Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
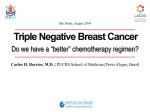
Distinct biomarker features in triple-negative breast cancer metastases to the brain, liver and bone Joanne Xiu1, Zoran Gatalica1, Sandeep Reddy1, James Waisman2, John Link3 1Caris Life Sciences, Phoenix, AZ, United States, 85040; 2City of Hope Medical Oncology, Duarte, CA, United States, 91010 and 3Breastlink Medical Group, Orange, CA, United States, 92868. Abstract Background: Triple-negative breast cancer (TNBC) is characterized by its aggressive nature and accounts for a disproportionate number of metastatic disease cases and breast cancer-related deaths. Despite recent improvements, TNBC patients who develop metastatic diseases have limited treatment options. We investigated biomarkers from brain, liver and bone metastases collected from TNBC patients to identify therapeutic options and to examine molecular differences between the metastatic sites. Method: Triple-negative breast cancer tumors referred to Caris Life Sciences (Phoenix, AZ) between 2009 and 2015 were tested with a combination of immunohistochemistry (IHC), fluorescent/chromogenic in-situ hybridization (FISH/CISH) and sequencing (Next-generation sequencing, or NGS and Sanger). Result: 1570 TNBC tumors were analyzed, including 1297 tumors taken from breast, 54 from brain, 172 from liver and 47 from bone. Select biomarker frequencies of protein overexpression (IHC), gene amplification (ISH) and mutations (SEQ) are summarized in Table 1. Brain metastases showed the highest protein expression of TOPO2A and PDL1; liver metastases showed the highest expression of AR and SPARC, as well as the highest mutation rate of PIK3CA. Bone metastases showed the lowest expression of TS, RRM1 and ERCC1. BRCA1 and BRCA2 mutation rates ranged from 0-11% in various specimen sites. Table 1 Biomarker And Method TOPO2A IHC PDL1 IHC AR IHC SPARC IHC PIK3CA SEQ TS IHC* RRM1 IHC* ERCC1 IHC* BRCA1 SEQ BRCA2 SEQ Breast specimens (%) 76 15 15 17 16 49 39 35 7 11 Brain Metastases (%) 100 40 10 30 5.3 54 43 55 0 11 Liver Metastases (%) 73 8 36 40 29 24 32 48 8 4 Bone Metastases (%) 39 17 26 15 25 15 16 16 0 0 P value$ <0.0001 0.03 0.0005 0.0027 0.036 <0.0001 0.006 0.002 ns ns Results Background TNBC is known for its highly aggressive behavior and resistance to current standard therapies. It’s is a well-defined subtype of breast cancer immunohistochemically however it remains a molecularly heterogeneous group (1). Clinical data suggest that TNBC patients with metastases to different organs experience different survival times however different responses to therapies haven’t been systematically explored (2). Multiplex tumor-profiling has shown to effectively prolong patients’ progression-free survival in metastatic heavily pretreated breast cancer (3), therefore we investigated the profiles in TNBC tumors with different metastases. Methods Results: 60% Brain Mets TNBC Breast specimen - TNBC 50% 100.0% N (NGS) Av. Age Age InterQuartile Range TNBC 7.9% IHC-PD-L1 p=0.0266 Immune checkpoint inhibitors 40.0% 15.3% 50.3% Low IHC-PTEN p=0.0382 Breast specimens 45.5% (N=1297) 484 54.6 yrs 47-64 yrs (N=54) (N=172) (N=47) 10 52.3 yrs 45-59 yrs 62 55.6 yrs 48-63 yrs 9 57.7 yrs 51-65 yrs 10% 15% p=0.0438 15% 13% 8% 8% 9% 6% 3% 8% 5% 5% 2% 2% 2% 3% 0% Irinotecan 74.5% IHC-TOPO1 p=0.0004 66.0% Most prevalent in TNBC-brain mets 56.3% 14.6% 43.0% IHC-TLE3 p=0.0009 28.3% 33.6% 15.0% Taxanes Agents most likely to benefit TNBC liver mets Taxanes 40.0% IHC-SPARCp 29.5% 17.1% p=0.0027 26.1% Bicalutamide, enzalutamide 36.5% IHC-AR p=0.0005 10.4% 15.3% 85.1% 76.4% Low IHC-TS p<0.0001 Fluropyrimidines 45.8% 51.0% 68.4% Gemcitabine 57.4% 61.0% 52.4% 45.5% Platinums 65.0% 50.0% Low IHC-TUBB3 p=0.0009 Brain metastases 20% PI3K/Akt/mTor inhibitors 67.3% 29% 58.0% 81.3% TNBC Bone metastases Agents most likely to benefit TNBC brain mets 61.7% Low IHC-ERCC1 p=0.0018 TNBC Liver metastases Bone mets -TNBC p=0.0355 30% 76.6% 40.0% 37.8% 5.6% 10.2% 5.6% 7.2% IHC-cMET TNBC Liver mets - TNBC Top2A inhibitors 73.4% 83.9% (N=1570) Brain mets -TNBC 40% 39.3% Low IHC-RRM1 p=0.0059 TNBC Breast specimens-TNBC Liver Mets - TNBC 84.4% Figure 1: Patient Characteristics 85% 80% Bone Mets -TNBC 16.7% IHCs were performed on formalin-fixed paraffin-embedded (FFPE) tumor samples using commercially available detection kits, automated staining techniques (Benchmark XT, Ventana, and AutostainerLink 48, Dako), and commercially available antibodies. FISH was used for evaluation of the HER-2/neu [HER2/CEP17 probe] and EGFR [EGFR/CEP7 probe] (Abbott Molecular/Vysis). CISH was also used (INFORM HER-2 Dual ISH DNA Probe Cocktail;EGFR DNP probe, Ventana). NGS was performed using the Illumina MiSeq platform. Specific regions of 47 genes of the genome were amplified using the Illumina TruSeq Amplicon Cancer Hotspot panel. Sanger sequencing included selected regions of BRAF, KRAS, NRAS, c-KIT, EGFR, and PIK3CA genes and was performed by using M13linked PCR primers designed to amplify targeted sequences. TNBC was defined as ER IHC negative(Ab: SP1; =0+ or <10%); PR IHC negative (Ab: 1E2; =0+ or <10%), Her2 IHC negative (Ab:4B5) and Her2 ISH negative (Her2 results and interpretation follow the ASCO/CAP scoring criteria. Wolff, AC. et al. (2013) J Clin Oncol: 31 (31):3997-4013). 90% 70% IHC-TOP2A p<0.0001 n/a: data not available due to low N. * low levels predict response to associated drugs. $p values are calculated from comparing the group with the highest frequency with the lowest frequency. ns: non-significant, i.e., p>0.05 Conclusion: Distinct biomarker features identified in different metastatic sites in TNBC present the rationale to investigate differential treatment strategies. Based on biomarker results, etoposide, immune-modulatory agents may seem promising for brain metastases; anti-androgen therapies and nab-paclitaxel may be promising in treating liver metastases; while fluoropyrimidines, gemcitabine and platinum may be considered for TNBC patients with bone metastases. Figure 2: IHC and ISH marker comparison of TNBC tumors taken from the breast, bone, liver and the brain. Bars represent the frequency of the biomarker measurement observed. Therapeutic agents are listed for corresponding biomarkers that show significantly different frequencies. A star indicates statistical significance when the highest mutation rate is compared to the lowest. Figure 3: Comparison of gene mutations rates in primary TNBC and metastases to the brain, liver and bone. No statistical significance was seen with the exception of ERBB4 and PIK3CA with borderline significant p values. Most prevalent in TNBCliver mets Conclusions • The investigation of biomarkers by IHC, ISH and NGS shows molecular heterogeneity of TNBC tumors metastasized to the brain, liver and bone. • These results suggest agents that can potentially deliver increased benefit for TNBC patients with metastases to different organs, including TOP2A inhibitors and immune checkpoint inhibitors for brain metastases, taxanes and anti-androgen agents for liver metastases and fluoropyrimidine, gemcitabine and platinum agents for bone metastases. • The mutation data show promising results including high mutation rates of ERBB4 in brain mets and PIK3CA in liver mets, however, this portion of the study is from a limited NGS dataset. • Distinct molecular profiles identified in different metastases support the rationale of tailoring treatments of TNBC cancers to the biomarker features of individual patients. 75.0% 43.5% 37.5% IHC-EGFR Agents most likely to benefit TNBC bone mets Most prevalent in TNBC-liver mets 65.9% 50.0% 15.8% ISH-EGFR References 26.7% 22.1% 1. 50.0% 41.7% 41.7% 42.8% Low IHC-MGMT 0.0% 20.0% 40.0% 60.0% 80.0% 100.0% 120.0% 2. 3. Andre, F., C.C. Zielinksi (2012) “Optimal strategies for the treatment of metastatic triple-negative breast cancer with currently approved agents. “, Ann Oncol. Aug;23 Suppl 6:vi46-51. Tseng. L. M., M.F. Hou, et al. (2013) “Distant metastasis in triple-negative breast cancer” Neoplasma. 60(3):290-4. Jameson, G.S., N.J. Robert et al. (2014) “A pilot study utilizing multi-omic molecular profiling to find potential targets and select individualized treatments for patients with previously treated metastatic breast cancer.” Breast Cancer Res Treat. 147(3):579-88.