Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
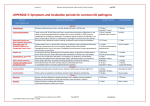
Travellers’ diarrhoea: prevention and management It has long been said that travellers’ diarrhoea could be prevented by a simple ‘boil it, cook it, peel it, or forget it’ regime, but studies have found that people who follow these rules may still become ill. Most people affected experience symptoms within 2–3d of arrival at their foreign destination, with more than 90% of cases starting within the first 2w, turning a dream fortnight into a nightmare! NICE CKS 2013 offers us helpful guidance for prevention, treatment and management of travellers’ diarrhoea, which can affect up to 60% of travellers. Symptoms Acute watery diarrhoea, at least 3 loose to watery stools/24h. Blood may be present in stools. May be accompanied by one or more of these symptoms: abdominal pain and cramps affect 80% of sufferers fever nausea/vomiting. Always enquire about locations visited, and vaccinations undertaken prior to travel, when patients present with post-travel diarrhoea. Enteric fever (typhoid) may present as diarrhoea and high fever, more commonly in children than in adults. Public Health England quarterly statistics show 78 cases reported across England and Wales in July–September 2015 alone. Typhoid is not as rare as you may think! (PHE, 2015). Cholera, which presents as severe watery diarrhoea, is less common, yet 42 confirmed cases were reported to PHE between 2011 and 2013, all of which emanated from foreign travel (PHE 2015). Ebola, high-profile news in 2015, can also present as diarrhoea and low-grade fever before its haemorrhagic phase. Cases have been thankfully few in the UK, but vigilance should be maintained. The management of suspected Ebola is not mentioned in CKS 2013, but I have included a link to PHE advice for primary care in the Practical tools box at the end of this article. Prognosis In most cases, travellers’ diarrhoea is non-serious and self-limiting: Untreated bacterial diarrhoea, for most people, lasts around 3–5d. Viral diarrhoea symptoms last for 2–3d. Protozoal diarrhoea can persist for weeks to months if not treated. However, around 1.5% of people who experience travellers’ diarrhoea then go on to develop irritable bowel syndrome. Infants, elderly people and the immunocompromised can have more severe effects from travellers’ diarrhoea. Emergency admission is warranted if the patient is vomiting and unable to retain fluids, or if there are features of severe dehydration. Causes Cause is ingestion of contaminated food/water and the causative organism partly depends on the country of travel. Bacteria account for 80–90% of cases, most common bacterial causes are: E. coli, Campylobacter, Shigella and Salmonella. Enterotoxigenic E. coli (ETEC), mostly in Latin America and Africa, but is also seen globally. Campylobacter, in people visiting South Asia and South East Asia. Viral causes account for 15–20% of cases of TD: Norovirus and rotavirus are most commonly implicated. Norovirus outbreaks are commonly seen in holiday resorts or on cruise ships. Parasites are responsible in 2–10% of cases: Giardia intestinalis and Cryptosporidium are typically associated with long-term travel or travel to endemic areas such as Eastern Europe, Italy, St Petersburg, Bangladesh and Ethiopia. Protozoans such as Giardia are a common causative organism in those with illness lasting >10d, symptoms starting after return from travel or Illness associated with weight loss (http://emedicine.medscape.com/article/176718-overview#a5). Toxins in uncooked food account for 5% of cases: Usually Staph. aureus, Bacillus cereus or Clostridium perfringens. These tend to cause sudden onset of nausea, vomiting and diarrhoea. Cholera is an uncommon cause of diarrhoea in travellers returning to the UK (NaTHNaC, 2011). Assessing risk before travelling To assess the risk of acquiring travellers’ diarrhoea find out the following. Which country the person is going to visit Low risk zones (<7%): western Europe, USA, Canada, Japan, Australia, and New Zealand. Intermediate risk zones (<20%): southern Europe, Israel, South Africa, Caribbean islands and the Pacific. High risk zones (>20%): Africa, Latin America, the Middle East, and most parts of Asia. Individual countries where strict food, water, and personal hygiene precautions should be practised are listed on www.nathnac.org. Assess for other risk factors Infants, elderly people, those with severe cardiac or renal disease, people who are immunocompromised. Areas with poor sewage facilities, hand washing facilities, or access to safe drinking water. Campers, adventurers, and passengers on cruise ships. Peak incidence is summertime and, in South Asia, the hot months preceding the monsoon season. Consider whether a prescription