Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
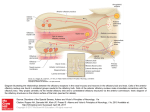
To rediscover the olfactory cleft Poster No.: C-1701 Congress: ECR 2010 Type: Educational Exhibit Topic: Head and Neck Authors: P. Henrot , P. Gallet , B. Grignon , T. Georgel , R. Jankowski ; 1 2 1 2 2 2 2 Vandoeuvre-lès-Nancy/FR, Nancy/FR Keywords: olfactory cleft, woodworker's adenocarcinoma, sinus anatomy DOI: 10.1594/ecr2010/C-1701 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 65 Learning objectives To be familiar with the anatomy and radioanatomy of the olfactory cleft To review the radiologic specific signs of tumors of the olfactory cleft To be familiar with the main types of tumors arising in the olfactory cleft Images for this section: Page 2 of 65 Page 3 of 65 Fig. 1: The nasal airstream passes for preference along the floor of the nose and the inferior meatus during quiet respiration. Two physiologically different zones are encountered in the nasal cavity: -a wide zone conducting the high speed airflow : the respiratory cleft (yellow area) -a narrow zone conducting a low speed airflow toward the olfactory region : the olfactory cleft (red area) The inferior limit of the olfactory cleft is above the inferior end of the middle turbinate Fig. 2: Coronal CT scan depicts an enlargement of the left olfactory cleft (red line), a bulging of the septum (green line)beyond the midline (blue line), and a lateral tilting of the conchal lamina (yellow line). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 4 of 65 Fig. 3: Axial T2-weighted image demonstrate a different signal between the tumor (asterisk)in low signal and the ethmoidal labyrinth opacified by obstruction (yellow arrow). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 5 of 65 Fig. 4: Man of 85y., reporting nasal obstruction for many years. CT shows evidence of an obstruction of both olfactory clefts (red asterisks). The ethmoidal labyrinth appears with a normal air content ( yellow arrows). Biopsy revealed a bilateral respiratory epithelial adenomatoid hamartoma (REAH). Page 6 of 65 Fig. 5: Man of 72y. suffering from an unilateral left nasal obstruction for 2 years. Biopsy of a left nasal mass demonstrates an inverted papilloma. The mass fills the posterior half of the left olfactory cleft (red arrow) and involves the respiratory cleft inferiorly (yellow arrow). Page 7 of 65 Background Tumors of the olfactory cleft in the literature There is no reported dedicated work dealing with imaging findings of tumors of the olfactory cleft in the radiological literature. In the literature dealing with imaging of tumors of the sinonasal cavities and nasal cavity, the actual anatomic site of origin reported may not always be accurate of well documented. Although some references reported locations of tumors on the lateral wall of the nasal cavity or septum, olfactory cleft is not specifically mentioned. However …some tumors are known to arise in the olfactory cleft (such as olfactory neuroblastoma), some tumors have been reported to involve the upper nasal cavity (such as melanoma), and some tumors frequently involve the lateral wall of the nasal cavity (such as inverted papilloma). Moreover, new concepts were recently reported: • • Woodworkers adenocarcinoma arises in the olfactory cleft (Jankowski et al Rhinology 2007; 45: 308-14). Respiratory Epithelial Adenomatoid Hamartoma (REAH) may be found in the OC in patients suffering from nasal polyposis. Definition of the olfactory cleft is controversial. For some authors, the olfactory cleft corresponds to the olfactory region, covered by the olfactory mucosa, featuring the cribriform plate and 1 cm² on each side, on the lateral nasal wall and on the septal wall. For most authors the olfactory cleft is defined according to a physiological approach taking account the nasal airstream. Also, the air passes for preference along the floor of the nose and the inferior meatus during quiet respiration. Two physiologically different zones in the nasal cavity can thus be distinguished (fig.1): on page 10 • A wide zone conducting the high speed airflow : the respiratory cleft Page 8 of 65 • A narrow zone conducting a low speed airflow toward the olfactory region : the olfactory cleft In this concept, the inferior limit of the olfactory cleft corresponds to the inferior end of the