Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
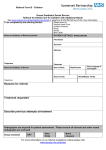
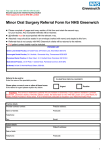
PLEASE RETURN THIS FORM TO: Warwickshire Special Care Dental Service, Whitnash Lodge – Booking & Access Team Leamington Hospital Heathcote Lane, Heathcote, Warwick, CV34 6SR, or Fax: 01926 339230 WARWICKSHIRE SPECIAL CARE DENTAL SERVICE REFERRAL FORM Patients with disabilities, medical conditions or phobia/tolerance problems at severe end of the spectrum only Patient’s Details: (Mr/Mast/Mrs/Miss/Ms) Dentist Details: Surname: Referring Dentist: Forename: Dental Practice Address: Address: Postcode: Phone No: Date of Birth: NHS No: General Practitioner: Postcode: Phone No: Date of Referral: Please tick: Urgent Routine (Referral will be returned if not provided) Name: GP Address: Postcode: Phone No: Is the patient in pain? No Yes - Mild /Intermittent Yes – Severe/Continuous Has the patient had an Orthodontic opinion? Yes (Please attach a copy) No (Please refer to our Special Care Referring guidelines on how to proceed) Relevant Medical History & Medication: REASON FOR REFERRAL: (Radiographs are required for extractions of adult teeth – please ensure they are available with this referral) Physical Access: Unable to access surgery/transfer to dental chair? Phobia/Tolerance Problems: Yes No (Only accepted with evidence of reasonable attempts having been made to provide treatment for those who can tolerate examination. Patients who demonstrate an ability to tolerate the aspects below on assessment will not be accepted.) Has a dental examination been possible with the patient lying supine? If yes, what attempts have been made to provide dental treatment? Which aspects is the patient unable to tolerate? Instrumentation Air Water Other - Please detail: Suction Yes No Local Anaesthetic Please ensure you have completed and attached all essential relevant information. Failure to do so may result in the referral being declined.