Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
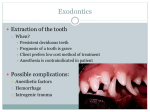
Radiographs in Endodontics Normal radiographic anatomy Interpretation Application Importance of endodontic radiography Specialized radiographic techniques Normal radiographic anatomy Radiographic recognition of the disease requires Sound knowledge of the radiographic appearance of normal structures Teeth Cervical burn out Diffuse radiolucent areas Mesial & distal -cervical regions Between the edge of the enamel cap & crest of alveolar ridge. Supporting structures Lamina Dura Tooth socket -- thin radiopaque layer of dense bone X-ray beam passes tangentially through many times the thickness of thin wall Thickness and density–the amount of occlusal stresses LD--- wider and more dense(heavy occlusion) LD--- thin and less dense (not subjected to occlusal function) Intact LD indicates vital pulp Alveolar crest Gingival margin of the alveolar process that extends between the teeth ---radiopaque line Not more than 1.5mm from CEJ of adjacent teeth Periodontal ligament space Radiolucent space between tooth root and LD Varies in width— -patient to patient, - tooth to tooth, -location to location around one tooth. Maxilla Intermaxillary suture (median suture) Thin radiolucent line in the midline between two portions of premaxilla Extends from alveolar crest between central incisors Continues posteriorly between the maxillary palatine processes to the posterior aspect of hard palate Anterior nasal spine Periapical radiographs of max CI Midline,radiopaque About 1.5 to 2 cm from the alveolar crest Below the junction of the inferior end of nasal septum and inferior outline of nasal fossa Nasal fossa Lies just above the oral cavity Radiolucent Incisive foramen Nasopalatine or anterior palatine foramen Lies in the midline of the palate behind the central incisor Between the roots of CI Lateral fossa(incisive fossa) -- Gentle depression in the maxilla near the apex of LI –Appear diffusely radiolucent Nasolacrimal canal Formed by nasal and maxillary bones Seen on maxillary occlusal projections in the region of molars Maxillary sinus Air containing cavity lined with mucous membrane Three sided pyramid Base--medial wall adjacent to the nasal cavity Apex extending laterally into zygomatic process of maxilla Three sides are; Superior wall forming the floor of the orbit 2. Anterior wall extending above premolars 3. Post wall above the molar teeth and max tuberosity 1. Roots of molars usually lie in close apposition to max sinus Borders of max sinus appears as thin , delicate radiopaque line Zygomatic process Extension of lateral max surface that arises in the region of the apices of first and second molars on periapical radiographs– U shaped radiopaque line Open end directed superiorly Enclosed rounded end is projected in the apical region of first and second molar Pterygoid plate lies immediately posteriorly to tuberosity of maxilla radiopaque Mandible Symphysis Infantsradiolucent line through the midline of the jaw between the images of the forming deciduous CI Suture fuses by the end of first year of life Genialtubercles (mental spine) Lingual surface of the mand Spine shaped Well visualized in mand occlusal radiographs Periapical--radiopaque mass in the midline below Incisor roots Mental ridge Periapical radiographs of Mand CI--seen as 2 radiopaque lines sweeping bilaterally forward and upward toward the midline Mental fossa Radiolucent depression on the labial aspect of mandible between the alveolar ridge & the mental ridge Mental foramen Anterior limit of inferior dental canal Round, oblong, slit-like or irregular Half way between lower border of mand and crest of alveolar process, (region of the apex of second premolar) When mental foramen is projected over one of the premolar apices it may stimulate periapical disease ( continuity of lamina dura around the apex— indicates absence of periapical abnormality) Mandibular canal Dark linear shadow with thin radiopaque superior and inferior borders cast by lamella of bone that bounds the canal Located jus inferior to apices of posterior teeth Application Diagnosis of hard tissue alterations Number,location,size,shape and direction of roots and root canals Localize hard to find or disclose unsuspected,pulp canals Locate a pulp ---receded or calcified Position of structures in F-L dimension Position and adaptation of primary filling point Evaluate -- final root canal filling Examination of lips,cheeks and tongue for fractured tooth fragments & foreign bodies Hard-to-find apex ---periradicular surgery Confirm foll periradicular surgery and before suturing ==tooth fragments and filling materials have been removed Follow up films ==outcome of treatment Viewing conditions Ambient light in viewing room should be reduced Mounted in a film holder Size of the view box should accommodate the size of the film Intense light source -- to evaluate dark regions of the film Magnifying glass --detailed information of small regions of the film Interpretation Wuehrmann review one structure at a time--- -- lamina dura Follow this structure all the way around the first tooth on the left and then around the next tooth and the next until the full film or full mouth survey is scanned Findings --normal or changed. Proceed to next structure ---crowns of teeth Each crown is evaluated independently Radiographic coronal evaluation includes depth of caries and restoration with respect to pulp Crest of alveolar process should then be followed --from left to right --upper to lower --structures outside the alveolar process should be evaluated - sinuses ,floor of nose,foramina and so Tracing the dark periodontal ligament space will reveal number, size and shape of the roots While observing the root -periradicular lesions -root defects --anomalies,fractures and external resorption Number,size shape,curvature of all the canals Internal resoption, pulp stones, linear calcification and open apices Anatomic structures can be mistaken for pulpoperiradicular lesions Expoure at Different angulation and by pulp testing Radiolucencies not associated with the root apex --projected away from the apex by varying the angulation Importance of Endodontic Radiography Radiograph-- paramount importance Excellent diagnostic films =before treatment =during treatment = after treatment INITIAL RADIOGRAPHS Studied carefully Not only as an aid in diagnosis but also a “blue print” for what to expect during treatment Identifying presence and nature of pathosis Size and shape of pulp chamber Direction and angulation of the canals as they leave the pulp chamber Obstructions -pulp stones Curvature of roots and approximate length of tooth Distal or mesial