for ‘ stand by’ antibiotic treatment (to use if affected) is a suitable alternative if prophylaxis is not indicated, if the person is travelling to particularly high-risk locations where medical assistance is poor or unavailable (see section on Prophylactic medication and stand-by antibiotics, below). Prevention The incidence of travellers’ diarrhoea has not significantly fallen in the last decade. Information leaflets on food safety and drinking water are available on the World Health Organization website – see Practical tools box at the end of this article. Hygiene measures Alcohol sanitising hand rub, where’s the evidence? Well, there isn’t masses of hard evidence, but a preliminary study of 257 international travellers returning from abroad concluded that the use of hand sanitiser is associated with a significant reduction (CI 0.04) in the incidence of travellers’ diarrhoea – 17% of those who had used hand rub were affected, compared to 30% in those who had not (Travel Med Infectious Dis 2014;12:494). Hand rub has got to be worth a go! Hands should always be washed before eating, and before handling food — particularly after contact with raw meat and uncooked food. Foodstuffs to avoid CKS suggests avoiding: Tap water and ice cubes. Shellfish, mussels, oysters, and clams (filter feeders) because they can concentrate pathogens and toxins. Food that is not thoroughly cooked, and steaming hot prior to serving. Food from buffets, markets, and street vendors, unless kept piping hot, or well-refrigerated. Homemade mayonnaise and uncooked eggs. Cooked food that has been in contact with raw food, or with uncooked eggs. Leafy greens including lettuce, and uncooked fruit and veg with damaged skin. Unpasteurised dairy products, including ice cream. Drinking water Bottled water is the safer choice for drinking water. The seal must not have been tampered with. Water should be boiled (for at least 1min) if in doubt. Where there is no access to safe water, micropore filtering and chlorine preparations are a second-best option. Advise patients that, during an episode of diarrhoea: Increase fluid intake to prevent dehydration — particularly important in young children and elderly people. For infants, breast-feeding should not be interrupted. Avoid alcohol and other beverages with a diuretic effect such as coffee and tea. Prophylactic medications and stand-by antibiotics Antibiotic prophylaxis, although effective, should not be routinely prescribed because: It offers no protection against non-bacterial causes. For most, the condition is mild and self-limiting. Prophylaxis can give a false sense of security and lead to neglect of food and water precautions. The increasing prevalence of antibiotic resistance is of concern. Antibiotic treatment can lead to harms. C. difficile infection risk is increased in people taking longer courses of antibiotics, such as for prophylaxis. Other adverse effects associated with antibiotics include gastrointestinal symptoms (such as diarrhoea), allergic reactions, vaginal thrush, and sun sensitivity (associated with quinolones). Antibiotic chemoprophylaxis is ONLY for use in special circumstances, e.g. those with a colostomy. If you must prescribe prophylaxis for travellers’ diarrhoea, CKS suggests the following regime: Ciprofloxacin 500mg once daily (off-label use, requiring private prescription) for up to 3w (but in South and South East Asia there is significant resistance to ciprofloxacin). Ciprofloxacin should not be prescribed for children, adolescents, pregnant or breast-feeding women. Azithromycin is not suitable for prophylaxis. Probiotics: evidence of prevention of travellers’ diarrhoea is limited, and their use is not recommended by CKS as prophylaxis. Bismuth subsalicylate 525mg (2 tablets) chewed four times daily: Offers about 60% cover, but adverse effects are common at the most effective doses. Not to be given if on long-term salicylates or warfarin. Interferes with absorption of doxycycline (malaria prophylaxis). Blackens stools and tongue – so is not widely used! Stand-by treatment of travellers’ diarrhoea (to be taken if needed) CKS advise the following: Ciprofloxacin 500 mg twice daily for 3d (licensed indication, requiring private prescription). Advise the person to evaluate their response after 24h of taking the antibiotic and to complete the 3d course if they are still unwell, or stop sooner if they are improved. Ciprofloxacin should not be prescribed for children, adolescents, pregnant or breast-feeding women, or for people in whom quinolones are contraindicated. For adults, and for children >45kg body weight, azithromycin 500mg daily for 3d (off-label use) may be prescribed as stand-by treatment. Treatment Hydration is critical. In mild illness this is all that is required. Be particularly