Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
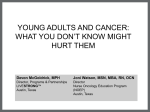
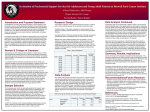
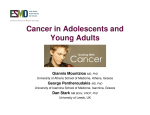
research Five-year experience of McGill University’s Adolescent and Young Adult Oncology Program The challenge of serving a unique population Michael Palumbo, MD, PhD, Petr Kavan, MD, PhD, David Roberge, MD, Thierry Muanza, MD, Sabrina R. Perri, PhD, and Gerald Batist, MD Contributing authors Abstract Progress in pediatric oncology has been among the most dramatic stories in modern medicine. In contrast, survival rates for adolescents and young adults (AYA) with cancer plateaued in the late 1970s. Reasons for this are not fully understood and may include differences in the biology of the cancers, poor understanding of host and tumour physiology, poor enrollment into adult and pediatric clinical trials, and lack of AYA-specific clinical trials. Further, AYA patients suffer from frequent loss to followup, delayed diagnosis and poor treatment compliance. To address these issues, in 2003 McGill University created an AYA oncology program with a corresponding patient registry. After five years in existence the program has achieved increased enrollment into clinical trials (including AYA-specific trials), along with reduced loss to followup. The program has also facilitated tumour banking and the implementation of psychosocial and rehabilitation services crucial to this population. We describe ongoing challenges that will likely affect attempts to establish similar programs elsewhere, and propose possible solutions to these challenges: lack of awareness of the unique therapeutic, psychosocial and rehabilitation needs of this population, the paucity of available clinical trials and the reluctance of some clinicians to refer patients to the program. As we learned with pediatric oncology, improved outcomes in the AYA population will require centralization of AYA oncology programs, along with interprovincial and international cooperation. Petr Kavan MD, PhD is Director of the McGill Adolescent and Young Adult Oncology Program and Associate Professor of Medicine at McGill University. Michael Palumbo, MD, PhD is a Resident in Internal Medicine at McGill University and Director of Statistics for the adolescent and Young Adult Oncology Program. David Roberge, MD and Thierry Muanza, MD are both Assistant Directors of the AYA Program and Assistant Professors of Medicine at McGill. Sabrina R. Perri, PhD is a Regional Medical Liaison in Oncology (Scientific Affairs) at AMGEN Canada Inc., Medical Affairs, Amgen, Canada. Gerald Batist, MD is a Professor and The Director of Oncology at McGill University. Address for correspondence: Dr. Petr Kavan, MD, PhD, E-715, Segal Cancer Center, Jewish General Hospital, 3755 Côte-Ste-Catherine, Montreal, QC, H3T 1E2; Tel: 514 340 8222 ext.4210; Fax: 514 340 8302; Email: [email protected] Mark Karanofsky, MD Richard Dalfen, MD Martin Chasen, MD Evgenia Garoufalis, MD Marie-Christine Guiot, MD Rolando Del Maestro, MD, PhD Richard Leblanc, MD Christine Leblanc, RN Eleanor Scharf, RN, MSc Randi Fogelbaum, MSW, PSW Mary Ann Dalzell, MSc Pht. The contributing authors are from the Adolescent and Young Adult Oncology Program, Department of Oncology, McGill University, Montreal, Quebec, Canada. Rationale The problem Initiatives set forth nearly half a century ago to improve outcomes in children diagnosed with a malignancy have dramatically improved survival. In 1971, The National Cancer Act added adults with cancer as a priority, and considerable advances have been made in a number of adult malignancies. In the mid 1990s, several studies, performed mainly by Bleyer et al, identified a population of patients largely between 15 to 19 years of age who were not benefiting from the advances in either pediatric or adult malignancies.1-4 Recent subgroup analyses, including a Progress Review from The National Cancer Institute (NCI), have determined that improvement in ©2009 Parkhurst, publisher of Oncology Exchange. All rights reserved. 38 Œ VOL. 8, N0. 