Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
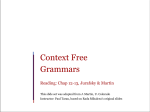
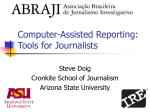
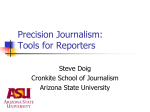
Perspective Annals of Internal Medicine An Academic Center’s Delivery of Care After the Haitian Earthquake Amir K. Jaffer, MD; Rafael E. Campo, MD; Greg Gaski, MD; Mario Reyes, MD; Ralf Gebhard, MD; Enrique Ginzburg, MD; Michael A. Kolber, PhD, MD; John Macdonald, MD; Steven Falcone, MD, MBA; Barth A. Green, MD; Lazara Barreras-Pagan, RN, BHSA; and William W. O’Neill, MD The Miller School of Medicine of the University of Miami and Project Medishare, an affiliated not-for-profit organization, provided a large-scale relief effort in Haiti after the earthquake of 12 January 2010. Their experience demonstrates that academic medical centers in proximity to natural disasters can help deliver effective medical care through a coordinated process involving mobilization of their own resources, establishment of focused management teams at home and on the ground with formal organizational oversight, and partnership with governmental and nongovernmental relief agen- cies. Proximity to the disaster area allows for prompt arrival of medical personnel and equipment. The recruitment and organized deployment of large numbers of local and national volunteers are indispensable parts of this effort. Multidisciplinary teams on short rotations can form the core of the medical response. T and a simple intensive care unit), supply storage, and staff quarters. Other supplies were airlifted from Miami several times daily. Approximately 140 patients from our first facility were transported to the new hospital on 21 January 2010. Staffing of the hospital was accomplished almost exclusively through volunteers who signed up for 5- to 7-day deployments. A travel clinic was set up in Miami to provide counseling for deploying volunteers, and a Web-based survey for returning volunteers was used to assess their adherence to malaria prophylaxis and to determine whether referrals for medical or psychological issues were needed. To coordinate efforts, we created under the supervision of a chief medical officer an organizational structure that mirrored our hospital structure in Miami but also addressed Haiti-specific issues. Because of the massive damage to the communications infrastructure, we set up satellite links for telephone and Internet connections. The command groups in Haiti and Miami had joint conference calls every morning, during which the day’s goals and plans were determined. he 12 January 2010 earthquake in Haiti, one of the worst natural disasters in the past 2 centuries, left 230 000 dead and 1.5 million homeless. Given the University of Miami’s proximity to Haiti and a 15-year relationship with Haitian physicians through Project Medishare, a not-for-profit health care organization set up by Miller School of Medicine faculty, the university was able to offer emergency relief within 20 hours after the earthquake. We have previously described our experience during the week after the earthquake (1). Here we describe the University of Miami Hospital in Haiti, a field hospital that began functioning at the Port-au-Prince airport 8 days after the earthquake (Figure 1). ORGANIZATION OF SYSTEMS, TEAMS, FIELD HOSPITAL AND THE Given the magnitude of the relief effort, it immediately became apparent that logistic organization would be as challenging as delivering care. Critical needs were obvious: coordination of flights from Miami into a damaged airport; provision of guidance regarding medical precautions for hundreds of volunteers; and transportation of massive amounts of medical supplies, food, and water. We quickly established an organization table to keep track of multiple aspects of the operation (Figure 2) and put together a coordinating center housed at our Miami campus. Our initial hospital was a small facility within the United Nations compound that we rapidly outgrew (1). The second hospital was constructed in 4 days after flying in 2 electric generators, construction equipment, and 4 air-conditioned tents from Miami: one tent each for a pediatric ward and an adult ward (with 4 operating rooms See also: Web-Only Conversion of graphics into slides Ann Intern Med. 2010;153:262-265. For author affiliations, see end of text. This article was published at www.annals.org on 20 July 2010. CLINICAL CARE AND www.annals.org COORDINATION Because of limited resources and the large number of patients in need, medical and surgical triage was of paramount importance. On arrival, patients were triaged by an internist or a pediatrician, and