middle turbinate. Radioanatomy of the olfactory cleft (1) The roof is subdivided into three parts (fig.2): on page 12 -The anterior (nasal) part corresponds to the inferior edge of the nasal spine of the frontal bone and nasal bone -The middle (ethmoidal) part corresponds to the cribriform plate -The postérior (sphenoidal) part corresponds to the ethmoidal process of the sphenoid In the coronal plane, the roof of the olfactory cleft is located lower than the ethmoidal roof (fig.3). on page 12 The anterior wall is a virtual frontier between nasal vestibule and the olfactory cleft (fig.4). on page 14 The posterior wall corresponds to the anterior wall of the sphenoid(fig.4). on page 14 The lateral wall, called turbinal wall of the ethmoidal labyrinth, is subdivided into two parts: • • the superior part corresponds to the conchal lamina, a bony lamella that gives insertion to the middle (fig.5) on page 14 , superior (fig.6) on page 16 and supreme turbinates (fig.7) on page 18 . The conchal lamina joins the ethmoidal roof above the cribriform plate and its segment above the cribriform plate is called lateral lamella of the intracranial olfactory groove (fig.8) on page 20 . the inferior part corresponds to the middle turbinate (fig.9) on page 22 The internal wall of the olfactory cleft features the nasal septum (fig.10) on page 24 . The inferior wall is virtual, below the inferior end of the middle turbinate (fig.10) on page 24 . Surrounding anatomic structures are: (fig.11) on page 26 Page 9 of 65 -above: the intracranial olfactory groove and anterior cranial fossa -laterally the ethmoid labyrinth and then the orbit -medially the perpendicular plate covered by septal perichondrium-periosteum and the contralateral nasal cavity Images for this section: Page 10 of 65 Page 11 of 65 Fig. 1: The nasal airstream passes for preference along the floor of the nose and the inferior meatus during quiet respiration. Two physiologically different zones are encountered in the nasal cavity: -a wide zone conducting the high speed airflow : the respiratory cleft (yellow area) -a narrow zone conducting a low speed airflow toward the olfactory region : the olfactory cleft (red area) The inferior limit of the olfactory cleft is above the inferior end of the middle turbinate Fig. 2: The roof of the olfactory cleft is divided in three parts: Anterior (nasal) part (red arrows): nasal bone (1), nasal spine of the frontal bone (2) and internal wall of the frontal sinus (3) Middle (ethmoidal) part : cribriform plate (blue arrows) Postérior (sphenoid) part : ethmoidal process of the sphenoid (green arrow) Page 12 of 65 Fig. 3: In the coronal plane, the roof of the olfactory cleft (blue arrow) is located lower than the ethmoidal roof (yellow arrow) Page 13 of 65 Fig. 4: The anterior wall is a virtual frontier between nasal vestibule and the olfactory cleft (red line). The posterior wall corresponds to the anterior wall of the sphenoid (yellow line). Page 14 of 65 Page 15 of 65 Fig. 5: Coronal CT scan of the lateral wall, called turbinal wall of the ethmoidal labyrinth. The superior part corresponds to the conchal lamina (in red), a bony lamella that gives insertion to the middle (green arrow), superior and supreme turbinates. Page 16 of 65 Page 17 of 65 Fig. 6: Coronal CT scan of the lateral wall, called turbinal wall of the ethmoidal labyrinth. The superior part corresponds to the conchal lamina (in red), a bony lamella that gives insertion to the middle, superior (yellow arrow)and supreme turbinates. Page 18 of 65 Page 19 of 65 Fig. 7: Coronal CT scan of the lateral wall, called turbinal wall of the ethmoidal labyrinth. The superior part corresponds to the conchal lamina (in red), a bony lamella that gives insertion to the middle, superior and supreme turbinates (blue arrow). Page 20 of 65 Page 21 of 65 Fig. 8: Coronal CT scan of the lateral wall, called turbinal wall of the ethmoidal labyrinth. The conchal lamina joins the ethmoidal roof above the cribriform plate. The segment above the cribriform plate is called lateral lamella of the intracranial olfactory groove (yellow arrow). Page 22 of 65 Page 23 of 65 Fig. 9: Coronal CT scan of the lateral wall, called turbinal wall of the ethmoidal labyrinth. The inferior part of the turbinal wall corresponds to the middle turbinate (yellow arrows). Page 24 of 