Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
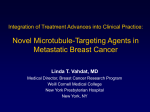
clinical review Ixabepilone clinical review Ixabepilone: A novel microtubule-stabilizing agent for the treatment of metastatic breast cancer Susan Goodin I mportant advances in the management of breast cancer include the introduction of three main classes of chemotherapeutic agents— anthracyclines, taxanes, and fluorinated pyrimidines (e.g., capecitabine)—that have improved overall outcomes for patients with metastatic disease.1-3 However, the clinical utility of these therapies has become limited in some patients by the emergence of drug resistance.4-7 The increasing use of anthracyclines and taxanes as adjuvant therapies has highlighted the need for new, effective, first-line therapies for metastatic disease.3 It has also led to the investigation of ways to overcome the problem of drug resistance in order to maximize the impact of chemotherapy on survival. The epothilone derivatives are one class of agents resulting from this research. The epothilones are microtubulestabilizing agents that have shown promising activity in patients with various cancers, including cancers resistant to taxanes and other cytotoxic drugs.7-11 Epothilones are naturally occurring macrolide compounds (i.e., containing a macrocyclic lactone ring) that constitute a novel class of cytotoxic drugs. Naturally derived epothilones have limitations such Purpose. The pharmacology, pharmacokinetics, clinical efficacy, safety, dosage, and administration of ixabepilone in patients with metastatic breast cancer are examined. Summary. The clinical utility of the three main classes of chemotherapeutic agents used in breast cancer (i.e., anthracyclines, taxanes, and fluorinated pyrimidines) is limited in some patients by the emergence of drug resistance which leads to disease progression. A recent addition to the available drugs for the treatment of advanced breast cancer is the epothilone B analog ixabepilone, which has demonstrated clinical activity in patients who have tumors that have progressed while on other chemotherapy regimens, including anthracyclines and taxanes. In Phase II clinical trials of ixabepilone in patients with metastatic breast cancer, clinically meaningful benefits have been achieved with ixabepilone monotherapy in patients in whom anthracyclines, taxanes, and capecitabine are no longer effective. Ixabepilone has demonstrated activity in first-, second-, and subsequent-lines of therapy and in different subtypes of patients with advanced disease. In a Phase III trial in patients who as metabolic instability and a low therapeutic index; therefore, a number of synthetic and semisynthetic derivatives have been developed to improve the pharmacologic proper- Susan Goodin, Pharm.D., FCCP, BCOP, is Professor of Medicine, Robert Wood Johnson Medical School, University of Medicine and Dentistry of New Jersey, Piscataway, and Director, Division of Pharmaceutical Sciences, The Cancer Center of New Jersey, 195 Little Albany Street, New Brunswick, NJ 08901 ([email protected]). Bristol-Myers Squibb provided funding to L. C. Shepherd, Ph.D., had previously received taxanes and anthracyclines, the combination of ixabepilone and capecitabine was significantly more effective in producing an objective response and in prolonging progressionfree survival than capecitabine alone. At the recommended dose and administration schedule, ixabepilone is generally well tolerated. The most clinically relevant adverse events associated with its use have been myelosuppression and peripheral neuropathy, which is primarily sensory and cumulative but reversible within six weeks of a dosage reduction or the discontinuation of therapy. Conclusion. Ixabepilone, the first drug in a new class of microtubule-stabilizing agents called epothilones, offers a new treatment option for patients with metastatic or locally advanced breast cancer who are refractory to standard chemotherapy. Index terms: Antineoplastic agents; Breast neoplasms; Capecitabine; Combined therapy; Dosage; Ixabepilone; Mechanism of action; Neoplasm metastasis; Resistance; Toxicity Am J Health-Syst Pharm. 2008; 65:2017-26 ties of naturally derived epothilones and optimize their in vivo antitumor efficacy. 12,13 Currently, three synthetic derivatives of epothilone B are in various stages of clinical de- for her editorial assistance during manuscript preparation. Copyright © 2008, American Society of Health-System Pharmacists, Inc. All rights reserved. 1079-2082/08/1101-2017$06.00. DOI 10.2146/ajhp070628 Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 2017 clinical review Ixabepilone velopment: ixabepilone, patupilone, advanced breast cancer in patients and sagopilone. One epothilone D whose tumors are resistant or refracderivative (KOS-1584) is in clinical tory to anthracyclines, taxanes, and capecitabine.14 development. This article reviews the pharmaCurrently, the only drug in this class with labeling approved by the cology, pharmacokinetics, clinical Food and Drug Administration efficacy, safety, dosage and admin(FDA) is ixabepilone (Ixempra, istration, and role in therapy of ixBristol-Myers Squibb).14 The clinical abepilone in patients with metastatic activity of ixabepilone has been dem- breast cancer. onstrated in patients with metastatic breast cancer who had previously Pharmacology As with the taxanes and other been treated with other chemotherapy regimens, including anthracy- agents that target tubulin, 21 the clines and taxanes.15-20 Ixabepilone epothilones, including ixabepilone, is indicated for use in combination bind to the b-tubulin subunits of with capecitabine for the treatment microtubules to induce microtubule of patients with metastatic or locally polymerization and stabilization, advanced breast cancer who are re- which lead to arrest of cells in the sistant to treatment with an anthra- G2-M phase of the cell cycle and cycline and a taxane, or in patients the induction of apoptosis (Figure whose cancer is resistant to taxanes 1).12,22 Epothilones bind to a tubulinbinding pocket of microtubules in and for whom further anthracycline )XABEPILONEAI therapy is contraindicated. It is also a manner that is different from that indicated for use as monotherapy for of the taxanes.23 Furthermore, their the treatment of metastatic or locally susceptibility to multidrug-resistance mechanisms also distinguishes them from the taxanes.24 Studies with ixabepilone have shown that it demonstrates antineoplastic