Leuven, Belgium; R. Ewert, Greifswald, Germany; J. Gossage, Augusta, Ga; F. Grimminger, Lich, Germany; H. Matsubara, Okayama, Japan; O. Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 Galiè et al Miera, Berlin, Germany; M. Mizoguchi, Fukuoka, Japan; M. Pfeifer, Regensburg, Germany; M. Reynaud-Gaubert, Marseille, France; H. Watanabe, Shizuoka, Japan; D. Zwicke, Milwaukee, Wis; P. Corris, Newcastle on Tyne, United Kingdom; G. Elliott, Salt Lake City, Utah; H. Endo, Kanagawa, Japan; P. Fairman, Richmond, Va; S. Gaine, Dublin, Ireland; D. Kiely, Sheffield, United Kingdom; Y. Kihara, Hyogo, Japan; H. Kuraishi, Kanagawa, Japan; P. MoralesMartin, Valencia, Spain; J. Suzuki, Tokyo, Japan; Y. Takeda, Aichi, Japan; T. Zieldalski, Everett, Wash. Acknowledgments Tadalafil in Pulmonary Arterial Hypertension 9. 10. 11. Michael Anne Shane, MS, assisted in the coordination and editing of this manuscript. 12. Source of Funding 13. Disclosures 14. The study was funded by Eli Lilly and Company. Nazzareno Galiè, MD, has served as a member of the PHIRST steering committee for Eli Lilly and has participated in advisory board activities for Actelion, Pfizer, United Therapeutics, Eli Lilly, Bayer-Schering, Encysive, and GlaxoSmithKline. He has been a paid lecturer for Actelion, Pfizer, Bayer-Schering, and Encysive. Bruce H. Brundage, MD, has served as a consultant or advisory board member for the following companies: Actelion, GTx, Pfizer, Gilead, Medtronics, Eli Lilly, United Therapeutics. Hossein A. Ghofrani, MD, has received honoraria and acts as a consultant for Actelion, Bayer Schering, Encysive, Ergonex, GlaxoSmithKline, Novartis, and Pfizer. Ronald J. Oudiz, MD, has served as member of the PHIRST steering committee/advisory board for Eli Lilly . Gerald Simonneau, MD, has served as member of the PHIRST steering committee for Eli Lilly/ICOS and has participated in advisory board activities and has served as consultant for Actelion, Pfizer, United Therapeutics, Eli Lilly, Bayer-Schering, and GlaxoSmithKline. He is a paid lecturer for Actelion, Pfizer, and Bayer-Schering. Zeenat Safdar, MD, has consulting agreements with Actelion, Encysive, Gilead, and United Therapeutics. Shelley Shapiro, MD, has speaker and consulting agreements with Actelion, Eli Lilly, Gilead, and United Therapeutics. R. James White, MD, acts as a consultant for Actelion, Gilead, and United Therapeutics and has received research funds from a US NIH grant to the University of Rochester General Clinical Research Center. Melanie Chan, PhD, is an employee and stockholder of Eli Lilly . Anthony Beardsworth, MD, is an employee and stockholder of Eli Lilly. Lyn Frumkin, MD, PhD, is a former employee at ICOS Corporation, the codeveloper (with Eli Lilly) of tadalafil. Robyn J. Barst, MD, serves as a consultant to Actelion, Eli Lilly, Gilead, Pfizer, Novartis, and GlaxoSmithKline. References 1. Rubin LJ. Primary pulmonary hypertension. N Engl J Med. 1997;336: 111–117. 2. Galie N, Rubin L, eds. Pulmonary arterial hypertension: epidemiology, pathobiology, assessment and therapy. J Am Coll Cardiol. 2004;43: S1–S90. 3. Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J Med. 2004;351:1655–1665. 4. Pietra GG, Capron F, Stewart S, Leone O, Humbert M, Robbins IM, Reid LM, Tuder RM. Pathologic assessment of vasculopathies in pulmonary hypertension. J Am Coll Cardiol. 2004;43:S25–S32. 5. Humbert M, Morrell NW, Archer SL, Stenmark KR, MacLean MR, Lang IM, Christman BW, Weir EK, Eickelberg O, Voelkel NF, Rabinovitch M. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43:S13–S24. 6. Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004;351:1425–1436. 7. Badesch DB, Abman SH, Simonneau G, Rubin LJ, McLaughlin VV. Medical therapy for pulmonary arterial hypertension: updated ACCP evidence-based clinical practice guidelines. Chest. 2007;131:1917–1928. 8. Archer SL, Djaballah K, Humbert M, Weir KE, Fartoukh M, Dallava SJ, Mercier JC, Simonneau G, Tuan DX. Nitric oxide deficiency in 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 9 fenfluramine- and dexfenfluramine-induced pulmonary hypertension. Am J Respir Crit Care Med. 1998;158:1061–1067. Giaid A, Saleh D. Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. N Engl J Med. 1995;333:214 –221. Wharton J, Strange JW, Moller GMO, Growcott EJ, Ren X, Franklyn AP, Phillips SC, Wilkins MR. Antiproliferative effects of phosphodiesterase type 5 inhibition in human pulmonary artery cells. Am J Respir Crit Care Med. 2005;172:105–113. Corbin JD, Beasley A, Blount MA, Francis SH. High lung PDE5: a strong basis for treating pulmonary hypertension with PDE5 inhibitors. Biochem Biophys Res Commun. 