Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
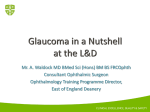
ORIGINAL STUDY Diode Laser Cyclophotocoagulation for Nanophthalmic Chronic Angle Closure Glaucoma Shani Golan, MD and Shimon Kurtz, MD Purpose: To retrospectively evaluate the results of diode laser cyclophotocoagulation (CPC) in patients with nanophthalmos. Methods: The data on all bilaterally nanophthalmic patients who underwent diode laser CPC in our department between 2004 and 2012 were retrieved and evaluated. Results: Four patients fulfilled study entry criteria. All 4 were females aged 58, 62, 68, and 74 years. The mean preoperative intraocular pressure of 46 ± 5.7 mm Hg dropped to 16.2 ± 1.5 mm Hg at the final follow-up visit (43.5 ± 16 mo). Visual acuity did not change in 2 patients and slightly worsened in the other 2. Choroidal detachment was observed in all patients between 7 and 14 days after the procedure and lasted for 1 to 2 months, resolving spontaneously in 2 patients and following systemic steroid treatment in the other 2. Conclusions: Diode laser CPC was an effective treatment for patients with glaucoma secondary to nanophthalmos. Key Words: nanophthalmos, chronic angle closure glaucoma, diode laser cyclophotocoagulation (J Glaucoma 2015;24:127–129) N anophthalmos is a rare condition that results in reduced dimensions of the globe in all directions caused by developmental arrest after closure of the fetal fissure. It usually affects both the eyes and may be inherited as autosomal dominant, autosomal recessive, or sporadically.1 Nanophthalmos is distinguished from other types of microphthalmia and anterior microphthalmos based on a shorter than normal axial length (r20.5 mm), a shallow anterior chamber, high lens/eye volume ratio, and moderate to severe hyperopia.1 Patients with nanophthalmos are prone to develop a chronic painless type of glaucoma in middle age, probably due to the natural increase in lens size.2,3 The management of angle closure glaucoma in these patients is problematic, mainly due to the frequent complication of choroidal effusion and nonrhegmatogenous retinal detachment following glaucoma surgery as well as the risk of postoperative ciliary-block malignant glaucoma.2–5 We report the efficacy and safety of diode laser cyclophotocoagulation (CPC) treatment in nanophthalmic glaucoma patients. Received for publication August 4, 2012; accepted April 8, 2013. From the Department of Ophthalmology, Tel Aviv Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. Disclosure: The authors declare no conflict of interest. Reprints: Shani Golan, MD, Department of Ophthalmology, Tel Aviv Medical Center, Sackler Faculty of Medicine, Tel Aviv University, 6 Weizman Street, Tel Aviv 64239, Israel (e-mail: shanigola2@ gmail.com). Copyright r 2013 Wolters Kluwer Health, Inc. All rights reserved. DOI: 10.1097/IJG.0b013e31829da1ba J Glaucoma Volume 24, Number 2, February 2015 PATIENTS AND METHODS We evaluated the medical records of all patients with diagnosis of glaucoma with nanophthalmos at the Glaucoma Service of Tel Aviv Medical Center treated in our department between 2004 and 2012. The Ethics Committee for Human Research at the Tel Aviv Medical Center approved this study. Patients who did not undergo diode CPC surgery or had inadequate records to ensure at least 1 year of follow-up were excluded from the study. The patients’ charts were reviewed for sex, age at initial diagnosis, family history, visual acuity, refraction, gonioscopy, intraocular pressure (IOP), and axial length was recorded in all of the 4 patients. Echographic findings (anterior chamber depth, lens, and scleral thickness) were also recorded in 1 patient (#1). Fundus examination, glaucoma medications, and postoperative complications were recorded in all 4 patients as well. There were 4 patients who fulfilled the study entry criteria. They had all undergone laser iridotomy as the initial procedure for primary angle closure as well as bilateral cataract surgery with posterior chamber intraocular lens implantation. They had been unsuccessfully treated for elevated IOP with IOP-lowering agents (3 to 4 drugs) before undergoing laser treatment. Diode CPC was performed by a single surgeon (S.K.), using 15 to 20 