Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
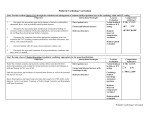
UT Inpatient Cardiology Rotation Brief description and target group: A four-week rotation for Internal Medicine residents caring for patients under the care of a cardiologist in a tertiary medical center. Overall Educational Goals and Objectives: This rotation involves all aspects of caring for hospitalized patients under the care of a cardiologist. The rotation centers around the management of patients admitted or consulted on by an academic “teaching” service. The service is comprised of an attending cardiologist, a general cardiology fellow, 2 internal medicine residents, and a cardiovascular pharmacist. The larger multidisciplinary team includes members from nursing, pharmacy, physical therapy and nutrition. There will be an emphasis on patients that are critically ill, but will include those admitted to a telemetry floor or other areas of the hospital. The responsibilities of the resident on this rotation includes performing histories and physicals on admissions or new consults, daily notes and orders, communication with patients’ families, coordination of consultations, procedures, discharge summaries, identifying the academic team patients with a sticker and face-to-face hand-over to the night medicine service. The fellow will lead the team and provide oversight to patients admitted to the cardiac intensive care unit, be the first point of contact for the family members of patients who are critically ill and coordinate the transfer of patients out of the intensive care setting and into an acute care or telemetry environment, ensuring excellent handover. The fellow will serve as the immediate contact for the residents and will guide daily rounds and management of the patients. It is the responsibility of the team (fellow or resident) to communicate with the attending of record whenever there is a decline in the clinical condition of a patient that necessitates a transfer to the ICU, intubation, or cardiopulmonary resuscitation. In the event of a patient death, this must also be communicated to the attending of record. Rotation Specific Educational Goals by Competency Overall Goals for each resident 1. Medical Knowledge. Exhibit an understanding of the basic and clinical science associated with common conditions that affect the cardiovascular system. Develop and execute a care plan for patients that are seriously or critically ill. 2. Patient Care. Implement a treatment plan in the setting of a multidisciplinary team. Provide patients and families a detailed understanding of the plan and the associated potential risks and benefits. 3. Interpersonal Skills and communication. Provide care for the patient that leaves the patient and family well informed. Communicate effectively with other members of the multidisciplinary team. Participate in bedside and class room didactic teaching. 4. System Based Practice. During the rotation, there will be opportunities to participate in ongoing quality improvement initiatives focused on improving care of the cardiovascular patient. A multidisciplinary team that includes Cardiothoracic Surgeons, Cardiovascular Intensivists and representatives from nursing, pharmacy, respiratory therapy and nutrition are working to improve care delivery, quality and outcomes. The goals of this team are to address issues relating to the delivery of healthcare services to patients with a cardiovascular diagnosis. Issues will include meeting core-measures, and patient safety goals, early ambulation and extubation, ensuring a smooth transfer out of the intensive care environment, optimizing patient education, and creating more efficient systems of care. 5. Problem Based Learning. The team will identify areas for further study on rounds. The fellow will coordinate a mini-journal club around the topics and organize a time to review the evidence. 6. Professionalism. Adhere to the dress and behavioral standards set forth by the University of Tennessee at Chattanooga. All members of the team will be expected to interact with patients honestly and provide an atmosphere that is patient and family centered; to fully participate in quality of care and safety initiatives to insure patient safety; and to participate in the education of the team and to develop a pattern of lifelong learning. Additionally, all members of the team will be expected to accurately report duty hours, identify situations in which fatigue or other issues impair their ability to provide excellent clinical care. Teaching methods: The principal teaching method is practical hands-on experience in a mentored environment for the trainee in all aspects of the care process on the inpatient service, encompassing patients admitted to the service. The Cardiovascular Disease attending has ultimate responsibility for all patients so will constantly supervise and guide the trainee as needed in the evaluation, diagnosis and treatment of patients. Teaching is centered around discussion of the individual patient with emphasis on decisionmaking, evidence-based therapies, ethical and socio-economic issues. More formally, the service has a 