activity against tumors that are naturally insensitive to paclitaxel or have developed resistance to paclitaxel, both in preclinical models22 and a Phase I clinical trial in patients with metastatic breast cancer.25 Pharmacokinetics Ixabepilone exhibits linear pharmacokinetics over the dosage range of 15–57 mg/m2.26 After administration, ixabepilone is rapidly distributed across a large volume (>1000 L) at steady state, indicative of extensive tissue binding (67–77% to serum proteins) and uptake.26 Ixabepilone is primarily eliminated by the liver. Over 30 metabolites of ixabepilone are produced by oxidative metabolism via cytochrome P-450 (CYP) isoenzyme 3A4, none of which have demonstrated clinically Figure 1. Mechanism of action of ixabepilone. Ixabepilone binds to the b-tubulin subunits of microtubules to induce microtubule polymerization and stabilization, which lead to G2-M arrest and the induction of apoptosis. Illustration by Taina Litwak, CMI. 0OLYMERIZEDTUBULIN SUBUNIT 3PHASE $.!SYNTHESIS )XABEPILONE 'PHASE 0REPARATION FORMITOSIS .ORMALTUBULINDISSOCIATION 'PHASE 3YNTHESISOF COMPONENTSFOR $.!SYNTHESIS -PHASE #ELLDIVISION )XABEPILONE BINDSTOTUBULIN 2ATEOFTUBULIN DISSOCIATIONREDUCED 4UBULIN MOLECULE $YNAMICSOFMICROTUBULESSUPPRESSED STATICBUNDLESOFMICROTUBULESFORM .EW RESTINGCELLS $YNAMICINSTABILITYOFMICROTUBULES IMPORTANTTO'PHASE 2018 Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 #ELLDIVISIONARRESTEDAT'-PHASE !POPTOSISINDUCED RESULTINGINCELLDEATH clinical review Ixabepilone relevant cytotoxic activity.23 Sixtyfive percent of an intravenous dose of 14[C]-ixabepilone is eliminated in the feces and 21% eliminated in the urine.26 A study of patients with mild-tosevere hepatic impairment (n = 56), as defined by bilirubin and aspartate aminotransferase (AST) levels, revealed that dosage modifications are required in this patient population. Compared with patients with normal hepatic function (n = 17), the area under the concentration-versustime curve (AUC0–∞) for ixabepilone increased by 22% in patients with either bilirubin levels of >1–1.5 times the upper limit of normal (ULN) or an AST level above the ULN but with bilirubin levels of <1.5 times the ULN. The AUC0–∞ increased by 30% in patients with bilirubin levels of >1.5–3 times the ULN and by 81% in patients with bilirubin levels of >3 times the ULN, irrespective of the AST level.27 Ixabepilone has a terminal elimination half-life of approximately 52 hours.23 With the approved dosage regimen, plasma accumulation is not expected because the length of the administration cycle is approximately 10 times that of the terminal elimination half-life.26 Clinical efficacy in metastatic breast cancer The clinical efficacy of ixabepilone, administered as either monotherapy or in combination with capecitabine, has been demonstrated across the spectrum of patients with advanced breast cancer and is described below. Anthracycline and taxanerefractor y disease. Currently, capecitabine represents the standard reference treatment for patients with metastatic breast cancer in whom anthracyclines and taxanes are no longer effective.28-31 The combination of ixabepilone and capecitabine was considered initially in these patients because of the different mechanisms of action and the demonstrated synergy of the two drugs in human xenografts.32 Therefore, the combination was investigated in an openlabel, Phase I/II study in 62 patients with metastatic breast cancer who were previously treated with a taxane and an anthracycline.33,34 In this study, the combination of ixabepilone plus capecitabine demonstrated synergistic antitumor activity and a manageable safety profile. In patients for whom response could be evaluated, the objective response rate was 30%. It was concluded that the dosage used in further studies should be ixabepilone 40 mg/m2 administered as a three-hour infusion on day 1 of each 21-day cycle with capecitabine 1000 mg/m 2 administered orally twice daily on days 1–14 of every 21-day cycle. A randomized Phase III trial of patients who had measurable locally advanced or metastatic breast cancer and were previously treated with or resistant to anthracyclines and also resistant to taxanes demonstrated that a combination of ixabepilone and capecitabine at the dosages determined from the previous trial had superior clinical efficacy to capecitabine alone (1250 mg/m2 twice daily on days 1–14 every 21 days). 19 Patients enrolled in this large, multicenter, international trial met predefined resistance criteria (Table 1). Of the 752 randomized patients, >90% had received previous chemotherapy for metastatic breast cancer (48% had one previous regimen for metastatic disease, 39% had two previous regimens, and 5% had three previous regimens). All patients were resistant to taxanes. Approximately 90% of patients had two or more metastatic sites, over 80% had visceral metastases, approximately 25% had triple-negative (estrogen receptor [ER]-negative, progesterone receptor [PR]-negative, and human epidermal growth factor receptor 2 [HER2]-negative) tumors, and 36% had progressive disease as their best response with previous taxane therapy. After a median of four (capecitabine alone) or five (ixabepilone plus capecitabine) cycles of treatment, median progressionfree survival (PFS)—the primary endpoint—was significantly greater with the combination regimen than with capecitabine alone (5.8 months versus 4.2 months, respectively; hazard ratio [HR], 0.75; 95% Confidence Interval [CI], 0.64–0.88%; p = 0.0003), as was the independent radiology review-assessed response rate (35% versus 14%, p < 0.0001). Stable disease was reported for 41% and 46% of patients receiving ixabepilone with capecitabine and capecitabine monotherapy, respectively. Significant benefit with the Table 1. Criteria Used To Define Resistance to Anthracyclines and Taxanes for Patients in Phase III Trial of Ixabepilone Treatment Definition of Resistance Anthracyclines Tumor progression of ≤3 mo after the last dose in a metastatic setting Recurrence of ≤6 mo after the last dose in a neoadjuvant or adjuvant setting Received minimum cumulative doses of doxorubicin (240 mg/m2) or epirubicin (360 mg/m2) Tumor progression of ≤4 mo after the last dose in a metastatic setting Recurrence of ≤12 mo after the last dose in a neoadjuvant or adjuvant setting Taxanes Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 2019 clinical review Ixabepilone combination regimen was consistently maintained across most predefined