Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
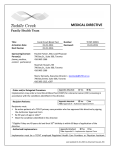
Medical Questionnaire Questionnaires will be kept confidential. Patient’s full name: Preferred name: Do you currently have a family physician? _____ If yes, name & location: For women: For men: _____ Number of pregnancies Delivery Mode:_______________ _____ Number of children_____ Prostate disorders: Testicular disorders: Age at start of menstruation _______ Age at start of menopause: ______ HRT ______________ # yrs: ________ Have you ever breastfed? Y/ N _____ Number of children Uterine Disorders: Hysterectomy: Full or Partial Preventative Health Screening (age 50+ or family Date of Last Pap Smear: History of Abnormal Pap Smear: Y /N history) Preventative Health Screening (age 50+ or family history) Date of last Mammogram: Due for Mammo: Date of last FOBT/colonoscopy: Y/N Mammo Req Given: Y / N Due for FOBT: Y / N FOT given: Y / N Declined FOBT: Y / N Colorectal Cancer: Date of last FOBT/colonoscopy: Due for FOBT: Y / N FOBT given: Y / N Declined FOBT: Allergies Allergies to medications: (specify type of reaction) Other known allergies, include reactions: Surgical History List surgeries and dates (include tonsils, adenoids, appendix, etc): Have you had a reaction to anaesthesia? Have you been told you are difficult to intubate? 1 I003 – SGBCHC – 1 HOUR INTAKE PT QUESTIONNAIRE - DRAFT Medical problem: Head, eye, ear, nose, throat Angina/Angioplasty/Cardiac/CAD Hypertension High cholesterol Stroke/TIA Vascular disorders Clotting/bleeding disorder Person al medical history Anemia Asthma/emphysema/COPD/other lung disorder Gastrointestinal disorders Liver disease – Hep A/B/C, cirrhosis Kidney/bladder disorders Arthritis Osteoporosis/osteopenia Chronic muscle/joint pain Thyroid disease Diabetes Headaches/migraines Neurological disorders Psychiatric/mental health Addictions Dementia/ABI/cognition issues Skin – eczema, psoriasis, other Cancer type: Diagnosis date: Treatment: Problem/Date of onset: Immunization Flu Shot: Y / N (record for MSAA indicators) Pneumococcal (age 65+): Y / N Zostavax (age 55+): Y / N Last Td/Tdp: (one pertussis vaccine in adulthood regardless of last Td) Family History List ALL family members & any illnesses. If deceased, indicate at what age & COD. Mother:________________________________ Father: ________________________________ Sister(s): _______________________________ Brothers: _______________________________ ______________________________________ ______________________________________ Employment Occupation/History: Where are you employed? If not working: □ Retired □ EI □ OW □ other: Disability pension: CPP / ODSP / other: Are you interested in volunteering with the SGBCHC? □ No income □ Yes □ No Relationship/Marital status: Abuse: Other SDM, POA-PC, POA-F: Who do you live with? Who is your support system? Do you have in-home support? (CCAC, Red Cross, hospice, etc.) Literacy: Mental health issues: 3 I003 – SGBCHC – 1 HOUR INTAKE PT QUESTIONNAIRE - DRAFT Tobacco use: Non-Smoker Never Quit Date: Years smoking: cigs/day: Quit attempts (dates): On a scale of 1-10 how would you rate your motivation to quit smoking? Not ready to quit Ready to quit Interest in quitting: If yes, referred to smoking cessation group: □ Do you drink alcohol? __________ If yes, how many drinks per week? ________________________ Lifestyle Type(s) of alcohol consumed: Recreational drugs: Gambling: Transportation: Do you exercise regularly? __________ Frequency: _______________________ Describe type(s) of activity: Nutrition: Mobility issues: □ mobility aid used (e.g.: cane, walker, wheelchair): Falls risk: Have you had a fall in the past 12 months? Have you had a near fall in the past 3 months? Do you have a fear of falling? *Yes to any, refer to falls prevention program* Pharmacy: Extended health benefit plan/ODSP/Trillium/Other: Do you see any specialists? (Name and specialty): Are you taking any medication(s) at this time? Is it ok to leave information on your answering machine or with a spouse/person who answers the phone? □ Yes □ No □ Sometimes Details: Are there any other health issues/concerns you would like to mention at this time: 5 I003 – SGBCHC – 1 HOUR INTAKE PT QUESTIONNAIRE - DRAFT Referral to programs: Date: Chronic Disease/Pain Self Management Program Nutrition Programs Diabetes Education Workshops Mindfulness Meditation Nordic Pole Walking Fitness for Health Signature: _________________________________ Date: __________________________