65 Page 25 of 65 Fig. 10: The internal wall of the olfactory cleft features the nasal septum (yellow thisk line). Fig. 11: Anatomic structures surrounding the olfactory cleft are: -above: the intracranial olfactory groove (red arrowhead) and anterior cranial fossa -laterally the ethmoid labyrinth (blue arrow) and then the orbit -medially the perpendicular plate covered by septal perichondrium-periosteum (green arrowhead) and the contralateral nasal cavity Page 26 of 65 Imaging findings OR Procedure details The reported imaging findings in the literature are relative to tumors of the sinonasal cavities or nasal cavities without any specific mention to the olfactory cleft: -Mass (CT-MR) -Variable signal in T1 and T2-weighted images (MR), often low signal on T2 -Intratumoral calcifications or entrapped bone (CT) -Bone erosion of sinonasal walls, orbit and cribriform plate, rarely sclerotic reaction (CT) -Opacification of sinuses by obstruction (more reliably depicted with MR than CT) -Inflammatory dural changes, neoplastic dural invasion or anterior cranial fossa invasion (MR) -Subperiosteal extraconal invasion or intraorbital invasion (CT-MR) -Perineural spread along trigeminal nerve branches (MR) A new concept has been recently reported: wood-workers adenocarcinoma (WAC) arises inside the olfactory cleft and not in the ethmoid. Woodworker's adenocarcinoma was classically described as arising in the ethmoid (2,3) From endoscopic surgical observations, Jankowski et al. reported that WAC arise in the olfactory cleft and grow out in the nasal cavity like polyp neoplasm and, even after reaching big volume, many of them do not invade, but just displace and push out the surrounding structures, ie the nasal septum and the turbinate wall of the ethmoidal labyrinth. (4) These findings of endoscopic surgery were confirmed by radiologic findings in a study from Georgel et al (5). Page 27 of 65 In this study, CT of 20 consecutive woodworker patients treated for an adenocarcinoma with endoscopic surgery were compared with CT of 33 control patients. The olfactory cleft was significantly wider in woodworker's adenocarcinoma than in control patients (15.12 +/-4.52 mm vs 3.28 +/-0.68, p < 0.001) The septum was significantly deviated from midline in woodworker's adenocarcinoma (-4.58 +/-3.05 mm vs 0.51 +/- 0.98 p < 0.001). The conchal lamina angle with vertical midline was significantly higher in woodworker's adenocarcinoma (39.76°+/-13.83 vs 0.45°+/-2.13, p < 0.001). The lateral tilting of the turbinal wall of the ethmoidal labyrinth demonstrates that the site of origin of the adenocarcinoma is inside the olfactory cleft and not inside the ethmoidal labyrinth. (case 1 : fig.1-5 , case 2 : fig.6-9 , case 3 : fig.10-16) MR could also demonstrate the site of origin of the adenocarcinoma inside the olfactory cleft by showing evidence of: -A mass of the olfactory cleft -A lateral tilting of the conchal lamina -A septal bulging -An absence or only partial tumoral involvement of the ethmoid labyrinth containing: •Air (low signal on T1-T2) •Mucosal inflammatory thickenning •Opacification of sinuses by obstruction (high signal T2, no enhancement after gadolinium) •Preservation of the ethmoidal cells under the ethmoidal roof even in large tumors Other tumors could usually or unusually arise in the olfactory cleft Respiratory epithelial adenomatoid hamartoma (REAH) Page 28 of 65 This lesion was described in 1995 by Wenig and Heffner, and previously reported as rare (6). However it may be more frequent and, despite initial descriptions localized HERA on the nasal septum, it appears to more frequently develop in the olfactory cleft (7). It could be commonly associated with nasal polyposis (NP) (8). In a work in progress by Jankowski in 380 operated patients with nasal polyposis, REAH or REAH-like lesions were present at pathologic examination in 18.2 %, bilateral in 62.3%. REAH was retrospectively depicted at CT as a polyp, sometimes associated with an enlargement of the olfactory cleft ( case 4 : fig.17-18 , case 5 : 19-20). Surgery of nasal polyposis may not resolve nasal obstruction or anosmia if lesions of REAH are present inside the olfactory cleft. Depiction of respiratory epithelial adenomatoid hamartoma (REAH) with CT could also optimize surgical planning. Olfactory neuroblastoma Olfactory neuroblastoma