subgroups of patients, including those with ER/PR/HER2negative status and HER2-positive status, and those with visceral metastases.19 Overall survival data from this study are pending. A second randomized, Phase III trial comparing ixabepilone plus capecitabine with capecitabine alone in patients with advanced breast cancer previously treated with anthracyclines and taxanes has completed enrollment.35 Patients in this study did not receive more than two previous chemotherapy regimens, and those who did not receive treatment for metastatic disease must have relapsed within one year of treatment. The primary outcome measure in this trial was overall survival. The secondary outcome measured the quality of life and time to progression, objective response rate, and duration of response in patients with measurable disease. An earlier multicenter, single-arm, Phase II study investigated ixabepilone monotherapy (40 mg/m2 as a three-hour infusion every three weeks) administered to 49 patients with metastatic breast cancer who experienced disease progression while receiving taxane therapy or within 4 months of it (6 months if taxanes were used only in the adjuvant setting) and in patients who were given a taxane as their last regimen.18 Previous therapy also included an anthracycline-based regimen. An objective response rate of 12% (all partial responses) and a median time to disease progression of 2.2 months (95% CI, 1.4–3.2 months) after ixabepilone therapy were observed.18 The median survival time in these patients (86% of whom had received two or more previous chemotherapy regimens and 84% had visceral disease) was 7.9 months. Stable disease was observed in 41% of patients. Anthracycline, taxane, and capecitabine-refractory disease. In 2020 a multicenter, single-arm, Phase II study, ixabepilone monotherapy (40 mg/m2 as a three-hour infusion every three weeks) was investigated in 126 patients with metastatic breast cancer resistant to previous therapy with anthracyclines, taxanes, and capecitabine.15 Of the 126 patients enrolled, 88% had received two or more previous chemotherapy regimens in the metastatic setting, 64% had three or more metastatic sites, 77% had visceral disease, and 33% had triplenegative tumors; 113 patients were assessable for response to ixabepilone treatment. An investigator-assessed objective response rate for all treated patients was 18.3% (95% CI, 11.9– 26.1%), and an independent radiology facility-assessed response rate of 11.5% (95% CI, 6.3–18.9%) was observed.15 Fifty percent of patients in the study had stable disease during ixabepilone treatment. The median PFS was 3.1 months (95% CI 2.7–4.2 months), and the median duration of response was 5.7 months.15 Taxane-naive disease. A singlearm, Phase II study evaluated the efficacy of first-line ixabepilone monotherapy (40 or 50 mg/m2 i.v. infusion over one or three hours every three weeks) in 65 patients with metastatic breast cancer who had received one (92%) or two (8%) previous anthracycline-based adjuvant regimens.16 Although the patients were permitted to have previously received a taxane as part of an adjuvant regimen, provided one or more years had elapsed since the completion of treatment, the majority of patients (83%) had not received a taxane before enrollment. The objective response rate with ixabepilone monotherapy in this patient group was 41.5% (95% CI, 29.4–54.4%), and the median duration of response was 8.2 months (95% CI, 5.7–10.2 months). Thirty-five percent of patients had stable disease during the study, and the median overall survival time was 22 months (95% CI, 15.6–27.0 months). Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 Another single-arm, Phase II study was conducted in 23 patients with metastatic breast cancer who had not received a taxane but were permitted to have received other previous therapy (e.g., an anthracycline, capecitabine, or both), which had been received by 70% of patients.17 Ixabepilone was administered at a dosage of 6 mg/m2 by i.v. infusion over one hour on five consecutive days every three weeks. After a median of 8 cycles of ixabepilone treatment (range, 2–22 cycles), an objective response rate of 57% (95% CI, 34.5–76.8%) was achieved; 13 patients (57%) had partial responses, and 6 (26%) had stable disease. The median time to progression and response duration were 5.5 and 5.6 months, respectively. First-line therapy. A portion of the patients included in the clinical trials described received no previous chemotherapy or anthracyclines and taxanes in the adjuvant setting and were therefore treated with ixabepilone as first-line therapy in the metastatic setting. This included all 65 patients in the study who had previously been treated with an adjuvant anthracycline regimen,16 7 of 23 taxane-naive patients who had not received any previous chemotherapy and 9 of the 23 who had received adjuvant anthracycline therapy,17 and 26 of 375 patients (7%) who received ixabepilone plus capeci tabine in the randomized, Phase III study in taxane-resistant patients who had not received any previous chemotherapy. 19 Higher response rates were achieved for ixabepilone administered as first-line therapy in these studies in comparison with its use in patients receiving the drug as second-line or third-line therapy. In a subset of 55 patients treated in the randomized, Phase III study conducted by Thomas et al.,19 ixabepilone plus capecitabine maintained superiority over capecitabine alone when used as first-line therapy with regard to median PFS (7.0 months clinical review Ixabepilone versus 2.1 months; HR, 0.46; 95% CI, 0.25–0.85; p = 0.0109) and objective response rate (44% versus 10%, p = 0.0054).36 The median PFS time and objective response rate for first-line ixabepilone plus capecitabine were greater than for the corresponding results for the overall population (5.8 months and 35%, respectively), 93% of whom had received at least one previous therapy for metastatic disease.19 Combination therapy with targeted agents. Trials investigating ixabepilone in combination with targeted therapy are planned or ongoing. These include a randomized, Phase II trial comparing ixabepilone plus trastuzumab with docetaxel plus trastuzumab in patients with HER2positive locally advanced disease, metastatic disease, or both,37 and a Phase I trial of ixabepilone plus lapatinib (a dual HER1 and HER2 inhibitor) in patients with HER2-positive metastatic breast cancer.38 A randomized, Phase II, threegroup trial comparing two schedules of