Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
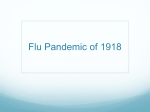
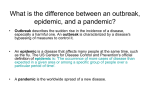
Vaccine xxx (2006) xxx–xxx Estimation of the reproductive number of the Spanish flu epidemic in Geneva, Switzerland G. Chowell a,∗ , C.E. Ammon b , N.W. Hengartner a , J.M. Hyman a b a Theoretical Division (MS B284), Los Alamos National Laboratory, Los Alamos, New Mexico 87545, USA Institute of Social and Preventive Medicine, Faculty of Medicine, CMU, P.O. Box 1211, Geneva 4, Switzerland Abstract The 1918 influenza pandemic known as the “Spanish Flu” has been the worst in recent history with estimated worldwide mortality ranging from 20 to 100 million deaths. Using epidemic modeling and hospital notification data during the 1918 influenza pandemic in the Canton of Geneva, Switzerland, we estimated the reproductive numbers of the first and second waves of influenza infection to be R1 = 1.49 (95% CI: 1.45–1.53) and R2 = 3.75 (95% CI: 3.57–3.93), respectively. Our estimates indicate that containment of the next influenza pandemic could require strict interventions that include effective isolation strategies in hospitals and reductions in the susceptibility of the general population. © 2006 Elsevier Ltd. All rights reserved. Keywords: Influenza; Spanish flu; Reproductive number 1. Introduction In the Canton of Geneva, Switzerland, the influenza pandemic of 1918/1919 infected more than 50% of the population, and the mortality rate was highest in the age group 21–40 years particularly in males [1]. The Canton of Geneva is located in the southwestern corner of Switzerland, surrounded in its majority by France, and covers an area of 282 km2 . The first wave occurred in July 1918 the second deadliest wave in October–November 1918 and the third wave was observed at the end of 1918. The symptoms presented during the second wave were more severe than during the first and third waves. We use a compartmental epidemic model that considers under-reporting of cases that are not diagnosed in hospital clinics and the relative transmissibility from asymptomatic cases. The model is calibrated using epidemic data of the 1918 influenza pandemic in the Canton of Geneva, Switzerland. We estimate the reproductive number for the first influenza wave to be 1.49 (95% CI: 1.45–1.53) and for the second ∗ Corresponding author. Tel.: +1 505 606 1483; fax: +1 505 665 5757. E-mail address: [email protected] (G. Chowell). wave 3.75 (95% CI: 3.57–3.93). Our estimated reproductive numbers indicate that containment of the next influenza pandemic could require the simultaneous implementation of aggressive interventions targeting reductions in the transmissibility of infectious cases and the susceptibility of the general population. 2. Materials and methods 2.1. Model description We use a compartmental epidemic model (Fig. 1) to describe the transmission dynamics of pandemic influenza. Individuals are classified in the following epidemiological classes: Susceptible, exposed, clinically ill and infectious, asymptomatic (partially infectious), hospitalized, recovered, and death from influenza. The data are the daily number of new hospitalizations during the 1918 influenza pandemic in Geneva, Switzerland. Random mixing in the population is assumed. The birth and natural death rates are assumed to have common value (average life expectancy of 60 years in 1917 [2]), and the population is assumed to be initially completely susceptible. Recovered individuals from the first wave 0264-410X/$ – see front matter © 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.vaccine.2006.05.055 JVAC-6288; No. of Pages 4 2 G. Chowell et al. / Vaccine xxx (2006) xxx–xxx Fig. 1. Schematic representation of the transition of individuals (indicated by arrows) among the different epidemiological states during an influenza pandemic. are assumed protected to the second wave [1,3]. A proportion of latent individuals progress to the clinically infectious class, and the rest of the latent individuals progress to the asymptomatic class. Hospitalized individuals are assumed infectious since there is no evidence of the effectiveness of interventions, and disruptions in the sanitary and medical sectors were common [1]. Clinically infectious individuals are hospitalized or recover without being diagnosed (e.g., mild infections, hospital refusals [1]). Hospitalized individuals (reported) either recover or die from influenza. The mortality rates were adjusted according to the case fatality proportion. 