careful to maintain hydration in infants and children, the elderly, and those with chronic disease. There is no good evidence that oral rehydration solution (ORS) is better than anything else. Bismuth subsalicylate reduces nausea and loose stool frequency. Seldom used in UK but available OTC overseas. It must NOT be used in children <16y, due to link between salicylates and Reye's syndrome. Loperamide may be more effective than bismuth in more severe diarrhoea, and helps with cramps. Onset of action is quicker than bismuth, with benefit seen at 4h. It must NOT be used in children (fears over intestinal obstruction), nor if fever >38.5°C, or if gross blood in stools. Antibiotics can shorten duration of illness by 1–2d compared with placebo, but may cause side-effects. If in the UK, confirm infection so that targeted treatment is possible. If overseas, a single dose or 3 days of treatment will give benefit within 20–36 h. The suggestion is to take stat dose and review 12–24h later – if improvement seen then stop treatment, if not continue for 3d. Ciprofloxacin 750mg stat orally, or 500mg bd for 3d, is the commonest treatment used, but is less effective in South and South East Asia. Azithromycin 1000mg stat orally, or 500mg bd for 3d can be used in place of ciprofloxacin. Beware of nausea with 1000mg dose). Loperamide is safe to take in conjunction with antibiotics. Patients should be advised to seek medical assistance if: Stools are blood-stained, or if there is persistent fever. It is difficult to maintain adequate hydration, because of frequent, watery stools, or repeated vomiting. Diarrhoea persists for more than 3–4d. Children show signs of irritability, sunken eyes, reduced skin elasticity. Remember that salads may have been washed, and ice cubes made up, with water from contaminated water supplies. Brush teeth using bottled water. ‘Boil it, peel it, cook it or forget it’, still goes a long way in preventing travellers’ diarrhoea! Travellers’ diarrhoea Common, and usually resolves spontaneously within 3–4d, but 10% have symptoms for more than a week and 2% have symptoms for more than 1m. In prolonged illness (>10d) or onset after return from travel or if associated with weight loss think of parasitic infections such as Giardia. Boil water or treat it with chlorine/iodine AND filtered with a filter diameter of ≤1µm. Protozoan parasites are relatively resistant to chlorine and iodine. Wash your hands before eating. Avoid 'high risk' foods: 'Wash it, peel it, boil it, cook it or forget it!'. Antibiotics, probiotics and bismuth subsalicylate can be used as prophylaxis, but antibiotics are only recommended in specific circumstances. Treatment is with hydration +/– antidiarrhoeal agents +/– antibiotics. Professional development Do you, and others in your practice, Read-code Travellers’ diarrhoea? Try doing a search. Could it be helpful, to individual patients and in infection control, to Read-code Travellers’ diarrhoea more accurately? Do you have patients who travel to visit relatives in Ebola-endemic areas – brush up on advice for primary care from Public Health England: www.gov.uk/government/uploads/system/uploads/attachment_data/file/404002/Informati on_for_primary_care_managing_patients_who_require_assessment_for_Ebola.pdf Practical tools WHO Food and Drink safety leaflet: www.who.int/foodsafety/publications/consumer/en/travellers_en.pdf Ensuring safe drinking water, WHO advice leaflet: www.who.int/water_sanitation_health/hygiene/envsan/sdwtravel.pdf WHO travel advice: www.who.int/ith/en/index.html The Foreign and Commonwealth Office offers advice on travel including health advice plus other issues (visas, security risks, local laws and customs, risks of natural disasters, how to register on arrival, what to do if things go wrong): www.fco.gov.uk/en/travellingand-living-overseas/travel-advice-by-country/ The one-day course for all nurses in general practice Swamped with new clinical information and latest guidance? ‘Matt/The Daily Telegraph 2016 © Telegraph Media Group Ltd’ Too much for you to read and too little time to read it? Need to give evidence-based advice to patients, carers and colleagues? Want help meeting NMC revalidation requirements? We trawl through all the relevant journals to bring you right up to speed on the issues, literature, research and guidelines relevant to nursing in general practice. We are the only update course for Nurses that is completely free from pharmaceutical company sponsorship so you’ll get an independent, unbiased view of all of the latest evidence. What will be covered? This is a dynamic and engaging one-day course that offers a wide-ranging, evidence-based programme, including all you need to know about: • NMC Revalidation • Long-term conditions important to primary care nurses, inc. diabetes, atrial fibrillation and liver disease • Respiratory conditions: preventing asthmas deaths, management of acute exacerbation • Lipids and statins • Gastroenterology • Sexual health, inc. FGM & the Law • Suspected cancer and latest guidelines • Vaccinations • plus top-to-toe topics from rhinitis to vaginal discharge to verrucas! Who is this course for? All General Practice Nurses. 