then an appropriate surgeon (trauma, orthopedic, or neurosurgery) developed a plan of care. Many of our nursing and medical staff were of Haitian origin and spoke Creole. Family members helped in caring and feeding patients. Limbs with gross infection and impending sepsis or compromised vascular flow had emergent guillotine amputation and staged debridement after 3 treating surgeons concurred and patients gave written consent through a Creole interpreter. No amputation was closed before the third debridement. Open fractures were scheduled for repeated debridement every 2 to 3 days. There was a low 262 © 2010 American College of Physicians Downloaded From: http://annals.org/pdfaccess.ashx?url=/data/journals/aim/20212/ on 05/04/2017 An Academic Center’s Delivery of Care After the Haitian Earthquake threshold for repeated operative debridement. Intraoperative fluoroscopy permitted application of external fixators when appropriate. Because of the challenging field conditions, we chose not to undertake internal fixation. Patients requiring this were transferred to the USNS COMFORT or the United States. More than 203 surgical procedures were performed between postearthquake days 4 and 12. We treated 48 chronic compartment syndromes by postearthquake day 12. On postearthquake day 10, we acquired a digital radiography machine and casted nearly all closed ankle, tibia, wrist, and forearm fractures (more than 98 in 3 days). Best attempts were made at closed reduction by orthopedic surgeons. The need for a wound care team became apparent—approximately 80% of patients had open wounds. Our wound care program consisted of both adult and pediatric bedside teams for dressing changes that were equipped to handle major debridement and vacuumassisted closure application with conscious sedation. Patients requiring surgical intervention in the immediate aftermath of an earthquake frequently have extremity injuries that are challenging in anesthetic management, because many individuals develop hypovolemia, sepsis, electrolyte, and coagulation disturbances (2, 3) that can complicate general and neuraxial anesthesia. Peripheral nerve blocks have a favorable safety profile and provide adequate anesthesia independent of oxygen supplies and electricity and, if necessary, with only limited monitoring. Therefore, most surgeries were performed under local peripheral nerve blocks, and only some complex surgical cases were performed under general anesthesia. Perspective Figure 1. Aerial view of University of Miami Hospital, Port-au-Prince, Haiti. Arrow A is the location of the operating room in the posterior part of the first tent. Arrow B is where the wound center was located. Arrow C is the triage area. Arrow D is the second triage tent, where the pediatric patients were admitted. Arrow E is the tent where staff and health care workers were housed. The supplies tent is to the left but is not included in the photograph. Internists, pediatricians, and hospitalists focused on the medical management of surgical patients (for example, fluid and pain management and thromboembolism prophylaxis) and were responsible for the logistic aspects of organizing and running the hospital. Infectious diseases specialists helped select antibiotic regimens from a simple yet robust antimicrobial formulary. Combined medical- Figure 2. Organization of the team at the command center in Miami. Chief Medical Officer Chief Administrative Officer Security/ Facilities/ IT/Telecom Lead Personnel and Flight Logistics Lead Rotation Material Donations Lead Fundraising Telecom, Facilities Coordinator Material Donations Lead Fundraising Telecom Coordinator Fundraising IT Coordinator Grant writer IT Coordinator Finance Fundraising Finance Airport Ramp, Warehouse, and Transportation Lead Supply Chain Lead Coordinator Coordinator Coordinator Nonmedical Supplies Public Relations/ Communications Lead Medications Consultant Airplane and Flight Slots Office Manager/ Manifest/ Volunteer Coordinator Information Line Information Line Receptionist/ Information Line Volunteer Spreadsheet Teams were created with a lead person responsible for each team, including finance, fundraising, IT, security, personnel and flight logistics, material donations, airport operations, supply chain, public relations and communications, and volunteers. IT ⫽ information technology. www.annals.org 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 263 Downloaded From: http://annals.org/pdfaccess.ashx?url=/data/journals/aim/20212/ on 05/04/2017 Perspective An Academic Center’s Delivery of Care After the Haitian Earthquake Figure 3. Initial presentation and