inclination of the roots CONFIRMATORY RADIOGRAPHS Second most valuable film after initial entry into crown ,access opening appears to be headed away from the canal orifice ---evaluate alignment Confirmatory length- of- tooth film Position of the file tip in relation to root apex Shows whether the file is in the canal as intended or has entered a root perforation Confirmatory trial point radiograph Confirms the visual and tugback judgement of the fit of initial filling point Provides the final opportunity to judge the advancement of instrumentation Confirmatory post- treatment film Determines the length, density, configuration and quality of obturation Should be made before a coronal restoration is placed Imp during surgery-- searching for root tips, lost filling material, location of root apexes during trephination or apicoectomy Post- treatment evaluation radiograph Evaluate the changes taking place periradicularly Abnormal or unusual findings -----retreat either surgically or non surgically Re-treatment radiography Before initiating re-treatment--fresh film Tooth , perforations, broken instruments, failure to obturate, ineffective surgery. RADIOGARPHS FOR TRACING Supplemental radiographs --chronic draining sinus A GP cone (30 size) is placed into the tract with cotton forceps until solid stop is felt Periodontal lesions may also be traced radiographically --depth and extent A silver point of size 30 is placed into the tract until it is stopped by the sulcus depth or bone and is then radiographed Helps to Determine the depth of pocket Amount of supporting bone on a periodontally involved tooth Which root of a multirooted teeth-amputated or treated with periodontal surgery Buccal object rule-cone or tube shift technique, clarks rule or SLOB rule visualize the anatomy of superimposed structures, roots, pulp canals vary the horizontal angulation of central ray of x-ray beam Clarks rule states that -- the most distant object from the cone (lingual) moves toward the direction of the cone Radiographic diagnosisperiradicular lesions Pulpal inflammation and necrosis -periradicular changes Widening of PDL space usually at the apex Apical external resorption Apex --slightly blunted to gradually resorbed It may also be obliquely resorbed or have a cupped out appearance chewed appearance of the tree felled by a beaver Moth eaten appearance -- tooth by accident was rippled loose from its ligament and /or was replanted Condensing osteitis Exact opposite of root resorption Teeth with chronic pulpal infl Root is blunted by inflammatory resorption and then this space is filled by osteosclerotic bone radiopaque appearance on X-ray films Foll successful RCT radiopacity slowly changes back to normal appearance Asymptomatic apical periodontitis Well circumscribed osseous lesion Radiographically-Thickening of PDL and resorption of lamina dura to destruction of apical bone Size varies from few mm to cm or larger in size Do not always appear on the periapex. Occasionally they are seen on the lateral surfaces of the root associated with lateral canal Asymptomatic apical abscess Larger, more diffuse and irregular radiolucent lesion Lesion may drain into mouth thru a sinus tract or extraorally onto to the neck or chin Apical cyst Lesion appear more circumscribed Move roots of the teeth laterally-PATHOGNOMONIC feature of cyst Lesions of non endodontic origin Pathologic changes may be mistaken for periradicular lesions of pulpal origin Non odontogenic cyst-globulomaxillary cyst, the midline palatal cyst and cyst of nasopalatine canal cysts are not associated with the exact root end ---move away from the root ends -horizontal angulation is varied To be further considered in D/D of cystsvitality of pulp Apical cyst-Non vital Non odontogenic cysts --traumatic injuries causes pulp death Periodontal lesion may be mistaken for periradicular lesion of endodontic origin Periodontal probe and pulp testerinvaluable method Place a silver or GP point in periodontal probe and take a radiograph If the lesion is traceable to the apex of the tooth and pulp responds to pulp testing-10 periodontal involvement Specialized radiographic techniques Direct digital radiography Direct replacement of an X-ray film with an electron image receptor or sensor and an image is displayed on the computer DDR makes use of a Solid state sensor, typically a CCD, Complimentary metal oxide silicone or a charge injection device connected by a cable to a computer, a monitor and a printer DDR sensor is packaged in a hard aluminium or plastic shell X-ray --is converted by a screen to green light transmitted through an optical fiber to CCD sensor CCD then converts green light to electrons that are deposited in electron wells for subsequent read out ,line by line by the electronics Advantage Instantaneous availability of images after exposure without removing sensor from the mouth Allows multiple angles to be taken --location of canals --identification of root curvatures --verification of working length --verification of obturation . Tangible benefits No dark room or processing equipment is needed Infection control procedures are reduced Duplicates are instantly made with absolute no loss in image quality Sensitivity of the receptors and digital nature of the image X- ray exposure Computers ===store and enhance the image Radiographic picture on the computer screen ====treatment Time savings Time is saved by not waiting for film processing Retakes -ease of retakes -instant -X-ray head ,patient and sensor are still in place Dose reduction -- low X-ray dosage Tooth length measurement Begin at the apex and advance the cursor toward the crown with the mouse computer --calculate a preoperative length in mm even around curvatures Sensor size small sensor size -comfortable for the pt,and easier for the assistance to place larger sensors -more difficult to place(rigidity) Digital subtraction radiography Uses a computer to assess, in two or more radiographs, pathologic changes that have taken place over a period of time 2 digital images to be compared are brought into computer software Stored in a numeric format in the computer memory compared mathematically Background images have not changed (crowns , fillings etc)--are subtracted which inturn highlights area that have changed (lesion size) Tomography it is a radiographic technique that essentially slices the teeth into thin sections computers then reassemble the sections to generate a three dimensional image Pulp spaces and roots B-L curvature, Shape of the canal space and location of the apical foramen An additional adv– -- elimination of specialized angled radiography -- All angled views will be simultaneously captured in one exposure Thank You