2005;334:930 –938. Tantini B, Manes A, Fiumana E, Pignatti C, Guarnieri G, Zannoli R, Branzi A, Galie N. Antiproliferative effect of sildenafil on human pulmonary artery smooth muscle cells. Basic Res Cardiol. 2005;100:131–138. Michelakis E, Tymchak W, Lien D, Webster L, Hashimoto K, Archer S. Oral sildenafil is an effective and specific pulmonary vasodilator in patients with pulmonary arterial hypertension: comparison with inhaled nitric oxide. Circulation. 2002;105:2398 –2403. Sastry BKS, Narasimhan C, Reddy NK, Raju BS. Clinical efficacy of sildenafil in primary pulmonary hypertension, I: a randomized, placebocontrolled, double-blind, crossover study. J Am Coll Cardiol. 2004;43: 1149 –1153. Galie N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, Fleming T, Parpia T, Burgess G, Branzi A, Grimminger F, Kurzyna M, Simonneau G; the Sildenafil Use in Pulmonary Arterial Hypertension (SUPER) Study Group. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 2005;353:2148 –2157. Singh T, Rohit M, Grover A, Malhotra S, Vijayvergiya R. A randomized, placebo-controlled, double-blind, crossover study to evaluate the efficacy of oral sildenafil therapy in severe pulmonary artery hypertension. Am Heart J. 2006;151:851.e1– 851.e5. Cialis (tadalafil) product label. Food and Drug Administration Web site. Available at: http://www.fda.gov/cder/drug/infopage/cialis/default.htm. Accessed February 1, 2008. Ghofrani HA, Voswinckel R, Reichenberger F, Olschewski H, Haredza P, Karadaş B, Schermuly RT, Weissmann N, Seeger W, Grimminger F. Differences in hemodynamic and oxygenation responses to three different phosphodiesterase-5 inhibitors in patients with pulmonary arterial hypertension: a randomized prospective study. J Am Coll Cardiol. 2004;44: 1488 –1496. Palmieri EA, Affuso F, Fazio S, Lembo D. Tadalafil in primary pulmonary arterial hypertension. Ann Intern Med. 2004;141:743–744. Guyatt GH, Sullivan MJ, Thompson PJ, Fallen EL, Pugsley SO, Taylor DW, Berman LB. The 6-minute walk: a new measure of exercise capacity in patients with chronic failure. Can Med Assoc J. 1985;132:919 –923. Barst R, McGoon M, Torbicki A, Sitbon O, Krowka MJ, Olschewski A, Gaine S. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43:S40 –S47. Ware JEJ, Kosinski M, Gandek B. SF-36® Health Survey: Manual & Interpretation Guide. 2nd ed. Lincoln, RI: Qualitymetric, Inc; 2000. Rabin R. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33:337–343. StatXact Procs for SAS Users: Statistical Software for Exact Nonparametric Inference (User Manual). Version 6 ed. Cambridge, Mass: Cytel Software Corporation; 2004. Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, Bourge RC, Keogh A, Oudiz R, Frost A, Blackburn SD, Crow JW, Rubin LJ. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165:800 – 804. Olschewski H, Simonneau G, Galie N, Higenbottam T, Naeije R, Rubin LJ, Nikkho S, Sitbon O, Speich R, Hoeper M, Behr J, Winkler J, Seeger W, for the AIR Study Group. Inhaled iloprost in severe pulmonary hypertension. N Engl J Med. 2002;347:322–329. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, Pulido T, Frost A, Roux S, Leconte I, Landzberg M, Simonneau G. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002;346: 896 –903. Barst R, Langleben D, Badesch BD, Frost A, Lawrence EC, Shapiro RS, Naeije R, Galie N. Sitaxsentan therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2006;47:2049 –2056. Galie N, Olschewski H, Oudiz RJ, Torres F, Frost A, Ghofrani HA, Badesch DB, McGoon MD, McLaughlin VV, Roecker EB, Gerber MJ, Dufton C, Wiens BL, Rubin LJ, for the Ambrisentan in Pulmonary Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009 10 30. 31. 32. 33. 34. Circulation June 9, 2009 Arterial Hypertension Study Group. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy (ARIES) Study 1 and 2. Circulation. 2008;117: 3010 –3019. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, Groves BM, Tapson VF, Bourge RC, Brundage BH; the Primary Pulmonary Hypertension Study Group. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. 