ixabepilone plus bevacizumab with paclitaxel plus bevacizumab as first-line therapy in patients with locally recurrent or metastatic disease is ongoing.39 Results from these trials will better define the role of ixabepilone in combination with targeted therapies. Clinical efficacy in different patient subgroups. In the clinical studies of ixabepilone, patients were enrolled regardless of their HER2 status and hormone receptor status.15,16,18,19 Patients with HER2-positive tumors were required to have previously discontinued trastuzumab. In the Phase III trial comparing ixabepilone plus capecitabine with capecitabine alone in patients with metastatic disease resistant to taxanes, analysis of PFS in prespecified patient subsets revealed that the clinical benefits of ixabepilone plus capecitabine were achieved in the majority of patient subgroups.19 There were significant differences favoring the combination regimen over capecitabine alone in relation to receptor status (notably for HER2-positive and ER/PR/ HER2-negative tumors); previous chemotherapy regimens for metastatic disease (anthracycline resistant and taxane resistant); and patient characteristics, including age (greater or less than 50 years), Karnofsky performance status, and presence of visceral disease. No data were available for patients in relation to ethnicity or the presence of liver dysfunction. Clinical trials of ixabepilone have included patients with poor prognosis, patients with triple-negative tumors, and patients with extensive and aggressive tumor burden. In three Phase II and III clinical trials of ixabepilone, patients with triplenegative tumors accounted for approximately 25–35% of the patients enrolled.15,18,19 Most of the patients enrolled in the Phase II and III studies of ixabepilone had an extensive and aggressive tumor burden, as evidenced by the high percentages of patients with visceral metastases and multiple involved disease sites.15-19 The clinical activity of ixabepilone was evident in both of these groups of patients.15-19 Complete pathological response (pCR) rate was documented in a study in which up to four cycles of ixabepilone (40 mg/m2 infused over three hours every three weeks) were administered as primary systemic (neoadjuvant) therapy to patients with invasive breast cancer (stages IIA–IIIB) before undergoing surgery (n = 164).40 A total of 29 patients achieved pCR, and of those, 17 (11%) also had pCR in the axillary lymph nodes. This response rate compares favorably with other monotherapy regimens in this population. Safety Ixabepilone demonstrated a predictable and manageable safety profile when used at the dosage and administration schedule (40 mg/ m2 i.v. over three hours every three weeks) during clinical trials, and its toxicities do not appear to overlap with those of capecitabine.15,16,18,19 In Phase II and III clinical trials, the most clinically relevant adverse events associated with ixabepilone were myelosuppression (primarily neutropenia) and peripheral neuropathy. Table 2 provides a summary of adverse events reported in Phase II clinical trials of ixabepilone monotherapy.15-18 In the Phase III trial, grade 3 or 4 neutropenia occurred in 68% of patients receiving ixabepilone plus capecitabine compared with 11% of patients receiving capecitabine alone. Febrile neutropenia was experienced by 4% of patients with the combination versus less than 1% with capeci tabine alone. Grade 3 or 4 (i.e., severe or disabling) neuropathy occurred in 23% of patients receiving the combination of ixabepilone plus capecitabine versus 0% with capecitabine alone.19 The neuropathy was primarily sensory and cumulative but was reversible with a median time to resolution of six weeks.19 Grade 3 or 4 hand–foot syndrome occurred with equal frequency in the two groups (18% versus 17%, respectively), as did grade 3 or 4 gastrointestinal disturbances such as nausea (3% versus 2%), vomiting (4% versus 2%), and diarrhea (6% versus 9%). These findings suggest that ixabepilone does not increase the hand– foot syndrome and gastrointestinal toxicity associated with capecitabine and, similarly, that capecitabine does not exacerbate neuropathy associated with ixabepilone. Neutropenia. Myelosuppression with ixabepilone primarily manifests as neutropenia. Grade 3 or 4 neutropenia occurred in 22–58% of patients in the Phase II clinical trials and in 68% of patients who received the combination of ixabepilone and capecitabine in the Phase III trial.19 Neutropenia is generally manageable by delaying ixabepilone administration and dosage reduction (Table Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 2021 clinical review Ixabepilone 3). Although some patients have required support with hematopoietic growth factors (e.g., filgrastim), such treatment was not mandated in the protocols of the clinical trials reporting these events and management was at the discretion of the treating physician.17,18 Table 2. Treatment-Related Adverse Events Reported in 10% or More of Patients in Phase II Clinical Trials of Ixabepilone Monotherapy in Metastatic Breast Cancera Adverse Eventb Nonhematologic toxicity Peripheral sensory neuropathy All Grade 3 or 4d Fatigue/asthenia All Grade 3 or 4 Myalgia/arthralgia Alopecia Nausea Stomatitis/mucositis/pharyngitis Vomiting Diarrhea Rash Musculoskeletal pain Anorexia Constipation Nail changes Fever Abdominal pain/cramping Headache Neuropathic pain Pain, other Infection without neutropenia Infection with febrile neutropenia Motor neuropathy Taste disturbance/dysgeusia Hematologic toxicity Neutropenia All Grade 3 or 4 Leukopenia All Grade 3 or 4 Anemia All Grade 3 or 4 Thrombocytopenia All Grade 3 or 4 Ref. 15 (n = 126)c No. (%) Pts Ref. 16 Ref. 17 (n = 65) (n = 23) 60 14 46 (71) 12 (52) 31 (63) 13 (20) 0 6 (12) 50 44 (68) 18 (78) 37 (76) 13 4 (6) 3 (13) 13 (27) 49 63 (97) 7 (30) 41 (84) 48 60 (92) 20 (87) 21 (43) 42 35 (54) 14 (61) 28 (57) 29 21 (32) NR 14 (28) 29 17 (26) 9 (39) 20 (41) 22 19 (29) 11 (48) 15 (31) NR 14 (22) NR 6 (12) 20 NR NR NR 19 12 (18) NR 9 (18) 16 13 (20) 13 (56) 10 (20) 9 11 (17) 13 (56) 4 (8) NR 9 (14) NR 8 (16) 13 5 (8) NR 5 (10) 11 9 (14) NR NR NR 8 (12) NR 4 (8) 8 9 (14) NR 32 (65) NR 9 (14) NR 6 (12) NR 4 (6) 0 3 (6) 10 4 (6) 2 (9) NR 6 7 (11) 15 (65) NR 79 54 57 (89) 20 (87) 37 (58) 5 (22) 90 49 60 (92) 32 (50) 84 60 (92) 19 (83) 3 (6) 8 2 (3) 0 2 (4) 44 26 (40) 12 (52) 8 0 1 (4) b Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 NR 53c NR 3 (6) NR 1 (2) NR = not reported. All toxicity grades