98% of the nurses who attended our Spring GPN Update course would recommend it to a colleague. Practice Nurses and Nurse Practitioners said: “Probably the best course I have been on for a long time” “Highly informative and warranted time out of practice” “The Handbook will become my bible!” We know how important it is that nurses and doctors share knowledge and skills to improve care. Our course is both written and presented by our resident ANP Debra Sprague and GP Sharon Dixon. What’s not included: This course contains no theorists, gurus or sponsors. It is brought to you by real-life nurses and doctors, who will be back at the coal face once the course has finished! www.gp-update.co.uk/nurses What will you get on our course? Updates on the latest clinical evidence and guidance across a wide range of chronic and acute conditions. •Great practical tips and tools to improve patients’ engagement with their long-term conditions. •Loads of ideas, guidance and reassurance on making CPD a part of your everyday practice. •Tools tailored to meet NMC requirements, to help you with your Revalidation evidence. •Ways to move things forward in your practice area. •Tips to help you and your team work together effectively •Expertise and practical tools to share with your practice and support patients in managing their health. •Guidance in managing clinical risk, with suggested activities to help you easily audit aspects of clinical safety •Lots of humour and fun to help get through everything in one day – without compromising the content of course! The GPN Update Handbook Delegates receive a copy of the 340-page GPN Update Handbook. This fully-referenced, evidence-based handbook covers the most important research, policy and guidance relevant to primary care nursing over the last 5 years. GPN CPD You’ll also get one year’s FREE subscription to GPN-CPD.com - a purpose built tool giving you a really easy way to track your CPD for NMC Revalidation and the entire course handbook online. No need to pay extra for these valuable resources! Who are we? Red Whale is one of the leading providers of primary care medical and nursing education in the UK with over 13,000 primary care practitioners attending our courses each year. We specialise in producing courses that are evidence-based, highly relevant to everyday practice and full of actions that delegates can take away and implement immediately. You may well have already heard great things about the GP Update Course from your GP colleagues. The GPN Update Course keeps that fast-moving and fun format, with material focused on the priorities for nursing in primary care: to support YOU in supporting your patients. For more details, go to www.gp-update.co.uk/nurses The GPN Update Course dates Exeter Leeds Birmingham Fri 14 Oct Fri 4 Nov Sat 5 Nov Price: £195 DISCOUNT CODE: Enter GPN2016A45 code at checkout or when booking on the phone and receive £45 discount on any GPN Update autumn course dates To book: Online at www.gp-update.co.uk or use the form below or call us on 0118 960 7077 I would like to come on the following GPN Update Course (please write legibly!): Course location............................................................................................ Course date...................................... Name............................................................................... Address.......................................................................... .................................................................................................................................................................................... Email.................................................................................................... Discount Code........................................... (Please write your email address clearly as we’ll use it to send your confirmation letter and receipt.) I can’t attend a course, but I would like to order the 2016 GPN Handbook and 12 months access to GPN CPD. £150 Please send this form with your cheque payable to GP Update Limited to: GP Update, The Science and Technology Centre, Earley Gate, Whiteknights Road, Reading RG6 6BZ GP Update Limited, registered in England and Wales No. 7135974. Registered Office: Prospect House, 58 Queens Road, Reading RG1 4RP Full terms and conditions are available at www.gp-update.co.uk GPN/0916 Relevant challenging and fun!