1996;334:296 –302. McLaughlin VV, Oudiz RJ, Frost A, Tapson VF, Murali S, Channick RN, Badesch DB, Barst RJ, Hsu HH, Rubin LJ. Randomized study of adding inhaled iloprost to existing bosentan in pulmonary arterial hypertension. Am J Respir Crit Care Med. 2006;174:1257–1263. Simonneau G, Rubin L, Galie N, Barst RJ, Fleming T, Frost A, Engel PJ, Kramer MR, Burgess G, Collings L, Cossons N, Sitbon O, Badesch BD, for the Pulmonary Arterial Hypertension Combination Study of Epoprostenol and Sildenafil (PACES) Study Group. Addition of sildenafil to long-term intravenous epoprostenol therapy in patients with pulmonary arterial hypertension. Ann Intern Med. 2008;149:521–530. Frost A, Langleben D, Oudiz R, Hill D, Horn E, Mc Laughlin VV, Robbins I, Shapiro RS, Tapson V, Zwicke D, DeMarco T, Schilz R, Ruchelli ED, Rubenfire M, Barst R, for the STRIDE-1 Study Group. The 6-min walk test (6MW) as an efficacy endpoint in pulmonary arterial hypertension clinical trials: demonstration of a ceiling effect. Vasc Pharmacol. 2005;43:36 –39. Wrishko RE, Dingemanse J, Yu A, Darstein C, Phillips DL, Mitchell MI. Pharmacokinetic interaction between tadalafil and bosentan in healthy male subjects. J Clin Pharmacol. 2008;48:610 – 618. 35. Burgess G, Hoogkamer H, Collings L, Dingemanse J. Mutual pharmacokinetic interactions between steady-state bosentan and sildenafil. Eur J Clin Pharmacol. 2008;64:43–50. 36. Channick RN, Simonneau G, Sitbon O, Robbins IM, Frost A, Tapson VF, Badesch DB, Roux S, Rainisio M, Bodin F, Rubin LJ. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet. 2001;358: 1119 –1123. 37. Galiè N, Rubin LJ, Hoeper M, Jansa P, Al-Hiti H, Meyer GMB, Chiossi E, Kusic-Pajic A, Simonneau G. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet. 2008;371:2093–2100. 38. Dhaun N, Webb DJ. Endothelin-receptor antagonism: the future is bright. Lancet. 2008;371:2061–2062. 39. Farber HW. The status of pulmonary arterial hypertension in 2008. Circulation. 2008;117:2966 –2968. 40. Pepke-Zaba J, Gilbert C, Collings L, Brown MCJ. Sildenafil improves health-related quality of life in patients with pulmonary arterial hypertension. Chest. 2008;133:183–189. 41. Barst RJ, Langleben D, Frost A, Horn EM, Oudiz R, Shapiro S, McLaughlin V, Hill N, Tapson VF, Robbins IM, Zwicke D, Duncan B, Dixon RA, Frumkin LR. Sitaxsentan therapy for pulmonary arterial hypertension. Am J Respir Crit Care Med. 2004;169:441– 447. 42. Galie N, Badesch BD, Oudiz R, Simonneau G, McGoon M, Keogh A, Frost A, Zwicke D, Naeije R, Shapiro RS, Olschewski H, Rubin L. Ambrisentan therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2005;46:529 –535. CLINICAL PERSPECTIVE There is no cure for pulmonary arterial hypertension, a devastating, progressive disease with increasingly debilitating symptoms. Currently approved treatment options include prostanoids, endothelin receptor antagonists, and a phosphodiesterase type-5 inhibitor. These therapies improve symptoms, exercise capacity, hemodynamics, and clinical outcome but are limited by either parenteral or inhaled delivery systems, the need for laboratory monitoring, or frequent dosing schedules. In addition, the majority of pivotal trials have shown the efficacy-to-safety balance of the approved medications when administered as monotherapy, and less information is available on the effects of these drugs when combined with background therapy with other approved compounds. The results of the Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) study provide evidence for the efficacy of the orally active phosphodiesterase type-5 inhibitor tadalafil at a dose of 40 mg once daily. The effects on exercise capacity and hemodynamics are comparable to those of the other drugs approved for pulmonary arterial hypertension. Furthermore, tadalafil 40 mg is able to improve time to clinical worsening, most adverse events were mild to moderate in severity, and there were no clinically significant changes in laboratory variables measured. Therefore, the favorable efficacy-to-safety profile of tadalafil 40 mg once daily offers a clinically meaningful addition to the currently approved treatment options. Approximately 50% of the patients enrolled in the PHIRST study were on background therapy with the endothelin receptor antagonist bosentan; in this subgroup as well, the favorable effects of tadalafil 40 mg were confirmed, although by a lesser extent. These data may support the use of combination therapy in pulmonary arterial hypertension. Downloaded from circ.ahajournals.org by TOMMY BROCK on May 27, 2009