unless otherwise noted. c This report did not include number of patients corresponding to the percentages listed. d Based on National Cancer Institute Common Toxicity Criteria. a 2022 Ref. 18 (n = 49) NR NR The incidence of febrile neutropenia reported in Phase II and III trials has been low (Table 2).16,18,19 Peripheral sensory neuropathy. Neuropathy is a characteristic adverse event of microtubule-stabilizing agents.42 The peripheral sensory neuropathy reported in clinical trials of ixabepilone has primarily been mild to moderate in severity and mostly reversible within an acceptable time frame (median time to resolution, six weeks).19 Grade 3 or 4 neuropathy occurred in 0–20% of patients treated with ixabepilone monotherapy in Phase II trials (Table 2) and 23% of patients treated with ixabepilone plus capecitabine in the Phase III trial.19 It has been postulated that less peripheral neuropathy may occur with ixabepilone when used as firstline therapy in taxane-naive patients, but this remains to be confirmed.39 There are no proven treatments for peripheral neuropathy associated with microtubule-stabilizing agents.41 It is not possible to predict the occurrence of this adverse event; therefore, health care team members who care for patients receiving ixabepilone should be aware of the onset of symptoms (i.e., burning sensation, hyperesthesia, hypoesthesia, paresthesia, discomfort, and neuropathic pain) and take appropriate action, including delayed administration of the next dose and dosage reduction. Treatment should not be restarted until neuropathy has returned to baseline or is a grade 1 or lower in severity. Management of other adverse events. As the ixabepilone infusion solution contains Cremophor EL, which may cause hypersensitivity reactions in some patients, premedication with antihistamines (i.e., both histamine H 1 -receptor and H 2 receptor antagonists) is necessary to reduce the risk of such reactions.16 However, in contrast to premedication for taxanes,42,43 corticosteroid premedication is not required with ixabepilone unless the patient has clinical review Ixabepilone had a hypersensitivity reaction to a previous administration of the drug. In addition to dosage adjustments and delay in administration, supportive care interventions may be required for specific adverse events associated with ixabepilone administered with or without capeci tabine.42,44 Interventions that may be considered include the following: analgesics for myalgia and arthralgia, anesthetic mouthwashes for the treatment of stomatitis or mucositis, antiemetics for nausea and vomiting, emollients for hand–foot syndrome due to capecitabine in combined regimens, and antidiarrheals and fluid replacement for diarrhea (prophylactic antibiotics may be indicated for patients with diarrhea and neutropenia). Dosage and administration Multiple doses and schedules of ixabepilone were evaluated during the clinical development of the drug.8 Initially, dosages as high as 50 mg/ m2 every three weeks were evaluated; however, the severity and extent of the neuropathy forced a lowering of the dosage for further evaluation to the current recommended dosage.8,34 Other dosage schedules have also been evaluated, including ixabepilone 6 mg/m2 daily for five days every three weeks showing activity and tolerability in women who never received taxanes before taking ixabepilone.17 However, the ixabepilone dosage recommended by the manufacturer is 40 mg/m2 administered i.v. over three hours every three weeks. Dosages for patients with a body surface area greater than 2.2 m2 should be calculated based on 2.2 m2.26 Dosage adjustments for toxicities. If toxicities are detected during treatment, therapy should be delayed to allow recovery.26 Dosage adjustment guidelines for ixabepilone monotherapy and combination therapy are shown in Table 3. Dosage adjustments at the start of a cycle should be based on toxicity assessments from the preceding cycle. Patients should not begin a new cycle of treatment unless the neutrophil count is ≥1,500 cells/mm3, the platelet count is ≥100,000 cells/mm3, and nonhematologic toxicities have resolved or improved to grade 1 (mild). If toxicities recur, an additional 20% dose reduction is required.26 Dosage adjustments in patients with hepatic impairment. Patients with hepatic impairment should receive ixabepilone based on the guidelines in Table 3. In the case of ixabepilone monotherapy, patients with moderate hepatic impairment should be started at 20 mg/m2. The dosage in subsequent cycles may be adjusted upward to, but not exceeding, 30 mg/m2 if tolerated. Use of ixabepilone is not recommended in patients with AST or alanine aminotransferase (ALT) levels more than 10 times the ULN or bilirubin levels Table 3. Ixabepilone Dosage Adjustments for Toxicities and in the Presence of Hepatic Impairment or Coadministration of Other Drugs26 Condition Nonhematologic toxicitya Grade 2 neuropathy (moderate) lasting ≥7 days Grade 3 neuropathy (severe) lasting <7 days Grade 3 neuropathy (severe) lasting ≥7 days or disabling neuropathy Any grade 3 toxicity (severe) Transient grade 3 arthralgia/myalgia or fatigue Grade 3 hand-foot syndrome Any grade 4 toxicity (disabling) Hematologic toxicity Neutrophils <500 cells/mm3 for ≥7 days Febrile neutropenia Platelets <25,000/mm3 or platelets <50,000/mm3 with bleeding Hepatic impairment Ixabepilone monotherapy AST and ALT conc. ≤2.5 × ULN and bilirubin conc. ≤1 × ULN AST and ALT conc. ≤10 × ULN and bilirubin conc. ≤1.5 × ULN AST and ALT conc. ≤10 × ULN and bilirubin conc. >1.5 × ULN – ≤3 × ULN Ixabepilone and capecitabine combination therapy AST or ALT conc. >2.5 × ULN or bilirubin conc. >1 × ULN Coadministration with other drugs Potent inhibitors of CYP3A4b Suggested Ixabepilone Dosage Adjustment Decrease dose by 20% Decrease dose by 20% Discontinue treatment Decrease dose by 20% No change in dose required No change in dose required Discontinue treatment Decrease dose by 20% Decrease dose by 20% Decrease dose by 20% Recommended dose: 40 mg/m2 Recommended dose: 32 mg/m2 Recommended dose: 20–30 mg/m2 Contraindicated Starting dose: 20 mg/m2 Toxicities graded in accordance with the National Cancer Institute Common Toxicity Criteria for adverse events. ALT = alanine aminotransferase, AST = aspartate aminotransferase, CYP3A4 = cytochrome P-450 isoenzyme 3A4, ULN = upper limit of normal. b Inhibits oxidative metabolism of ixabepilone and may significantly increase exposure to the drug. Examples of potent CYP3A4 