is rare featuring 2-5 % of the tumors of the nasal cavity. Mostly arises from the olfactive epithelium in the upper nasal fossa. Intracranial invasion is frequent Dulgerov's classification in1992 (UCLA) takes into account the distance between the tumor and the cribriform plate in the early stages (9) : • • • • T1 : tumor of nasal cavity with persistent airspace between tumor and the cribriform plate T2 : tumor in contact with the cribriform plate or sphenoid involvement T3 : intracranial extradural invasion or orbital invasion T4 : intracranial intradural invasion Imaging findings in olfactory neuroblastoma are (case 6 : fig 21-24) : -A mass -Punctuate intratumoral calcifications (CT) -A low signal T1 relative to brain, and a high signal T2 Page 29 of 65 -A strong enhancement after gadolinium (MR) -Bone erosion of the cribriform plate (CT) -An intracranial extension with cystic areas (MR) Whole body CT and bone scan are mandatory for N and M staging because of the high metastatic risk Inverted papilloma (10,11) Inverted papilloma is rare, featuring 0.4 to 4.7 % of the tumors of nasal cavity. This tumor is benign but locally aggressive. The common site of origin is the lateral nasal wall (95%). Coexisting squamous cell carcinoma is frequent, in about 10 %. Imaging findings of inverted papilloma may simulate malignancy, demonstrating (case 7 : fig.25-27, case 8 : fig.28-31) : -A mass polypoid and lobulated with a columnar pattern -Calcifications in 4 % corresponding to entrapped bone rather than tumoral calcifications (CT) -A low signal on T2-weighted images (MR) -Erosion, thinning or bowing of bone structures corresponding to pressure atrophy and remodeling rather than frank invasion (CT) -A mild enhancement after gadolinium Other tumors that could arise in the sinonasal cavities For the other various sinonasal tumors, the tumoral site in the olfactory cleft has not been specifically mentioned, even if tumors have been sometimes located on the lateral nasal wall or upper nasal cavity: -SCC Page 30 of 65 -Sinonasal undifferentiated carcinoma -Adenoid cystic carcinoma -Melanoma -Lymphoma -Plasmocytoma -Neuroendocrine carcinoma -Metastasis -Paraganglioma -Schwannoma -Ectopic meningioma -Osteosarcoma -Chondrosarcoma -Fibrosarcoma Page 31 of 65 Images for this section: Page 32 of 65 Fig. 1: 76 y. old man, carpenter during 50y. Nasal obstruction and epistaxis. Diagnosis of a well differentiated adenocarcinoma of intestinal type. Obstruction of the left ethmoidonasal cavities (arrow). Fig. 2: 76 y. old man, carpenter during 50y. Nasal obstruction and epistaxis. Diagnosis of a well differentiated adenocarcinoma of intestinal type. Obstruction of the left ethmoidonasal cavities. Page 33 of 65 Fig. 3: Coronal CT scan depicts an enlargement of the left olfactory cleft (red arrow), a bulging of the septum (short green line)beyond the midline (blue line), and a lateral tilting of the conchal lamina (yellow line). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 34 of 65 Fig. 4: Coronal T2-weighted image demonstrate a different signal between the tumor (asterisk)in low signal and the ethmoidal labyrinth opacified by obstruction (yellow arrow). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 35 of 65 Fig. 5: Axial T2-weighted image demonstrate a different signal between the tumor (asterisk)in low signal and the ethmoidal labyrinth opacified by obstruction (yellow arrow). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 36 of 65 Fig. 6: 50 y. old man, carpenter during 17y. Nasal obstruction revealing a pappilar and mucinous adenocarcinoma of intestinal type. Obstruction of the left ethmoidonasal cavities. Page 37 of 65 Fig. 7: 50 y. old man, carpenter during 17y. Nasal obstruction revealing a pappilar and mucinous adenocarcinoma of intestinal type. Obstruction of the left ethmoidonasal cavities (yellow arrow). Page 38 of 65 Fig. 8: Coronal CT scan depicts an enlargement of the left olfactory cleft (red line), a bulging of the septum (green line)beyond the midline (blue line), and a lateral tilting of the conchal lamina (yellow line). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 39 of 65 Fig. 9: Coronal T2-weighted image demonstrate a different signal between the tumor (asterisk)in low signal and the ethmoidal labyrinth opacified by obstruction (yellow arrow). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 40 of 65 Fig. 10: Man, 72 y, retired carpenter reporting epistaxis for many weeks. ENT examination shows evidence of haemorragic polyps at the upper part of the left nasal cavity. Biopsy revealed adenocarcinoma of intestinal-type. CT depicts a mass filling the left olfactory cleft (asterisk). Page 41 of 65 Fig. 11: Man, 72 y, retired carpenter reporting epistaxis for many weeks. ENT examination shows evidence of haemorragic polyps at the upper part of the left nasal cavity. Biopsy revealed adenocarcinoma of intestinal-type. CT depicts a mass filling the left olfactory cleft (asterisk). Page 42 of 65 Fig. 12: Coronal CT scan. Elargement of the left olfactory cleft (red line) associated with a lateral tilting of the conchal lamina (yellow line). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 43 of 65 Fig. 13: CT shows a normal air content of the ethmoid labyrinth (yellow arrow). Page 44 of 65 Fig. 14: Coronal T2-weighted MR shows a normal air content of the ethmoid labyrinth (arrow). The origin of the tumor is inside the olfactory cleft and not in the ethmoid. Page 45 of 65 Fig. 15: MR show a normal air content of the ethmoid labyrinth with a low signal on T2weighted image after gadolinium (arrow) Page 46 of 65 Fig. 16: MR show a normal air content of the ethmoid labyrinth with a low signal on T1weighted images after gadolinium (arrow) Page 47 of 65 Fig. 17: Man of 85y., reporting nasal obstruction for many years. CT shows evidence of an obstruction of both olfactory clefts (red asterisks). The ethmoidal labyrinth appears with a normal air content ( yellow arrows). Biopsy revealed a bilateral respiratory epithelial adenomatoid hamartoma (REAH). Page 48 of 65 Fig. 18: Man of 85y., reporting nasal obstruction for many years. CT shows evidence of an obstruction of both olfactory clefts (red arrows). The ethmoidal labyrinth appears with a normal air content ( yellow arrows). Biopsy revealed a bilateral respiratory epithelial adenomatoid hamartoma (REAH). Page 49 of 65 Fig. 19: Woman of 70y. suffering from recurent sinusitis. CT performed before surgery depicted a polyp inside the left olfactory cleft (arrow). Biopsy revealed a respiratory epithelial adenomatoid hamartoma (REAH). Page 50 of 65 Fig. 20: Woman of 70y. suffering from recurent sinusitis. CT performed before surgery depicted a polyp inside the left olfactory cleft (arrow). Biopsy revealed a respiratory epithelial adenomatoid hamartoma (REAH). Page 51 of 65 Fig. 21: Woman of 69y. reporting unilateral left nasal obstruction for many years and an anosmia for one month. ENT examination shows a bleeding mass. Biopsy demonstrates an olfactory neuroblastoma. CT shows a mass of both nasal cavities (asterisk) with a strong enhancement after contrast medium injection, responsible for lytic changes of the septum (arrow) and turbinates. Page 52 of 65 Fig. 22: Woman of 69y. reporting unilateral left nasal obstruction for many years and an anosmia for one month. ENT examination shows a bleeding mass. Biopsy demonstrates an olfactory neuroblastoma. CT shows a mass of both nasal cavities with a strong enhancement after contrast medium injection, responsible for lytic changes of the septum and turbinates. Page 53 of 65 Fig. 23: T2-weighted MR shows the central location of the mass inside both olfactory clefts (asterisks). The ethmoid labyrinth appears compressed with a high signal on T2 correponding to opacification by obstruction (arrows). Page 54 of 65 Fig. 24: T1-weighted MR with gadolinium shows the central location of the enhancing mass inside both olfactory clefts (asterisks). The ethmoid labyrinth appears compressed with a partial or absence of enhancement after gadolinium (arrows). Page 55 of 65 Fig. 25: Man of 72y. suffering from an unilateral left nasal obstruction for 2 years. Biopsy of a left nasal mass demonstrates an inverted papilloma. The mass fills the posterior half of the left olfactory cleft (red arrow). Page 56 of 65 Fig. 26: Man of 72y. suffering from an unilateral left nasal obstruction for 2 years. Biopsy of a left nasal mass demonstrates an inverted papilloma. The mass fills the posterior half of the left olfactory cleft (red arrow) and involves the respiratory cleft inferiorly (yellow arrow). Page 57 of 65 Fig. 27: Man of 72y. suffering from an unilateral left