2.2. Demographic and epidemic data The 1917 census reports that the population size of the Canton of Geneva in 1917 was 174,673, which is about 42% of today’s population (Dubois J. E-mail communication. Office Cantonal de la Statistique–Genève. July 11, 2005). Daily epidemic data for the Canton of Geneva was obtained from the mandatory notifications registry in Switzerland [1] during the period July 1918–February 1919. The overall case fatality of the Spanish flu in Geneva was 4.2% [1]. Since we do not have the separate case fatality proportions for the spring and the fall waves of infection of the 1918 influenza pandemic in Geneva, we used the case fatality for the first (0.7%) and second (3.25%) waves of the 1918 influenza pandemic in UK as reported by Gani et al. [4]. 2.3. Parameter estimation We estimated the transmission rate (rate at which new infections are generated through the mixing of infectious and susceptible individuals), the recovery rate, the diagnostic rate, the relative infectiousness of asymptomatic cases, the proportion of clinical cases, and the initial numbers of exposed and infectious individuals by fitting our model to the epidemic curve of the cumulative number of influenza cases of the first and second waves of the 1918 influenza pandemic in Geneva, Switzerland [7]. The advantage of using the cumulative over the daily number of new notifications is that the former somewhat smoothes out known reporting delays on weekends and national holidays. The average latent period was fixed to 1.9 days [3], and the birth and natural death rates were fixed according to the mean life expectancy of Geneva, Switzerland in 1917 (60 years [2]). 2.4. The reproductive number The basic reproductive number is commonly denoted as R0 and defined as the number of secondary cases generated by a primary infectious case during its entire period of infectiousness in a completely susceptible population. Therefore, when R0 is greater than one, an epidemic can occur while a basic reproductive number smaller than one will not sustain an epidemic. One of the goals of public health interventions is to reduce this quantity to a number less than one as soon as possible. Here, we denote the reproductive number for the first wave as R1 and for the second wave as R2 . Notice that R1 can be referred to as the basic reproductive number of the first wave because we assume the population is completely susceptible at the beginning of the epidemic. However, R2 is not a basic reproductive number because individuals that recover from the first influenza wave are assumed protected to the second wave [3], reducing the effective population size. Reproductive numbers are useful in determining the magnitude of changes needed to bring an epidemic under control [5]. Once epidemiological parameters are estimated, the reproductive number of the first and second wave of infection can be obtained by plugging in the estimated parameter values into a formula of the reproductive number. A formula for the reproductive number can be derived from the structure of the compartmental model (Fig. 1) using standard methods in mathematical epidemiology [6]. For simplicity, we can write the reproductive number as the sum of the contributions to infection from the individuals in each of the three infectious categories. The contribution of the infectious and not hospitalized individuals to the reproductive number is given by: Rinfectious i = (fraction of symptomatic cases) × (transmission rate) ×(mean time in infectious class) G. Chowell et al. / Vaccine xxx (2006) xxx–xxx 3 Table 1 Estimated epidemiological quantities and their corresponding confidence intervals for the first and second waves of the 1918 influenza pandemic in the Canton of Geneva, Switzerland Epidemiological quantity First wave Transmission rate (1/days) Mean time in infectious class (days) Mean time in asymptomatic class (days) Mean time in hospital (days) Relative transmissibility from asymptomatic cases (0,1) Fraction of symptomatic cases (0,1) Fraction of symptomatic cases that are hospitalized (0,1) 8.0 1.21 2.94 0.92 0.003 0.10 0.062 Estimate Second wave 95% CI (7.74, 8.26) (1.07, 1.30) (2.78, 3.13) (0.68, 1.41) (0–0.011) (0.8, 0.12) (0.059, 0.065) Estimate 5.75 0.38 2.22 1.64 0.014 0.36 0.29 95% CI (5.27, 6.23) (0.36, 0.41) (1.89, 2.70) (1.38, 2.01) (0–0.034) (0.32, 0.40) (0.28, 0.31) Confidence intervals were constructed using bootstrap techniques. The contribution of the hospitalized