inhibitors include ketoconazole, itraconazole, clarithromycin, atazanavir, nefazodone, saquinavir, telithromycin, ritonavir, amprenavir, indinavir, nelfinavir, delavirdine, and voriconazole. a Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 2023 clinical review Ixabepilone more than 3 times the ULN. Limited data are available for patients with baseline AST or ALT levels more than 5 times the ULN. Caution should be used when treating these patients.26 Patients receiving combination treatment who have AST and ALT levels less than or equal to 2.5 times the ULN and bilirubin levels less than or equal to 1 time the ULN may receive the standard dose of ixabepilone (40 mg/m2).26 Dosage adjustments in patients receiving CYP3A4 isoenzyme inhibitors. The use of concomitant potent CYP3A4 inhibitors (e.g., ketoconazole) should be avoided. Grapefruit juice may also increase plasma concentrations of ixabepilone and should also be avoided. Guidelines to follow in the event that a potent CYP3A4 inhibitor must be coadministered are given in Table 3. If a potent CYP3A4 inhibitor is discontinued, approximately one week of washout should be allowed before escalating the ixabepilone dose.26 The effect of mild or moderate CYP3A4 inhibitors (e.g., erythromycin, fluconazole, verapamil) on ixabepilone pharmacokinetics has not been studied; thus, caution should be used when mild or moderate CYP3A4 inhibitors are administered in patients receiving ixabepilone. Premedication. To minimize the risk of a hypersensitivity reaction, all patients must be premedicated approximately one hour before the infusion of ixabepilone with an H1receptor antagonist (e.g., diphenhydramine hydrochloride 50 mg orally) and an H2-receptor antagonist (e.g., ranitidine 150–300 mg orally).26 Patients who have had a previous hypersensitivity reaction to ixabepilone require corticosteroid premedication (e.g., dexamethasone phosphate 20 mg i.v. 30 minutes before infusion or dexamethasone 20 mg orally 60 minutes before infusion) in addition to pretreatment with H1and H2-antagonists.26 2024 Preparation and administration. Ixabepilone is supplied as two vials, one containing ixabepilone powder and another containing mandatory diluent. Only the supplied diluent must be used for constituting ixabepilone for injection. To minimize the risk of dermal exposure, impervious gloves should be worn when handling vials containing ixabepilone.26 Both vials must be stored under refrigeration at 2–8 °C (36–46 °F) in the original package to protect them from light. Before reconstitution, the vials should be placed at room temperature for 30 minutes. When the diluent is first removed from the refrigerator, a white precipitate may be seen but will dissolve to form a clear solution once the diluent warms to room temperature. After reconstitution, the concentration of ixabepilone is 2 mg/mL. The solution may be stored in the vial, not the syringe, for a maximum of one hour at room temperature and room lighting conditions.26 Before administration, the solution must be further diluted only with Lactated Ringer’s Injection, USP, supplied in di(2-ethylhexyl) phthalate-free bags. This diluent is specified because it has a pH range of 6.0–7.5, which is required to maintain ixabepilone’s stability. Other diluents should not be used. The final ixabepilone concentration for infusion must be 0.2–0.6 mg/mL. This solution is stable at room temperature and light for a maximum of six hours. Administration of diluted ixabepilone must therefore be completed within this period.26 Role in therapy Ixabepilone is the first semisynthetic epothilone B analog with labeling approved by FDA and represents an important addition to the current armamentarium of drugs for the treatment of metastatic and locally advanced breast cancer. In patients with metastatic breast cancer, Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 ixabepilone has demonstrated a lack of complete cross-resistance with other drugs used to treat advanced breast cancer.15,18,19 Clinically meaningful benefits have been achieved with ixabepilone monotherapy in patients in whom anthracyclines, taxanes, and capecitabine all failed to provide a response.15 The synergistic activity of a combination of ixabepilone and capecitabine has been confirmed in a Phase III trial in patients who had previously failed on taxanes and anthracyclines; a combination of ixabepilone and capecitabine was significantly more effective in producing an objective response and in prolonging PFS than capecitabine alone.19 At the dosage and administration schedule recommended by the manufacturer in patients meeting the eligibility criteria for treatment, the therapeutic ratio of ixabepilone is generally favorable, and adverse events are generally manageable and reversible. Ixabepilone has demonstrated activity in HER2-positive and HER2negative patients. In the Phase III trial, 9% of patients in the ixabepilone plus capecitabine group had received previous trastuzumab therapy and 16% were HER2-positive.19 For patients with advanced breast cancer who have progressed following trastuzumab treatment, a combination of lapatinib plus capecitabine is a viable treatment option. The physician can determine whether a patient with resistance is still a candidate for anti-HER2 therapy. However, clinical trials are underway to investigate the potential of combining ixabepilone plus trastuzumab or lapatinib for the treatment of breast cancer. Chemotherapy remains the treatment of choice for patients with hormone-unresponsive or hormoneresistant metastatic breast cancer, HER2-negative tumors, extensive visceral disease, or life-threatening and rapidly progressing disease. 3 The profiles of patients enrolled in completed clinical trials that have clinical review Ixabepilone included patients previously treated with anthracyclines and taxanes across multiple lines of therapy for metastatic breast cancer provide guidance on the indications for the use of ixabepilone and may help select patients who will likely benefit from ixabepilone therapy.39 On the basis of the results of these trials, appropriate indications for ixabepilone can be suggested. These indications include first-line, second-line, thirdline, or higher therapies in patients with metastatic breast cancer previously treated with or resistant to anthracycline therapy, taxane therapy, or both18,19,35; first-line therapy in patients with metastatic breast cancer previously treated with anthracyclines or taxanes in the adjuvant setting16; and third- or fourth-line therapy in patients with metastatic disease previously treated with anthracyclines, taxanes, and capeci tabine. 