13-block lecture schedule and the residents will be invited to attend all lectures. They will be required to attend the Friday afternoon core lectures and case management series that occurs from 1:30-3:30 PM. Mix of diseases, patient characteristics, types of clinical encounters, procedures, and services: The patients seen during this rotation include the typical mix of the acute adult cardiac care with ~60% male and 40% female. The clinical pathology to which the resident will be exposed is wide-ranging and includes acute and chronic ischemic disease manifestations, all types of valvular heart disease, pulmonary hypertension, heart failure in all its etiologies, hypertension, and conduction system disease, and patients with renal and other peripheral arterial disease. Most learning on this rotation will be triggered by a first-hand encounter with a patient with either an acute or non-acute indication for hospitalization. Specific aspects of care include, but are not limited to, the management of ST segment elevation and non-ST segment elevation myocardial infarction, management of heart failure in all its etiologies, secondary prevention of ischemic heart disease, managing acute disturbances of cardiac rhythm, the management of antiarrhythmic drug therapy, management of acid-base and electrolyte disturbances in the cardiac patient, and the management of cardiogenic shock. Experience will also be gained in the postoperative management of patients undergoing cardiac surgery. Service Coverage: DAY MONDAY R1 R2 TUESDAY R1 R2 WEDNESDAY R1 R2 THURSDAY R1 R2 FRIDAY R1 R2 SATURDAY R1 R2 SUNDAY R1 R2 TIME 7:45 AM – 8:15 PM 6 AM – 6 PM 7:45 AM – 8:15 PM 6 AM – 6 PM 7:45 AM – 8:15 PM 6 AM – 6 PM 7:45 AM – 8:15 PM OFF 7:45 AM – 8:15 PM 6 AM – 6 PM 7:45 AM – 8:15 PM 6 AM – 6 PM OFF 7:45 AM – 8:15 PM HOURS 12.5 12 12.5 12 12.5 12 12.5 0 12.5 12 12.5 12 0 12.5 TOTAL 12.5 12 25 24 37.5 36 50 36 62.5 48 75 60 75 72.25 The service coverage will be daily with one resident covering 6 AM – 6 PM and the second resident covering 7:45 AM – 8:15 PM. Each resident will take one day off per week. This must be coordinated with the fellow at the beginning of the rotation. The fellow is off on Saturday so this day cannot be taken off. Transition of care to the night float team must be face-to-face each morning and night. Reading lists and other educational resources to be used: The core of information underlying diagnosis and clinical decision making in inpatient cardiology is to be found either on-line in practice guidelines or in core clinical journals. A significant number of relevant publications can be found referenced in the American College of Cardiology-American Heart Association guidelines. Thus, while the trainee will receive a virtual continuous infusion of references from the inpatient service attending physician, and will be responsible for gaining a grasp of this literature. The general internal medicine review series MKSAP and Medstudy provide a good general overview on cardiovascular disease. Method of evaluation of resident performance: The resident will be continuously evaluated each day as the rotation proceeds, with feedback from attending cardiologists and fellows throughout the rotation. A written evaluation using the competency based, global evaluation form in New Innovations will be prepared for each resident after completion of the rotation by both the attendings and fellows that were on the team during that time. Medical knowledge is assessed daily during rounds and patient admissions. In order to achieve a PASSING GRADE for the rotation, the attending physician must verify that the resident performed at an average or better level in each of the 6 medical competencies. Assessment Tool Faculty end of rotation assessment Fellow end of rotation assessment Staff assessment Procedure supervision Type Global Assessment Competency All PGY Level All Multisource feedback All All Multisource feedback Direct observation All PC All All UT Cardiovascular Disease Inpatient Service Rotation for Residents Upon completion of this rotation, residents will be able to: Objective Core Competency Learning Activity Teaching Method Evaluation Method MEDICAL KNOWLEDGE Understand the pathophysiology, clinical manifestations, natural history, and principles of management of aortic dissection, atrial arrhythmias (fibrillation, flutter, AVNRT), ventricular arrhythmias (tachycardia and fibrillation), AND simple congenital heart lesions. Understand the pathophysiology, clinical manifestations, natural history, prevention and principles of management and of coronary artery disease and myocardial infarction including follow-up care and postoperative care. Understand the pathophysiology, clinical manifestations, natural history, and principles of management of endocarditis. Understand the pathophysiology, clinical manifestations, natural history, and principles of management of hypertension including evaluation for primary and secondary hypertension and hypertensive emergency. Understand the pathophysiology, clinical manifestations, natural history, and principles of management of myocarditis and pericarditis. Understand the