shots 2.5 seconds and 2000 mW, with the patient under general anesthesia. RESULTS The study patients’ operated eye, pre-CPC and postCPC best-corrected visual acuity (BCVA) and IOP findings, procedure-related complications, and length of follow-up are listed in Table 1. All patients were known nanophthalmic patients, with an axial length ranging between 17 and 19 mm (mean 18 mm). The refraction ranged between + 6.00 and + 8.00 in both the eyes. All 4 patients were treated with 1 antihypertensive medication before hospitalization in both eyes. They were all hospitalized due to uncontrolled and elevated IOP (mean 46 ± 5.7 mm Hg; range, 38 to 51 mm Hg) in 1 eye. The fellow eye had normal IOP ranging between 12 and 17 (mean 15.25 mm Hg). The BCVA on the first day of hospitalization ranged between 20/50 and 20/100 in that eye and between 20/50 and 20/200 in the fellow eye. The anterior segment examination was normal in all the patients except patient #1 who had irregular configurated pupils in both eyes. All patients had an open patent iridotomy in both eyes, and gonioscopy revealed closed angles (Shaffer 0) in both eyes with elevated IOP in 1 eye only. They all had posterior chamber artificial intraocular lens in both eyes. The posterior segments were normal in both eyes of 3 patients, whereas patient #1 had an epiretinal membrane in both of her eyes. All patients www.glaucomajournal.com | 127 Golan and Kurtz J Glaucoma Volume 24, Number 2, February 2015 TABLE 1. Characteristics of the Study Patients* 1 2 3 4 Age (y) Eye Pre-IOP (mm Hg) Pre-BCVA Post-IOP (mm Hg)w Post-BCVA Complications Follow-up (mo) 74 62 68 58 Left Right Right Right 51 38 49 46 20/100 20/60 20/60 20/50 15 18 17 15 20/100 20/100 20/100 20/60 CD, fibrin CD, fibrin CD CD 60 42 50 22 *All the patients were females. wPost=post diode CPC. BCVA indicates best-corrected visual acuity; CD, choroidal detachment; IOP, intraocular pressure; Post, postcyclophotocoagulation (last follow-up measured); Pre, prediode cyclophotocoagulation. received treatment with topical with topical as well as systemic antiglaucoma medications [eg, oral acetazolamide 500 mg once daily, topical b-blocker (timolol 0.5%), carbonic anhydrase inhibitor (dorzolamide), and prostaglandin analogue (latanoprost)], for the elevated IOP, but with no benefit. Because of the failure of conservative treatment, each patient underwent diode laser photocoagulation (IRIS Medical OcuLight SL 810 diode laser system; IRIDEX Corp., Mountain View, CA) (15 shots 2.5 s and 2000 mW) under general anesthesia. They were all followed up for >20 months (mean 43.516; range, 22 to 60 mo). All 4 patients had developed choroidal detachment on day 7 to 14 after the procedure, which was verified by ultrasound examination. Figure 1 demonstrates the choroidal detachment observed on ultrasonography in patient #1. The choroidal detachment resolved a few weeks later (range, 4 to 8 wk) without any treatment in patient #2 and #3 and with treatment by systemic steroids which were slowly tapered off in patient #1 and #4. There was no change in the BCVA from the beginning to the end of follow-up in 2 patients and worsened by 2 lines in the other 2 (from 20/60 to 20/100 in both). BCVA ranged from 20/60 to 20/100 at the last follow-up visit. The final IOP ranged from 15 to 17 mm Hg in the operated eye (mean 16.2 ± 1.5 mm Hg), and all patients were treated with 0-1 topical antihypertensive medication at the end of follow-up. COMMENTS Nanophthalmos is a form of microphthalmos in which the axial length of a grossly normal globe is <20.5 mm. The size of lenses in nanophthalmos is within normal range, therefore the lens/globe volume ratio, which is 4% for normal eyes, increases up to the pathologic level of 10% to 30%. Nanophthalmos is often associated with varying degrees of angle closure glaucoma. A relative pupillary block etiology secondary to a posterior “pushing” mechanism is the most common cause of angle closure glaucoma, which eventually leads to peripheral anterior synechia (PAS) formation.2–5 The anterior chamber angle can also be closed by physical displacement of the peripheral iris by anteriorly rotated ciliary processes when nanophthalmos presents with annular ciliochoroidal effusion and