15 In addition, ixabepilone has been evaluated in patients whose disease progressed during treatment with anthracyclines because of resistance (progressive disease) or patients who reached the maximum cumulative dose of anthracyclines. Patients in these categories have been evaluated in a clinical trial that compared ixabepilone plus capecitabine with capecitabine alone.34 Significant efforts are ongoing to identify predictive and prognostic biomarkers to identify patients who are most likely to respond to ixabepilone treatment. Although initial results suggest that certain biomarkers (e.g., ER status, expression of the microtubule-associated protein tau) and gene signatures are predictive of responsiveness to ixabepilone; however, these findings have not been fully validated.40,45 Some patients may be at an increased risk for adverse events and may not be candidates for therapy with ixabepilone or may require treatment using a reduced dosage of ixabepilone. These include patients with abnormal liver function tests (AST or ALT levels more than 2.5 times the ULN or bilirubin levels more than 1 time the ULN), who may be at increased risk of treatmentrelated mortality.19 In these patients, the dosage of ixabepilone given as monotherapy should be reduced according to the degree of hepatic impairment. Use of ixabepilone as monotherapy is not recommended in patients with AST or ALT levels more than 10 times the ULN or bilirubin levels more than 3 times the ULN, and the combination of ixabepilone with capecitabine is contraindicated in patients with AST or ALT levels more than 2.5 times the ULN or bilirubin levels more than 1 time the ULN. The use of ixabepilone is also not recommended in patients with a neutrophil count of less than 1,500 cells/ mm3, a platelet count of less than 100,000/mm3, or preexisting peripheral neuropathy of grade 2 or higher. Patients with neuropathy of grade 2 or higher were not eligible for enrollment in clinical trials of ixabepilone. Ixabepilone should be administered with caution to patients with coexisting medical conditions associated with peripheral neuropathy such as diabetes mellitus or a substantial history of alcohol use, who also appear to be prone to neurotoxicity with paclitaxel.39,46 Patients with diabetes mellitus treated with ixabepilone may be at increased risk of severe neuropathy. Caution is also warranted in patients receiving treatment with other drugs that are potent inhibitors of CYP3A4 isoenzymes (i.e., ketoconazole, itraconazole, clarithromycin, atazanavir, nefazodone, saquinavir, telithromycin, ritonavir, amprenavir, indinavir, nelfinavir, delavirdine, or voriconazole).26 Since oxidative metabolism by CYP3A4 and CYP3A5 appears to be a prominent route of biotransformation of ixabepilone, concomitant administration of CYP3A4 inhibitors may significantly increase exposure to the drug. In such cases, the starting dose should be reduced. In addition, use of ixabepilone is not recommended in patients with a history of hypersensitivity to drugs formulated with Cremophor EL because ixabepilone infusion solution is formulated with this compound. Ixabepilone is indicated in combination with capecitabine for the treatment of metastatic or locally advanced breast cancer in patients refractory to anthracycline and taxane therapy, and as monotherapy for the treatment of metastatic or locally advanced breast cancer in patients after failure of an anthracycline, a taxane, and capecitabine. As well as demonstrating benefits in anthracycline- and taxane-pretreated patients, ixabepilone appears to be effective across all lines of therapy and in different subtypes of breast cancer patients with extensive or aggressive disease. Future studies will further define the role of ixabepilone in relation to the taxanes and other drugs used in the treatment of breast cancer. Conclusion Ixabepilone, the first drug in a new class of microtubule-stabilizing agents called epothilones, offers a new treatment option for patients with metastatic or locally advanced breast cancer who are refractory to standard chemotherapy. References 1. Gennari A, Conte P, Rosso R et al. Survival of metastatic breast carcinoma patients over a 20-year period: a retrospective analysis based on individual patient data from six consecutive studies. Cancer. 2005; 104:1742-50. 2. Hamilton A, Hortobagyi G. Chemotherapy: what progress in the last 5 years? J Clin Oncol. 2005; 23:1760-75. [Erratum. J Clin Oncol. 2006; 23:5851.] 3. Colozza M, De Azambuja E, Personeni N et al. Achievements in systemic therapies in the pregenomic era in metastatic breast cancer. Oncologist. 2007; 12:253-70. 4. Longley DB, Johnston PG. Molecular mechanisms of drug resistance. J Pathol. 2005; 205:275-92. 5. Lee JJ, Swain SM. Development of novel chemotherapeutic agents to evade the Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 2025 clinical review Ixabepilone 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. mechanisms of multidrug resistance (MDR). Semin Oncol. 2005; 32(suppl 7):S22-6. Clarke R, Leonessa F, Trock B. Multidrug resistance/P-glycoprotein and breast cancer: review and meta-analysis. Semin Oncol. 2005; 32(suppl 7):S9-15. Fornier MN. Epothilones in breast cancer: review of clinical experience. Ann Oncol. 2007; 18(suppl 5):v16-21. Goodin S, Kane M, Rubin EH. Epothilones: mechanism of action and biological activity. J Clin Oncol. 2004; 22:201525. Aghajanian C, Burris HA, Jones S et al. Phase I study of the novel epothilone analog ixabepilone (BMS-247550) in patients with advanced solid tumors and lymphomas. J Clin Oncol. 2007; 25:10828. Dawson NA. Epothilones in prostate cancer: review of clinical experience. Ann Oncol. 2007; 18(suppl 5):v22-7. Larkin JM, Kaye SB. Potential clinical application of epothilones: a review of phase II studies. Ann Oncol. 2007; 18(suppl 5):v28-34. Fumoleau P, Coudert B, Isambert N et al. Novel tubulin-targeting agents: anticancer activity and pharmacologic profile of epothilones and related analogues. Ann Oncol. 2007; 18(suppl 5):v9-15. Altmann KH, Pfeiffer B, Arseniyadis S et al. The chemistry and biology of epothilones—the wheel keeps turning. ChemMedChem. 2007; 2:396-423. Cortes J, Baselga J. Targeting the microtubules in breast cancer beyond taxanes: the epothilones. Oncologist. 