pathophysiology, clinical manifestations, natural history, and principles of management of cardiogenic shock. Understand the pathophysiology, clinical manifestations, natural history, and principles of management of valvular heart disease including aortic stenosis and mitral regurgitation. Demonstrates basic understanding of the pathophysiology, clinical manifestations, natural history, prevention, and principles of management of the common iatrogenic complications including adverse drug reactions, cardiac catheterization complications, central venous access complications, deep venous thrombosis, bleeding complications associated with antiplatelet and anticoagulant therapy, hypotension, and acute renal failure. Recognize major findings on routine imaging, including CXR, CT/MRI of chest, left ventricular catheterization, coronary angiography, right ventricular catheterization, echocardiogram, EKG, and ambulatory EKG monitoring. Demonstrates basic knowledge of the predictive power and test characteristics of laboratory and radiological testing. PATIENT CARE MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,C,E MK 1, 2, 3, 6, 7 A,B,C,E MK 1, 2, 3, 6, 7 A,C,E Acquire accurate and relevant history from the patient in an efficiently customized, prioritized, and hypothesis driven fashion. Seeks and obtains appropriate, verified, and prioritized data from secondary sources. Perform an accurate physical examination that is appropriately targeted to the patient's complaints and medical conditions. Identify pertinent abnormalities using common maneuvers. Identify some subtle or unusual physical findings that may influence clinical decision making, using PC 1,2,7 A,C PC PC 1,2,7 1,2,7 A,C A,C PC 1,2,7 A,C advanced maneuvers where applicable. Accurately track important changes in the physical examination over time. Synthesize all available data, including interview physical examination, and preliminary laboratory data, to define each patient’s central clinical problem. Develop prioritized differential diagnoses and evidence based diagnostic / therapeutic plans for common inpatient conditions. Modify differential diagnosis and care plan based upon clinical course and data as appropriate. With supervision, demonstrates competence, technical proficiency, and post procedure management in advanced cardiac life support. Make appropriate clinical decisions based upon the results of common diagnostic testing, including routine blood chemistries, hematologic studies, coagulation tests, arterial blood gases, ECG, chest radiographs, urinalysis and other body fluids. Demonstrate basic management of patients whose diagnosis is unclear. Recognize situations with a need for urgent or emergent medical care including life threatening conditions. Initiate management and obtain urgent assistance for patients with emergent medical conditions. Recognize when to seek additional guidance. Provide appropriate preventive care and teach patient regarding self-care. Effectively manage patients with common clinical disorders seen in the practice of inpatient cardiovascular medicine with appropriate supervision. Customize care in the context of the patient’s preferences, overall health, and wishes. PRACTICE-BASED LEARNING AND IMPROVEMENT PC PC 1,2,7 1,2,7 A,C A,C PC 1,2,7 A,C PC PC 1,2,7 1,2,7 A,C, A,C,D PC 1,2,7 A,C PC PC PC PC PC PC 1,2,7 1,2,7 1,2,7 1,2,7 1,2,7 1,2,7 A,C A,C,D A,C,D A,C,D A,C,D A,C,D PC 1,2,7 A,C,D Communicate risks and benefits of alternatives to patients. Customize clinical evidence for an individual patient. Appreciate the responsibility to assess and improve care collectively for patients on the inpatient service. Identify clinical questions through self study as they emerge in patient care activities. Access medical information resources to answer clinical questions and library resources to support decision making. Respond welcomingly and productively to feedback from all members of the health care team including faculty, peer residents, students, nurses, allied health workers, patients and their advocate. Actively seek feedback from all members of the health care team. Integrate teaching, feedback, and evaluation with supervision of interns’ and students’ delivery of patient care. Identify areas in the inpatient hospital environment that can be changed to improve effect of the processes and outcomes of care. Actively participate in the department’s required teaching conferences. Develop time management skills to perform required tasks in a reasonable amount of time with satisfactory quality. Reflect on feedback in developing plans for improvement. INTERPERSONAL AND COMMUNICATION SKILLS PBLI PBLI PBLI PBLI PBLI 1,2 1,2 1,2 1,2 1,2 A,C A,C,D A,C,D A,C A,C PBLI 1,2 A,C,D PBLI PBLI 1,2 1,2 A,C,D A,C PBLI 1,2 A,C,D PBLI PBLI 1,2,3,4,5,6 1,2 A,C A,C PBLI 1,2 A,C Demonstrate patient-centered interviewing techniques: a compassionate approach to history taking; the ability to modify interview techniques in response to the patient’s demeanor, cultural and/or religious background, and level of competency. Communicate sensitively and effectively with patients and with their families, including sensitivity to differences in