2, may 2009 research cancer survival has lagged considerably for the 15- to 39-year age group, now referred to by NCI as adolescents and young adults (AYA).5-10 The NCI made several subsequent recommendations in hopes of improving outcomes for this population.6,9 There is no standard international definition of “young adult” — the Public Health Agency of Canada has defined patients suffering from a malignancy between the ages of 20 to 44 years as young adults.11 In this article, AYA denotes patients from 15 to 39 years of age. The incidence of cancer in the North American AYA population is approximately 60 cases per 100,000 men and 100 cases per 100,000 women.11,12 The most common AYA malignancies are breast cancer, lymphoma, melanoma, female genital tract tumours, thyroid carcinoma, soft-tissue sarcomas, testicular cancer, colorectal carcinoma, leukemia, brain tumours and osteosarcoma.6 In comparison to both pediatric and older adult patients, the AYA population tends to have a worse prognosis — particularly when being treated for breast cancer, colorectal cancer, softtissue sarcoma, non-Hodgkin lymphoma or leukemia.6 Suggested explanations for the inferior outcomes include differences in the biology of the cancers, poor understanding of host and tumour physiology, poor enrollment into adult and pediatric clinical trials, and lack of AYA-specific clinical trials. There is evidence that significant improvement in survival can be achieved in patients 15 to 19 years of age with acute lymphoblastic leukemia, Ewing sarcoma, rhabdomyosarcoma, non- Hodgkin lymphoma and primary bone tumours when these patients are treated according to pediatric protocols.5,13-18 Similar results may also hold true for the entire AYA population but studies are lacking. Other suggested explanations for poor AYA outcomes include delayed diagnosis and poor treatment compliance. The NCI recently made landmark recommendations with regards to AYA cancer patients,6,19 among them: • increase the number of AYA patients in clinical trials • increase the number of available specimens for the study of AYA tumour biology • increase our understanding of host and tumour physiology and create a specific classification system for these cancers, rather than using pediatric or adult classifications • review previously acquired clinical trial data for AYA subset analysis • focus initially on cancers that occur with the highest frequency and have the largest differential in prognosis relative to either their adult or pediatric counterparts: sarcoma, leukemia, lymphoma, breast cancer and colorectal cancer. pists, occupational therapists, nutrition specialists and a data manager. Fellows interested in this new subdiscipline are also involved and incorporated as team members. The majority of team members have extensive experience in pediatric care. Entry clinics are at the Royal Victoria Hospital (RVH), Montreal Neurological Hospital (MNH) and Sir Mortimer B. Davis Jewish General Hospital (JGH), and a multidisciplinary clinic is located at the JGH Segal Cancer Centre. The referring physician has the choice of referring a patient for complex treatment or for consultation only. The wide variety of services offered was intended to encompass patients’ needs and requirements during their treatment period. Several clinical research associates on the team, in conjunction with the McGill Clinical Research Program, design, implement and accrue patients into clinical trials. After initial assessment, all patients are presented at the AYA tumour board and if needed at the site-specific tumour board. Tissue banking is also facilitated with the help of AYA-affiliated surgeons and pathologists. The group works closely with cancer support groups established by Hope & Cope, Venturing Out Beyond Our Cancer (VOBOC) and The Cedars Cancer Institute. AYA clinics are held two specific days each week so that AYA patients visit the clinic and infusion room together. AYA program physicians also act as consultants by attending tumour board meetings (sarcoma, brain and gastrointestinal), and are involved in treatment discussions of AYA patients still being assessed by surgeons — critical to obtaining referrals to the AYA program. Soon after its creation, medical and surgical oncologists specializing in breast, hepatic, colorectal, sarcoma and genitourinary cancers began to join the team and refer their patients. This report points out some of our successes and acknowledges some challenges