2007; 12:271-80. Perez EA, Lerzo G, Pivot X et al. Efficacy and safety of ixabepilone (BMS-247550) in a phase II study of patients with advanced breast cancer resistant to an anthracycline, a taxane, and capecitabine. J Clin Oncol. 2007; 25:3407-14. Roché H, Yelle L, Cognetti F et al. Phase II clinical trial of ixabepilone (BMS247550), an epothilone B analog, as firstline therapy in patients with metastatic breast cancer previously treated with anthracycline chemotherapy. J Clin Oncol. 2007; 25:3415-20. Denduluri N, Low JA, Lee JJ et al. Phase II trial of ixabepilone, an epothilone B analog, in patients with metastatic breast cancer previously untreated with taxanes. J Clin Oncol. 2007; 25:3421-7. Thomas E, Tabernero J, Fornier M et al. Phase II clinical trial of ixabepilone (BMS-247550), an epothilone B analog, in patients with taxane-resistant metastatic breast cancer. J Clin Oncol. 2007; 25:3399-406. Thomas E, Gomez HL, Li RK et al. Ix abepilone plus capecitabine for metastatic breast cancer progressing after anthracycline and taxane treatment. J Clin Oncol. 2007; 25:5210-7. Low JA, Wedam SB, Lee JJ et al. Phase II clinical trial of ixabepilone (BMS247550), an epothilone B analog, in 2026 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. metastatic and locally advanced breast cancer. J Clin Oncol. 2005; 23:2726-34. Rowinsky EK, Calvo E. Novel agents that target tubulin and related elements. Semin Oncol. 2006; 33:421-35. Lee FY, Borzilleri R, Fairchild CR et al. BMS-247550: a novel epothilone analog with a mode of action similar to paclitaxel but possessing superior antitumor efficacy. Clin Cancer Res. 2001; 7:142937. Nettles JH, Li H, Cornett B et al. The binding mode of epothilone A on alpha, beta-tubulin by electron crystallography. Science. 2004; 305:866-9. Brooks TA, Minderman H, O’Loughlin KL et al. Taxane-based reversal agents modulate drug resistance mediated by P-glycoprotein, multidrug resistance protein, and breast cancer resistance protein. Mol Cancer Ther. 2003; 2:1195-205. [Erratum. Mol Cancer Ther. 2004; 3:101.] McDaid HM, Mani S, Shen HJ et al. Validation of the pharmacodynamics of BMS-247550, an analogue of epothilone B, during a phase I clinical study. Clin Cancer Res. 2002; 8:2035-43. Ixabepilone package insert. Princeton, NJ: Bristol-Myers Squibb; 2007 Oct. Takimoto CH, Liu PY, Lenz H et al. A phase I pharmacokinetic study of the epothilone B analogue, ixabepilone (BMS-247550) in patients with advanced malignancies and varying degrees of hepatic impairment. A SWOG early therapeutics committee and NCI organ dysfunction working group trial. J Clin Oncol. 2006; 24(suppl 18S). Abstract. Blum JL, Jones SE, Buzdar AU et al. Multicenter phase II study of capecitabine in paclitaxel-refractory metastatic breast cancer. J Clin Oncol. 1999; 17:485-93. Blum JL, Dieras V, Lo Russo PM et al. Multicenter, phase II study of capeci tabine in taxane-pretreated metastatic breast carcinoma patients. Cancer. 2001; 92:1759-68. Reichardt P, Von Minckwitz G, ThussPatience PC et al. Multicenter phase II study of oral capecitabine (Xeloda) in patients with metastatic breast cancer relapsing after treatment with a taxanecontaining therapy. Ann Oncol. 2003; 14:1227-33. Fumoleau P, Largillier R, Clippe C et al. Multicentre, phase II study evaluating capecitabine monotherapy in patients with anthracycline- and taxane-pretreated metastatic breast cancer. Eur J Cancer. 2004; 40:536-42. Lee FY, Camuso A, Castenada S et al. Preclinical efficacy evaluation of ixabepilone (BMS-247550) in combination with cetuximab or capecitabine in human colon and lung carcinoma xenografts. 2006 ASCO annual meeting proceedings part I. J Clin Oncol. 2006; 24(suppl):12017. Bunnell CA, Klimovsky J, Thomas E. Final efficacy results of a phase I/II trial of ixabepilone in combination with capeci tabine in patients with metastatic breast cancer (MBC) previously treated with a Am J Health-Syst Pharm—Vol 65 Nov 1, 2008 taxane and an anthracycline. 2006 ASCO annual meeting proceedings part I. J Clin Oncol. 2006; 24(suppl):10511. 34. Vahdat LT, Klimovsky J, Bunnell C. Phase I/II trial in patients with metastatic breast cancer (MBC) previously treated with a taxane and an anthracycline: final safety data. 2006 ASCO annual meeting proceedings part I. J Clin Oncol. 2006; 24(suppl):10528. 35. ClinicalTrials.gov. Epothilone (ixabepilone) plus capecitabine versus capeci tabine alone in patients with advanced breast cancer. www.clinicaltrials.gov/ct2/ show/NCT00082433?term=nct00082433 &rank=1 (accessed 2008 Aug 5). 36. Jassem J, Thomas E, Gomez H et al. Phase III study of ixabepilone plus capecitabine in patients with metastatic breast cancer (MBC) progressing after anthracyclines and taxanes: subgroup analysis of patients receiving ixabepilone in the firstline setting. Eur J Cancer. 2007; 5:213. Abstract. 37. ClinicalTrials.gov. A Phase II combination of trastuzumab and ixabepilone versus trastuzumab and docetaxel in patients with advanced and/or metastatic breast cancer. www.clinicaltrials.gov/ct2/show/ NCT00490646?term=NCT00490646& rank=1 (accessed 2008 Aug 4). 38. ClinicalTrials.gov. Phase I study of ixabepilone + lapatinib +/- capecitabine to treat HER2 positive locally advanced or metastatic breast cancer. www. clinicaltrials.gov/ct2/show/NCT0063408 8?term=phase+1+trial+of+ixabepilone+ her2&rank=1 (accessed 2008 Aug 4). 39. ClinicalTrials.gov. A trial of 2 schedules of ixabepilone plus bevacizumab and paclitaxel plus bevacizumab for breast cancer. www.clinicaltrials.gov/ct2/show/NCT0 0370552?term=NCT00370552&rank=1 (accessed 2008 Aug 4). 40. Gianni L. Ixabepilone and the narrow path to developing new cytotoxic drugs. J Clin Oncol. 2007; 25:3389-91. 41. Lee JJ, Swain SM. Peripheral neuropathy induced by microtubule-stabilizing agents. J Clin Oncol. 2006; 24:1633-42. 42. Markman M. Management of toxicities associated with the administration of taxanes. Expert Opin Drug Saf. 2003; 2:141-6. 43. Lenz HJ. Management and preparedness for infusion and hypersensitivity reactions. Oncologist. 2007; 12:601-9. 44. Marse H, Van Cutsem E, Grothey A et al. Management of adverse events and other practical considerations in patients receiving capecitabine (Xeloda). Eur J Oncol Nurs. 2004; 1(suppl 8):S16-30. 45. Lee H, Xu L, Wu S et al. Predictive biomarker discovery and validation for the targeted chemotherapeutic ixabepilone. 2006 ASCO annual meeting proceedings part I. J Clin Oncol. 2006; 24(suppl):3011. 46. Rowinsky EK, Eisenhauer EA, Chaudhry V et al. Clinical toxicities encountered with paclitaxel (Taxol). Semin Oncol. 1993; 20(4, suppl 3):1-15.