ciliary body detachment.6 Response to medical treatment is poor, and miotics may even make the condition worse by relaxing the lens zonules in these patients.1–3 Laser iridotomy is very beneficial in the early stage of glaucoma for eliminating the pupillary block component before the occurrence of PAS formation.2–4 Argon laser peripheral iridoplasty is another laser treatment of choice if the anterior chamber remains appositionally closed after iridectomy.7 Intraocular surgery may be required when PAS have developed. Surgery is considered as a last resort because it is often followed by a considerable number of complications. Sudden decompression of the globe during surgery may trigger the development of massive uveal effusion, which may lead to secondary retinal detachment, intraocular hemorrhage and malignant glaucoma, and loss of vision. Singh et al3 found that 9 of the 15 patients who had filtration surgery for glaucoma failed to achieve control and that 13 suffered visual loss. The association of nanophthalmos with uveal effusion was first reported by Brockhurst.8 The uveal effusion may FIGURE 1. Representative ultrasound of patient #1 illustrating choroidal detachment following diode cyclophotocoagulation. 128 | www.glaucomajournal.com Copyright r 2013 Wolters Kluwer Health, Inc. All rights reserved. J Glaucoma Volume 24, Number 2, February 2015 develop either from the thickening of sclera and the reduced scleral permeability to proteins, or from the dense collagen around the vortex veins and the resulting compression of venous drainage channels. Thickening of the sclera has been implicated in the pathogenesis of uveal effusion and serous retinal detachment in patients with nanophthalmos.9–12 The application of diode laser CPC in the setting of nanophthalmic angle closure glaucoma has not been reported in the literature. The treatment of angle closure glaucoma by diode CPC in our above-described patients led to lowering of the IOP. It also led to the development of choroidal detachment that was treated with steroids and eventually resolved. The final visual acuity remained the same in 2 patients and worsened by 2 lines in the other 2. We administered general anesthesia to all patients because of the risk of local anesthesia increasing intraorbital pressure. In light of the potentially grave complications of glaucoma surgeries in patients diagnosed as having nanophthalmic chronic angle closure glaucoma, treatment with diode CPC may offer a means of lowering IOP with fewer complications. REFERENCES 1. Duke-Elder S. Anomalies in the size of the eye. In: Duke-Elder S, ed. System of Ophthalmology. St Louis, MO: CV Mosby; 1964:488–495. Copyright r Diode CPC for Nanophthalmic Glaucoma 2. Kimbrough RL, Trempe CS, Brockhurst RJ, et al. Angleclosure glaucoma in nanophthalmos. Am J Ophthalmol. 1979; 88:572–579. 3. Singh OS, Simmons RJ, Brockhurst RJ, et al. Nanophthalmos: a perspective on identification and therapy. Ophthalmology. 1982;89:1006–1012. 4. Jin JC, Anderson DR. Laser and unsutured sclerotomy in nanophthalmos. Am J Ophthalmol. 1990;109:575–580. 5. Auffarth GU, Blum M, Faller U, et al. Relative anterior microphthalmos: morphometric analysis and its implications for cataract surgery. Ophthalmology. 2000;107:1555–1560. 6. Burgoyne C, Tello C, Katz LJ. Nanophthalmia and chronic angle closure glaucoma. J Glaucoma. 2002;11:525–528. 7. Ritch R, Chang BM, Liebmann JM. Angle closure in younger patients. Ophthalmology. 2003;110:1880–1889. 8. Brockhurst RJ. Nanophthalmos with uveal effusion: a new clinical entity. Arch Ophthalmol. 1975;93:1289–1299. 9. Yamani A, Wood I, Sugino I, et al. Abnormal collagen fibrils in nanophthalmos: a clinical and histologic study. Am J Ophthalmol. 1999;127:106–108. 10. Shiono T, Shoji A, Mutoh T, et al. Abnormal sclerocytes in nanophthalmos. Graefes Arch Exp Ophthalmol. 1992;230: 348–351. 11. Stewart D III, Streeten BW, Brockhurst RJ, et al. Abnormal scleral collagen in nanophthalmos. An ultrastructural study. Arch Ophthalmol. 1991;109:1017–1025. 12. Yue BY, Kurosawa A, Duvall J, et al. Nanophthalmic sclera. Morphologic and tissue culture studies. Ophthalmology. 1986; 93:534–541. 2013 Wolters Kluwer Health, Inc. All rights reserved. www.glaucomajournal.com | 129