the McGill AYA program faces — challenges that will likely be encountered by other institutions setting up AYA programs. Some of these include increasing the awareness of the therapeutic, psychosocial and rehabilitation needs of AYA patients, McGill’s AYA oncology program In an attempt to meet the challenges faced by AYA patients, in 2003 McGill University created the first AYA oncology program (AYAO) in Canada. This program is now open to patients diagnosed with a malignancy before the age of 39, inclusive (the original age range was 18 to 30, inclusive), and older adults suffering from a pediatrictype malignancy. The program consists of the director (a hematologist/oncologist with pediatric oncology training), two assistant directors (both radiation oncologists, one of whom is also trained in pediatric radiation oncology), medical oncologists (one with specific expertise in rehabilitation), two general practition ers, psychiatrists, psychologists, tumour site-specific surgeons, a team of radiologists to grant patients rapid access to imaging, pathologists, pharmacists, a “pivot” nurse who helps the patient navigate the healthcare system and available resources, clinical nurse specialists, social workers, physiothera- ©2009 Parkhurst, publisher of Oncology Exchange. All rights reserved. Œ VOL. 8, N0. 2, may 2009 39 research Methods We conducted a retrospective chart review of the patients referred to the McGill AYA program from January 2003 until March 2008 who were diagnosed at less than 31 years of age. Most patients were at least 18 years old, as most younger patients are treated in children’s hospitals, but some who were older than 15 and had a typical adult malignancy were referred to the program. FIGURE 1. Age at diagnosis and referral for McGill AYA patients diagnosed with a malignancy at < 31 years of age* 40 35 30 percent increasing the number of available clinical trials and increasing the number of patient referrals. 25 20 15 10 5 0 10–14 15–19 20–24 25–29 Results Patient characteristics and referral statistics Of 160 patients referred to the program, 64 (40%) were female and 96 (60%) were male. Figure 1 shows the age distributions at time of diagnosis and referral: it represents all patients in the program diagnosed with a malignancy before 31 years of age. At present, the AYA program accepts all patients diagnosed with a malignancy at less than 40 years of age, but this was a recent change, based on NCI and Health Canada classifications, and is not reflected in the figure. While the number of referrals increased every year, a review of the tumour registries at McGill’s participating institutions revealed an overall referral rate of 42% at the JGH and 35% at the RVH and MNH. Approximately 44% of patients were referred from Quebec institutions outside the McGill catchment area. Tumour types, reasons for referral and treatment statistics A wide variety of tumour types were seen in the AYA program. Cancer types were 33% sarcoma, 26% brain or other central nervous system (CNS) tumours, 13% leukemia or lymphoma, 11% genitourinary or germ cell tumours, 8% gastrointestinal, 5% melanoma and 4% thyroid and breast cancer. Reasons for referral were: 109 patients (71%) for primary treatment, 29 (19%) for second- or third-line treatment, 11 (7%) for followup and 5 patients (3%) for second opinions. Eighty percent of patients were seen within two weeks of referral, with 15% seen on the same day and 43% seen within the first week. 30–34 age Œ VOL. 8, N0. 2, may 2009 40–44 > 45 n diagnosis n referral * The age range of patients was only changed to 15–44 years recently, based on NCI and Health Canada classifications. Figure 2 shows wait times from first contact to first treatment: 80% received treatment within three weeks of first contact. Clinical trials and outcomes Numerous clinical trials are ongoing at McGill. These include therapeutic, rehabilitation and nutrition program trials and fertility management trials. Several recently initiated Children’s Oncology Group (COG) trials and two AYA-specific trials are actively recruiting patients. Between 2003 and 2007, the overall number of patients enrolled in clinical trials each year has ranged between 14% and 32%, averaging about 27%; of these, 24 (50%) were in therapeutic