individuals to the reproductive number is given by: hospitalized Ri = (fraction of symptomatic cases that are hospitalized) ×(transmission rate) × (mean time in hospital) The contribution of the asymptomatic individuals to the reproductive number is given by: asymptomatic Ri = (fraction of asymptomatic cases) × (transmission rate) ×(relative transmissibility from asymptomatic cases) ×(mean time in asymptomatic class) The overall reproductive number is given by: hospitalized Ri = Rinfectious + Ri i Fig. 2. Model fit to the daily number of hospital notifications during the first two waves of the 1918 influenza pandemic in the Canton of Geneva, Switzerland. asymptomatic + Ri where the index i denotes either the first (i = 1) or the second wave (i = 2) of the influenza pandemic. Table 1 contains the estimates of the epidemiological quantities that comprise the reproductive number formulas above for the first and second waves of the 1918 pandemic influenza in Geneva. The estimated epidemiological parameters and their corresponding confidence intervals for the first and second waves are given in Table 1. Using our epidemiological estimates and the formula for the reproductive number given above, our estimate of the reproductive number for the first wave is 1.49 (95% CI: 1.45–1.53) and for the fall wave is 3.75 (95% CI: 3.57–3.93). 3. Results 4. Discussion We have estimated relevant epidemiological parameters from hospital notification data of the 1918 influenza pandemic in Geneva, Switzerland with a compartmental epidemic model (Fig. 1) by minimizing the distance between the actual and predicted number of hospital notifications. The population is divided in a number of groups or compartments namely susceptible, exposed, clinically ill and infectious, asymptomatic (partially infectious), hospitalized, recovered, and death from influenza. Our epidemic model describes well the observed epidemic data (Fig. 2). We used a compartmental epidemic model and hospital notification data of the 1918 influenza pandemic in Geneva, Switzerland to estimate the reproductive numbers of the first and second waves of infection. Our model accounts for underreporting of cases that are not diagnosed in hospital clinics and the relative infectiousness of asymptomatic individuals. Our model assumes random mixing of the population. This standard random mixing assumption is difficult to avoid without greatly complicating the mathematical model and having 4 G. Chowell et al. / Vaccine xxx (2006) xxx–xxx explicit information of the structure of the interactions among different subpopulations. Our estimate of the reproductive number for the second wave was significantly larger than that of the first. This is in agreement with the higher severity of symptoms and deadly complications observed during the second wave [1]. Estimates for the reproductive number in the Unites States using mortality data range between 2 and 3 [3], and in the UK, Gani et al. [4] estimated a basic reproductive number of 2 for the first wave and 1.55 for the second wave. Our results indicate that containment of the next influenza pandemic could require the simultaneous implementation of multiple component interventions that include effective isolation of hospitalized cases and reductions in the susceptibility of the general population through, for example, increasing hygiene, using protective devices (e.g., face masks), prophylactic antiviral use, and vaccination (if available). References [1] Ammon CE. Spanish flu epidemic in 1918 in Geneva. Switzerland Eur Surveill 2002;7:190–2. [2] Robine JM, Paccaud F. Nonagenarians and centenarians in Switzerland, 1860–2001: a demographic analysis. J Epidemiol Community Health 2005;59:31–7. [3] Mills CE, Robins JM, Lipsitch M. Transmissibility of 1918 pandemic influenza. Nature 2004;432:904–6. [4] Gani R, Hughes H, Fleming D, Griffin T, Medlock J, Leach S. Potential impact of antiviral use during influenza pandemic. Emerg Infect Dis 2005;11:1355–62. Available from http://www.cdc.gov/ncidod/ EID/vol11no09/04-1344.htm. [5] Anderson RM, May RM. Infectious diseases of humans. Oxford: Oxford University Press; 1999. [6] Diekmann O, Heesterbeek J. Mathematical epidemiology of infectious diseases: model building, analysis and interpretation. John Wiley & Sons; 2000. [7] Chowell G, Ammon CE, Hengartner NW, Hyman JM. Transmission dynamics of the great influenza pandemic of 1918 in Geneva, Switzerland: assessing the effects of hypothetical interventions. J Theor Biol, in press.