nasal obstruction for 2 years. Biopsy of a left nasal mass demonstrates an inverted papilloma. The mass fills the posterior half of the left olfactory cleft (red arrow) and involves the whole nasal cavity posteriorly (yellow arrow). Page 58 of 65 Fig. 28: Man of 71y., reporting a bilateral nasal obstruction for 2 years. ENT examination shows a mass filling the both nasal cavities. Biopsy demonstrates an inverted papilloma with some areas of dysplasia. Axial CT scan shows an enlargement of both olfactory clefts (red arrows), and lytic changes of the septum and turbinates (yellow arrows). Page 59 of 65 Fig. 29: Man of 71y., reporting a bilateral nasal obstruction for 2 years. ENT examination shows a mass filling the both nasal cavities. Biopsy demonstrates an inverted papilloma with some areas of dysplasia. Coronal CT scan shows an enlargement of both olfactory clefts (red arrows). Page 60 of 65 Fig. 30: Axial T2-weighted MR demonstrates the central nasal location of the mass involving the nasal vestibule (yellow arrowhead) with a low signal on T2 and a columnar aspect (asterisk) and reponsible for lytic changes of the nasal septum (yellow arrow). Page 61 of 65 Fig. 31: Axial T1-weighted MR demonstrates the central nasal location of the mass (asterisk) involving the nasal vestibule (yellow arrowhead) with a mild enhancement after gadolinium. Page 62 of 65 Conclusion There has been little concern about the olfactory cleft in the radiologic literature. Recent observations shed light on radiologic signs (CT and MR) of tumors of the olfactory cleft at early stage : -Mass occupying the airspace -Enlargement of the olfactory cleft -Lateral tilting of the conchal lamina -Septal bulging -Squeezing of the ipsilateral ethmoidal labyrinth, containing air, inflammatory changes or opacification by obstruction Clinical applications could be suggested: •Knowledge of tumors arising in the OC may improve the depiction of small adenocarcinomas in woodworkers with a symptom, or Respiratory Epithelial Adenomatoid Hamartoma in patient suffering from anosmia. •Imaging contributes to new therapeutic approaches such as endoscopic surgery. Page 63 of 65 Personal Information Philippe Henrot, MD Department of radiology Centre Alexis Vautrin 6, ave de Bourgogne 54511 Vandoeuvre-les-Nancy France phone: 0033 383598341 fax: 0033 383598550 e-mail: [email protected] References 1.Bodino C, Jankowski R, Grignon B, Jimenez-Chobillon A, Braun M. Surgical anatomy of the turbinal wall of the ethmoidal labyrinth. Rhinology 2004;42(2):73-80. 2.Roux FX, Behm E, Page P, Laccourreye O, Pages JC, Brasnu D. [Adenocarcinomas of the ethmoid sinuses. Epidemiological data]. Ann Otolaryngol Chir Cervicofac 2002;119(5):271-80. 3.Choussy O, Ferron C, Vedrine PO, Toussaint B, Lietin B, Marandas P, et al. GETTEC Study Group. Adenocarcinoma of Ethmoid: A GETTEC retrospective Multicenter Study of 418 Cases. Laryngoscope 2008;118:437-443 Page 64 of 65 4.Jankowski R, Georgel T, Vignaud JM, Hemmaoui B, Toussaint B, Graff P, et al. Endoscopic surgery reveals that woodworkers' adenocarcinomas originate in the olfactory cleft. Rhinology 2007;45(4):308-14. 5.Georgel T, Jankowski R, Henrot P, Baumann C, Kacha S, Grignon B, et al. CT assessment of woodworkers' nasal adenocarcinomas confirms the origin in the olfactory cleft. AJNR Am J Neuroradiol 2009;30:1440-4. 6.Wenig BM, Heffner DK. Respiratory epithelial adenomatoid hamartomas of the sinonasal tract and nasopharynx: a clinicopathologic study of 31 cases. Ann Otol Rhinol Laryngol 1995;104:639-45. 7.Lima NB, Jankowski R, Georgel T, Grignon B, Guillemin F, Vignaud JM. Respiratory adenomatoid hamartoma must be suspected on CT-scan enlargement of the olfactory clefts. Rhinology2006; 44:264-9 8.Delbrouck C, Fernandez Aquilar S, Choufani G, Hassid S. Respiratory epithelial adenomatoid hamartoma associated with nasal polyposis. Am J Otolaryngol 2004;25:282-4. 9.Dulguerov P, Calcaterra T. Esthesioneuroblastoma: the UCLA experience 1970-1990. Laryngoscope 1992;102:843-9. 10.Lawson W, Ho BT, Shaari CM, Biller HF. Inverted papilloma: a report of 112 cases. Laryngoscope 1995;105:282-8 11.Damman F, Pereira P, Laniado M, Plinkert P, Löwenheim H, Claussen CD. Inverted papilloma of the nasal cavity and the paranasal sinuses: using CT for primary diagnosis and follow-up. AJR 1999;172:543-8 Page 65 of 65