radiographic diagnosis of a pelvic fracture. were ready for discharge. The organization of the pediatric ward mirrored that of the adult ward. Besides operative capability, the inability to perform radiography and fluoroscopy when the focus was on managing crush injuries and fractures presented a major challenge. Portable digital radiography and fluoroscopy units were not available for about 10 days. Figure 3 highlights the initial clinical impression of a pelvic fracture that was confirmed when radiography became available. Radiography technicians were always in short supply, and physicians were trained to use the machines by the technicians and the manufacturer’s representatives, who flew to Haiti to provide training. Patients who could not be appropriately cared for at our hospital were transported to the Israel Defense Forces Medical Corps Field Hospital or the USNS COMFORT; some were flown to the United States in a military plane. Many of our health care workers had clinically significant emotional stress. Our psychiatry department dispatched personnel with experience in supporting health care workers involved in disaster relief, and we encouraged volunteers to pair up and monitor each other’s stress. LESSONS LEARNED AND APPLICATION RESPONSES TO DISASTERS Top. Initial presentation documents the initial impression for an earthquake victim admitted on 13 January 2010. Bottom. Radiographic diagnosis confirms the initial impression of pelvic fracture 9 days later on plain radiographs. surgical rounds were held at least once daily, with the objective of establishing a joint plan of care and identifying cases that needed surgical or radiological procedures or TO FUTURE Our university had never been involved in disaster relief of this magnitude. Aspects of our response that did not go as well as we would have hoped included our lack of adequate interaction early with the United States Southern Command based in Doral, Florida (which is responsible for U.S. military operations in South and Central America). Early interaction would have allowed us set up early communications between Haiti and Miami and to better procure and allocate personnel and supplies. Inclusion of immediate first responders who were fluent in Creole would have been most helpful. It also took several days to create an organizational structure for the disaster response de novo. On the basis of our experience, we believe the highest priority should be placed on putting an organizational structure in place at the local institution that is preparing to respond to a natural disaster. This structure should reflect aspects of the operation that are necessary on the ground in the foreign country and at home. We had a difficult time securing voluntary radiography technicians. Soliciting help early from national professional organizations, such as the American Society of Radiologic Technologists, might have prevented this limitation. Immediate creation of a Web-based document that specified medical needs for travel to the area (for example, immunizations and travel documents) and reflected what volunteers should expect to encounter would have been helpful. Preparedness counseling and planned postexposure counseling to deal with posttraumatic stress disorder should have been put in place immediately. 264 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 Downloaded From: http://annals.org/pdfaccess.ashx?url=/data/journals/aim/20212/ on 05/04/2017 www.annals.org An Academic Center’s Delivery of Care After the Haitian Earthquake Despite the limitations and gaps we have outlined, we feel our intervention was successful and that universitybased medical health care systems can play an important role in disaster relief. Our prior relationship with Project Medishare highlights the benefit of academic health centers having established relationships with foreign countries on which disaster response can be built. The critical and core elements of our response included prompt organization of teams and systems both in Miami and in Haiti, communication between personnel in Miami and Port-au-Prince on a scheduled and ongoing basis, deployment of shortstay medical volunteer teams, prompt transportation of essential supplies and equipment, and construction of a simple yet robust field hospital. The early phase of medical care delivery was focused on managing trauma. Very simple radiology equipment proved indispensable for the management of orthopedic trauma. Laboratory support was absent initially; however, many patients were successfully managed initially with clinical examination alone. Our experience and the lessons learned