Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
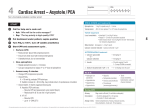
Emergency & Rapid Response Team Tools What is my role on the Rapid Response Team (RRT)? Whether in a small rural clinic or at a large county hospital, your expertise as a pharmacist is invaluable during a code. Your contribution can be a crucial part of saving an individual's life and you will be depended on (by the rest of the team) in the following ways: To identify appropriate drug therapies and make recommendations To provide correct medication dosages and limits To prepare the necessary medications/solutions Attending a Code 1. 2. 3. 4. Identify yourself and offer to handle medications Remove the medication tray from the crash cart Prepare all medications/solutions for the appropriate route of administration Provide drug information and recommendations as needed– Check patient’s allergies, age, height, 5. Ensure that the correct medication is being dispensed 6. Help code recorder keep track of medications used Click ➲ to open the original resource and explore more. ACLS Basics ➲ Normal Sinus Rhythm Heart rate: 60-100 beats per minute ECG Waves: P wave preceding QRS triplet. QRS narrow with positive P wave. Systole blood pressure: 90-120 Diastole blood pressure: 60-80 Respiratory rate: 12-18 breaths/min Normal O2 saturation: 90% or more Bradycardia Symptoms: heart rate less than 50 beats/min, chest discomfort/pain, SOB, decreased consciousness, weakness, light-headedness, presyncope or syncope Treatment: Atropine. 0.5 mg rapid IV bolus every 3 to 5 minutes. Max dose of 3 mg. Tachycardia Symptoms: heart rate greater than 100 beats/min, pain, decreased parasympathetic activity, sympathetic activation, hypotention, fever, hypoxia. Treatment: Correct underlying causes. If stable and no correctable cause, use vagal maneuvers and consider adenosine. (Initial dose = 6 mg rapid IV bolus + 20 mL normal saline flush. Try adenosine 12 mg twice if no improvement, with saline after each dose as described.) Cardiac Arrest: Ventricular Fibrillation (VF) OR Pulseless Ventricular Tachycardia (VTach) 1. 2. 3. 4. 5. 6. Management High Energy Shock CPR High Energy Shock (if indicated) CPR + Epinephrine (1 mg IV every 3 to 5 mins) High Energy Shock (in indicated) CPR + Amiodarone (Initial dose = 300 mg IV bolus; Second dose = 150 mg IV) Cardiac Arrest: Asystole OR Pulseless Electrical Activity (PEA) Management 1. CPR 2. Epinephrine* (1 mg IV every 3 to 5 minutes) 3. Rhythm check (if not shockable rhythm then continue CPR) 4. CPR 5. Epinephrine* 6. Rhythm check *Vasopressin may replace the first or second Epinephrine dose. Use 40 unites IV. Other Code Actions ➲ Compromised Airway All sizes of airways (may need in case of seizure) McGill forceps large and small to retrieve foreign object obstructing airway Respiratory Distress Nasal Canula for Infant, Pedi, Adult 100% non-rebreather masks for Infant, Pedi, Adult O2 ‘E’ cylinder with key, flow adapter, and Christmas tree (to connect to tubing) Respiratory Arrest Pocket Mask Ambu Bag for Infant, Pedi, Adult O2 ‘E’ cylinder with key, flow adapter, and Christmas tree (to connect to tubing) (Consider: Laryngoscope handles and blades, all sizes of ET tubes) “ACS” Acute Cardiac Syndrome Aspirin: chew one 325mg tab Nitroglycerin tab (gr. 0.4) sublingual every 5 minutes till relief achieved (max 3 tabs) 100% non-rebreather face mask at minimum 10-15 liters/min Establish IV access (Normal Saline at kvo rate) Cardiac Arrest A – B – Cs AED application (Turn on unit – Place pads – Allow to analyze – If advised, deliver shock) CPR Establish IV access (Normal Saline at kvo rate) Epinephrine 1 mg IVPush (1:10,000 conc) Continue with ACLS protocols to extent possible until EMS arrives Drug Overdose or Unresponsive Patient (becomes unresponsive for unknown reason) A – B – Cs Establish IV access (Normal Saline at kvo rate) Administer Narcan 1 mg IVP (max: 2 mg) Hypoglycemia Establish IV access (Normal Saline at kvo rate) Administer 25 mls D50, may repeat another 25 mls Anaphylactic Reaction (acute allergic response) Establish IV access (Normal Saline at kvo rate) EpiPen or EpiPen Jr. for children less than 30 kilograms Benadryl 50 mg IVPush for adult Pepcid 20 mg IV piggyback (mixed in 50 ml normal saline, D5WOLR) SoluMedrol 125 mg IVPush for adult A – B – Cs Standard Crash Cart Medications 1. Aspirin 325 mg tabs 2. Nitroglycerin 0.4 mg sublingual tabs 3. Dextrose 50% 50 ml. 4. Narcan 1 mg Amp 5. Epinephrine 1 mg, (1:10:000 conc) 6. Atropine Sulfate 0.1 mg/ml 7. Lidocaine 100mg 8. EpiPen 9. EpiPen Jr. (for child less that 30 kilograms) 10. SoluMedrol 125 mg Vial 11. Benadryl 50 mg Vial 12. Pepcid 20 mg Vial (per 2010 ACLS guidelines) Need extra practice? Take practice quizes to test your knowledge of ACLS https://www.acls.net/quiz.htm Watch ACLS review and tutorial videos http://acls-algorithms.com/acls-video-review Resources/Credit 1. http://www.ucdmc.ucdavis.edu/cppn/resources/clinical_skills_refresher/crash_car t/top_drawer.html 2. http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=7&ved=0CD YQFjAG&url=http%3A%2F%2Fwww.ttuhsc.edu%2Fprovost%2Fclinic%2Fforms %2FACForm2.03.A.pdf&ei=lPMXU_DRJYisyAHInYDgAQ&usg=AFQjCNG1nEv8 kxpAJAzxU6ERHrLZmqaucA&sig2=Z3LSiqpExa3Lj_RJzebvA&bvm=bv.62577051,d.aWc