trials, 17 (36%) were in fertility trials and 6 (13%) were in a nutrition and cancer rehabilitation trial. Figure 3, page 42, shows 5-year survival curves. Of all patients entered into the program since 2003, 36% were in remission, 23% had stable disease (either on or off treatment), 9% had disease progression, 23% had died and approximately 12% had been lost to followup. Overall survival rates were 65% for sarcomas and 88% for brain tumours, which are both major tumour sites. Discussion As previously mentioned, improvement in long-term survival in AYA patients has been minimal compared to pediatric and older adult oncology patients.5,6,10,19 Success in pediatric oncology resulted from initiatives begun several decades ago that recognized the low incidence of cancer in this population (0.5%). Initiatives included concentrating patients within specialized centres, study of tumour biology, and national and international collaborations to design pediatric clinical trials. At 3% to 4% of all cancers, cancer in the AYA population is more frequent but still relatively rare.11,12 Clearly, initiatives similar to those instituted for pediatric malignancies are required to improve treatment outcomes for AYA malignancies. Treating adolescents and young adults with cancer has many associated complexities that AYA centres must be prepared to tackle. From a therapeutic perspective, evidence that pediatric protocols may offer better long-term survival for some AYA malignancies calls for implementation of pediatric protocols at adult sites. The need for increased access to pediatric clinical trials ultimately requires that treating physicians have experience with pediatric protocols, be members of the COG and that sites be recognized by the COG. Many COG protocols, however, have upper age limits that restrict access of AYA patients, and ©2009 Parkhurst, publisher of Oncology Exchange. All rights reserved. 40 35–39 research COG does not have protocols for many adult malignancies, e.g. breast cancer. Although this may change in the future, AYAO sites must also be prepared to design and implement AYA-specific trials through an AYAO cooperative group. Many psychosocial challenges arise when treating AYA patients. They often find treatment in clinics filled with older adults psychologically challenging. They may feel they do not have the time to deal with their cancer or oncology followup schedule because of school, work and social activities. They may misunderstand the seriousness of their disease due to the lack of public knowledge about cancer in AYA patients, combined with a false sense of invincibility common in AYAs. Such factors result in poor treatment compliance and elevated rates of loss to followup. McGill designed its AYAO program in recognition of these considerations. The McGill core team members have pediatric oncology experience and many are part of COG, resulting in successful activation of selected COG trials at an adult institution. Further, our clinical research team has begun to implement AYA-specific trials; future projects include collaborations with other AYA groups to expand the size and number of these trials. Successes The number of patients included in clinical trials in our program has been nearly three- to four-fold greater than that reported in the general AYA oncology population.4,5,9 Concentrating patients together and offering numerous services has reduced loss to followup (12%) in comparison to published rates, which have been reported as being up to 50% to 70% when transitions from pediatric centres to adult care are included.20 Regarding outcomes, five-year survival rates of 50% to 60% for sarcoma patients and of 70% to 80% for brain/CNS tumours have been reported.5,12 Our five-year survival for sarcoma is comparable at 53%; for brain tumours it is higher at 88%, potentially owing to McGill’s strong neuro-oncology program. AYA patient with a typical pediatric malignancy like medulloblastoma or rhadomyosarcoma, a medical oncologist specializing in the management of breast cancer can refer a patient to the program while remaining the treating physician. Referral will allow for increased access to clinical trials, psychosocial services, patient support groups and tumour banking. Cases can then be