can be applied by medical centers and organizations interested in delivering emergent trauma care during future natural disasters. PERSONAL ARCHIVES Perspective From University of Miami Miller School of Medicine, Miami Children’s Hospital, University of Miami Sylvester Comprehensive Cancer Center, and University of Miami Health System, Miami, Florida. Potential Conflicts of Interest: Disclosures can be viewed at www.acponline .org/authors/icmje/ConflictOfInterestForms.do?msNum⫽M10-0807. Requests for Single Reprints: William W. O’Neill, MD, University of Miami Health System, 1600 Northwest 10th Avenue, RMSB 1122A, Miami, FL 33136; e-mail, [email protected]. Current author addresses and author contributions are available at www .annals.org. References 1. Ginzburg E, O’Neill WW, Goldschmidt-Clermont PJ, de Marchena E, Pust D, Green BA. Rapid medical relief—Project Medishare and the Haitian earthquake. N Engl J Med. 2010;362:e31. [PMID: 20181963] 2. Mulvey JM, Awan SU, Qadri AA, Maqsood MA. Profile of injuries arising from the 2005 Kashmir earthquake: the first 72 h. Injury. 2008;39:554-60. [PMID: 18054014] 3. Yang C, Wang HY, Zhong HJ, Zhou L, Jiang DM, Du DY, et al. The epidemiological analyses of trauma patients in Chongqing teaching hospitals following the Wenchuan earthquake. Injury. 2009;40:488-92. [PMID: 19328487] AND COLLECTIONS Add favorite articles to your personal archives or retrieve collections for the following article types at www.annals.org: Randomized clinical trials Clinical Guidelines and Position Papers Editorials In the Clinic On Being a Doctor and On Being a Patient Reviews Academia and Clinic www.annals.org 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 265 Downloaded From: http://annals.org/pdfaccess.ashx?url=/data/journals/aim/20212/ on 05/04/2017 Annals of Internal Medicine Current Author Addresses: Dr. Jaffer: Department of Medicine, University of Miami Miller School of Medicine, 1120 Northwest 14th Street, 933 CRB (C216), Miami, FL 33136. Dr. Campo: Division of Infectious Diseases, University of Miami Miller School of Medicine, Clinical Research Building, 1120 Northwest 14th Street, Room 855 (R-21), Miami, FL 33136. Dr. Gaski: Department of Orthopedics, University of Miami Miller School of Medicine, PO Box 016960 (D-27), Miami, FL 33101. Dr. Reyes: Division of Pediatric Hospitalists and Pediatric Advance Care Team (PACT), Miami Children’s Hospital, Main Building, Third Floor, 3100 Southwest 62nd Avenue, Miami, FL 33155. Dr. Gebhard: Department of Anesthesiology, University of Miami Miller School of Medicine, 1611 Northwest 12th Avenue, Room C-302, Miami, FL 33136. Dr. Ginzburg: Department of Surgery, University of Miami Miller School of Medicine, 1800 NW 10th Avenue, Miami, FL 33136. Dr. Kolber: Division of Infectious Diseases, University of Miami Miller School of Medicine, Clinical Research Building, 1120 Northwest 14th Street, CRB 859, Miami, FL 33136. Dr. Macdonald: Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, RSMB Room 2023, Miami, FL 33136. Dr. Falcone: University of Miami Miller School of Medicine, 1150 Northwest 14th Street, Suite 701, Miami, FL 33136. Dr. Green: Department of Neurologic Surgery, University of Miami Miller School of Medicine, Lois Pope Life Center, 2nd Floor, 1095 Northwest 14th Terrace (D4-6), Miami, FL 33136. Ms. Barreras-Pagan: University of Miami Sylvester Comprehensive Cancer Center (D-1), 1475 Northwest 12th Avenue, Suite 4037, Miami, FL 33136. Dr. O’Neill: University of Miami Health System, 1600 Northwest 10th Avenue, RMSB 1122A, Miami, FL 33136. Author Contributions: Conception and design: A.K. Jaffer, R.E. Campo, M. Reyes, M.A. Kolber, B.A. Green, L. Barreras-Pagan, W.W. O’Neill. Analysis and interpretation of the data: A.K. Jaffer, R.E. Campo, G. Gaski, J. Macdonald. Drafting of the article: A.K. Jaffer, R.E. Campo, G. Gaski, M. Reyes, R. Gebhard, E. Ginzburg, M.A. Kolber, S. Falcone, W.W. O’Neill. Critical revision of the article for important intellectual content: A.K. Jaffer, R.E. Campo, R. Gebhard, S. Falcone. Final approval of the article: A.K. Jaffer, R.E. Campo, M. Reyes, E. Ginzburg, M.A. Kolber, J. Macdonald, L. Barreras-Pagan, W.W. O’Neill. Provision of study materials or patients: B.A. Green, L. Barreras-Pagan. Administrative, technical, or logistic support: R. Gebhard, L. BarrerasPagan, W.W. O’Neill. Collection and assembly of data: A.K. Jaffer, R.E. Campo, G. Gaski, E. Ginzburg, M.A. Kolber, L. Barreras-Pagan. W-88 17 August 2010 Annals of Internal Medicine Volume 153 • Number 4 Downloaded From: http://annals.org/pdfaccess.ashx?url=/data/journals/aim/20212/ on 05/04/2017 www.annals.org