race, culture, gender, sexual orientation, socioeconomic ICS 1,2 A,B,C,D status, literacy, and religious beliefs. Write complete, timely, and concise admission notes for all patients admitted. Write complete, timely, and concise progress notes documenting daily care of patients admitted. Request consultative services in an effective manner. Clearly communicate the role of consultant to the patient, in support of the primary care relationship. Explain the general process of any ordered procedure (Cardiac catheterization, Echo, etc) with the emphasis on alleviating the patient’s fears and apprehensions. Assist patients in decision-making regarding treatment options, end-of-life care, and discharge planning. Utilize the electronic medical record to compose a complete, concise discharge summary. Ensure that the patient’s primary care physician and referring physician (when applicable) receives a copy of the discharge summary in a timely manner. Communicate effectively with colleagues when signing out patients or turning over care to another service. Engage in collaborative communication with all members of the health care team. Deliver appropriate, succinct, hypothesis-driven oral presentations. PROFESSIONALISM ICS ICS ICS ICS ICS 1,2 1,2 1,2 1,2 1,2 A,C,D A,C,D A,C,D A,C,D A,C,D ICS ICS 1,2 1,2 A,C,D A,C ICS ICS ICS 1,2 1,2,3,5,6 1,2,3,5,6 A,C,D A,B,D A,B,D Adhere to the UT COM Chattanooga Code of Professional Conduct. Demonstrate honesty and integrity at all times. Behave with high regard and respect for patients, colleagues, consultants, and all members of the health care team. Appreciate the effects of cultural and religious background on the patient’s approach and attitudes toward decision making, their disease, and treatment. Recognize the common ethical issues that face patients, their families, and caregivers related to chronic illnesses. Provide meaningful feedback to colleagues regarding their performance. Demonstrate a commitment to relieve pain and suffering. Respond promptly and appropriately to clinical responsibilities including but not limited to calls and pages. Carry out timely interactions with colleagues, patients and their designated caregivers. Ensure prompt completion of clinical, administrative, and curricular tasks. Recognize the scope of his/her abilities and ask for supervision and assistance appropriately. Maintain patient confidentiality. Recognize that disparities exist in health care among populations and that they may impact care of the patient. Provide physical, psychological, social and spiritual support for dying patients and their families. Recognize, respond to and report impairment in colleagues or substandard care via peer review process. Recognize the need to assist colleagues in the provision of duties. Serve as a professional role model for more junior colleagues . Effectively advocate for individual patient needs. Recognize, respond to and report impairment in colleagues or substandard care via peer review process. Recognize and manage conflict when patient values differ from their own. SYSTEMS-BASED PRACTICE P P P 1,2,3,4,5,6 1,2,3,4,5,6 1,2,3,4,5,6 A,C,D A,C,D A,C,D P 1,2,3,4,5,6 A,C,D P 1,2,3,4,5,6 A,C,D P P P P P P P P 1,2,3,4,5,6 1,2 1,2 1,2,3,4,5,6 1,2,3,4,5,6,7 1,2,3,4,5,6 1,2,3,4,5,6 1,2,3,4,5,6 A,C,D A,C,D A,C,D A,C,D A,C,D A,C,D A,C,D A,C,D P P P P P P P 1,2 1,2,3,4,5,6 1,2,3,4,5,6 1,2,3,4,5,6 1,2 1,2,3,4,5,6 1,2,3,4,5,6 A,C,D A,C,D A,C,D A,C,D A,C,D A,C,D A,C,D Understand the role of multidisciplinary resources to prepare patients and their families for hospital discharge, home management of disease, nursing home placement, and end-of-life care. Consider alternative solutions provided by other teammates. SBP 1,2 A,C,D SBP 1,2 A,C,D Identify, reflect upon, and learn from critical incidents such as near misses and preventable medical errors. Reflect awareness of common socio-economic barriers that impact patient care. Collaborate with other members of the health care team to assure comprehensive patient care. Manage and coordinate care and care transitions for patients discharged from the in-patient service, including home, rehabilitation, inter-hospital transfer, and hospice. Understand mechanisms for analysis and correction of systems errors. Demonstrate the incorporation of cost-awareness principles into standard clinical judgments and decisionmaking.. Use evidence-based, cost-conscious strategies in the care of hospitalized patients with complex illness. Negotiate patient-centered care among multiple care providers. SBP SBP SBP SBP 1,2 1,2 1,2 1,2 A,C,D A,C,D A,C,D A,C,D SBP SBP 1,2,3,6 1,2 A,C A,C,D SBP SBP 1,2 1,2 A,C A,C,D Core Competencies Learning Activities / Teaching Methods Evaluation Methods PC Patient Care MK Medical Knowledge PBLI Practice-Based Learning & Improvement ICS Interpersonal & Communication Skills P Professionalism SBP Systems-Based Practice 1. 2. 3. 4. 5. 6. 7. A. B. C. D. E. Direct Patient Care Teaching Rounds Noon Conference Medical Grand Rounds Journal Club Cardiovascular Conferences Assigned Readings Attending Evaluation Attending Observation of Procedures Fellow Evaluation Multisource Evaluation In-Training Examination