discussed regularly at AYA tumour board meetings. At the very minimum, patients should be referred for a second opinion so they can be placed on the AYA registry and evaluated for current or upcoming clinical trials. If the patient does not attend the AYA clinics, AYAO teams need the flexibility to meet with patients at non-AYA clinics. Regardless of the method of referral, AYAO programs are needed to promote patient access to pediatric and AYA clinical trials and to allow accumulation of tumour specimens and clinical data to help advance the field of AYA oncology. AYAO programs have an important role in educating physicians about the unique needs of the population and should remain flexible to accommodate their adult oncology colleagues. AYAO patients diagnosed with readily treatable malignancies such as testicular tumours should also be referred to the program. Not only will they likely benefit from the psychosocial and rehabilitation programs, but those presenting with advanced or refractory disease should be enrolled in clinical trials. Even those presenting with favourable disease pathology may benefit from being included in trials looking at reducing the treatment intensity and subsequent toxic side effects. All pediatric oncology patients should be referred, given the small yet non-negligible increased risk of malignancy throughout life and the physical, psychosocial and fertility side effects of therapeutic interventions, as well as implications for future insurance coverage. Importantly, a small subset of these cancer survivors (e.g. hereditary retinoblastoma patients) will be at significantly increased risk for second malignancies and complications. Considering that the average pediatrician or family practitioner lacks extensive experience with rare tumours Challenges Despite team efforts and increasing collaborations between hematologists and medical/surgical oncologists, the percentage of patients referred (42%) is still low. This is an obstacle many institutions will likely face when instituting an AYA program. With the expanding definition of AYA now encompassing patients aged anywhere from 15 to 39 or 44, obtaining referrals may become increasingly problematic. Cancer specialists need to be made be aware that referral to the program does not necessarily change the treating physician. While referral for treatment by an AYA oncologist with pediatric experience is likely appropriate for an FIGURE 2. Wait times from first contact to first treatment 35.00 29.21 30.00 percent 25.00 20.22 20.00 16.85 15.73 15.00 10.00 5.62 5.00 3.37 5.62 1.12 2.25 ≤ 49 > 49 0.00 same day ≤ 7 ≤ 14 ≤ 21 ≤ 28 ≤ 35 ≤ 42 days ©2009 Parkhurst, publisher of Oncology Exchange. All rights reserved. Œ VOL. 8, N0. 2, may 2009 41 research Toward age-sensitive oncology care No matter how much attention and specialized care AYAO patients receive, the significance of the unique biologic and psychosocial implications of age cannot be overstated. In the pediatric setting, where this concept was recognized long ago, the development of specialized programs has had a powerful impact. Interestingly, recent experimental and clinical experience suggests that a comparable scenario may also be true of elderly (> 70 years) patients with cancer.21 A potential model to consider in a comprehensive cancer centre is to view all patients not only with regard to their tumour diagnosis, but to offer additional treatment and research designed to respond to patients through the ages: pediatric, adolescent and young adult, mature adult and elderly. Such a scenario is challenging and requires creative evaluation of current practice, but is likely critical to optimizing cancer care. n Œ Disclosure AMGEN Canada Inc. provides McGill’s AYA program with research support. Dr. Batist reports serving on Amgen advisory boards. Dr. Kavan reports receiving research support from Amgen and Hoffmann-La Roche and being on advisory boards of Amgen, Hoffmann-la Roche, SanofiAventis and Schering-Plough. No other potential conflicts of interest were reported. References 1. Albritton K, Bleyer WA.The management of cancer in the older adolescent. Eur J Cancer. 2003;39(18):2584-99. 2. Bleyer A. Older adolescents with cancer in North America deficits in outcome and research. Pediatr Clin North Am. 2002 Oct;49(5):1027-42. 3. Bleyer WA. Cancer in older adolescents and young adults: epidemiology, diagnosis, treatment, survival, and importance of clinical trials. Med Pediatr Oncol 2002 Jan;38(1):1-10. 4. Bleyer WA, Tejeda H, Murphy SB et al. National cancer clinical trials: children have equal access; adolescents do not. J Adolesc Health 1997;21(6):366-73. 5. Bleyer A. Young adult oncology: the patients and their survival challenges. CA Cancer J Clin 2007;57(4):242-55. 6. Bleyer A, Barr R, Hayes-Lattin B et al. The distinctive biology of cancer in adolescents and young adults. Nat Rev Cancer 2008;8(4):288-98. FIGURE 3. Five-year survival curves for McGill AYA patients 120.00 t n 5 100.00 t n 5 t 5 n t 5 n t 5 n 80.00 percent and their therapeutic side effects, referral to a more experienced team for regular followup may be beneficial. 5 t n Œ VOL. 8, N0. 2, may 2009 5 5 t n n t 60.00 n t 40.00 20.00 0.00 0 1 3 6 12 24 36 48 60 months n t 5 7. Bleyer, WA, O’Leary, M, Barr, R et al. Cancer Epidemiology in Older Adolescents and Young Adults 15 to 29 Years of Age, Including SEER Incidence and Survival, 1975-2000. 2006 [cited; Available from www.seer.cancer.gov/publications/aya 8. Gibbon DG, Schaar D, Kamen B. A call to action: Cancer in adolescents and young adults: An unrecognized healthcare disparity. J Pediatr Hematol Oncol 2006;28(9):549-51. 9. National Institutes of Health. Closing the gap: Research and care imperatives for adolescents and young adults with cancer. A report of the Adolescent and Young Adult Oncology Progress Review Group. 2006. Available from http:// planning.cancer.gov/disease/AYAO_PRG_ Report_2006_FINAL.pdf 10. Schmidt C. Lack of progress in teen and young adult cancers concerns researchers, prompts study. J Natl Cancer Inst 2006;98(24):1760-3. 11. Cancer Care Ontario. Cancer in Young Adults in Canada. Toronto, ON, Canada, May 2006. Available at www.cancercare.on.ca/toolbox/libraries/ hcplibrary/ 12. Surveillance, Epidemiology and End Results (SEER) Program. Adolescent and Young Adult Cancer by Site, Incidence, Survival and Mortality. 2005 [cited; Available from www.seer.cancer.gov > Statistics > Cancer statistics review > 32. Adult and Young Adult Cancer 13. Boissel N, Auclerc MF, Lhéritier V et al. Should adolescents with acute lymphoblastic leukemia be treated as old children or young adults? Comparison of the French FRALLE-93 and LALA-94 trials. J Clin Oncol 2003;21(5):774-80. 14. de Bont JM, Holt B, Dekker AW. Significant difference in outcome for adolescents with acute lymphoblastic leukemia treated on pediatric vs 15. 16. 17. 18. 19. 20. 21. all tumours sarcoma brain/CNS adult protocols in the Netherlands. Leukemia 2004;18(12):2032-5. Ferrari A, Dileo P, Casanova M et al. Rhabdomyosarcoma in adults. A retrospective analysis of 171 patients treated at a single institution. Cancer 2003;98(3):571-80. Kantarjian HM, O’Brien S, Smith TL et al. Results of treatment with hyper-CVAD, a dose-intensive regimen, in adult acute lymphocytic leukemia. J Clin Oncol 2000;18(3):547-61. Ramanujachar R, Richards S, Hann I et al. Adolescents with acute lymphoblastic leukaemia: outcome on UK national paediatric (ALL97) and adult (UKALLXII/E2993) trials. Pediatr Blood Cancer 2007;48(3):254-61. Ramanujachar R, Richards S, Hann I, Webb D. Adolescents with acute lymphoblastic leukaemia: emerging from the shadow of paediatric and adult treatment protocols. Pediatr Blood Cancer 2006;47(6):748-56. U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute and the LIVESTRONG™ Young Adult Alliance. Closing the gap: Research and care imperatives for adolescents and young adults with cancer. A report of the Adolescent and Young Adult Oncology Progress Review Group. 2006. Available at http://searchosp1.nci.nih.gov/ disease/AYAO_PRG_Report_2006_FINAL.pdf Oeffinger KC, Mertens AC, Hudson MM et al. Health care of young adult survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. Ann Fam Med 2004;2(1):61-70. Retornaz F, Monette J, Batist G et al. Usefulness of frailty markers in the assessment of the health and functional status of older cancer patients referred for chemotherapy: a pilot study. J Gerontol A Biol Sci Med Sci 2008;63(5):518-22. ©2009 Parkhurst, publisher of Oncology Exchange. All rights reserved. 42 5