Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
MINISTRY of PUBLIC HEALTH of UKRAINE
VINNITSYA NATIONAL PIROGOV MEMORIAL
MEDICAL UNIVERSITY
It is "confirmed"
on a methodical meeting of
department of pediatric
dentistry
head-chair
doc.Filimonov Yu.V._____
" _______
_______ in20
Methodical recommendation for 4d year students
of dental faculty
Educational discipline
Module ¹
Rich in content module ¹
Topic
Course
Faculty
Autor
Pediatric surgery
1
1
Acute diseases of temporomandibular joint (arthritis),
disorders and management.
4
Dental
Isakova N.M.
Vinnitsya 2012
Actuality of theme .
Among disorders of TMJ first place belongs to processes of inflamatory origin
of various nature –specific, non specific, traumatic, non infectious, which can have
acute or chronic course .In acute arthritis all components of acute inflamation both
local and systemic –altered blood count,systemic immune response ..etc are observed.
Diagnostics of acute arthritis commonly does not cause specific difficulities, specially
and determination etiologic moments, for example previous acute otitis, parotits,
influenza, rheumatic attack, acute trauma ..etc .
1. Concrete aims:
1.A student must familiarize with the problem of realization of diseases of
temporomandibular joint for children, among the different age-related groups.
2. A student must know the features of anatomic structure of maxillufacial area for
the children of the different age-related groups and feature of physiology processes
for children. A student must know classification of diseases of temporomandibular
joint.
3. A student must lay hands on methodologies of the diseases of temporomandibular
joint for children.
4. A student must conduct differential diagnostics of the different urgent states and
render the first medical aid.
3.Educator aims:
1. To develop professional internalss and feelings of responsibility during realization
of treatment diseases of temporomandibular joint for children.
2. Able to carry out and psychological approach in-process with children
3 Base knowledges, abilities, habits which are necessary for study the topic.
Names of previous
disciplines
Skills are got
1. General anatomy
2. Gistology
3. Therapy, pediatrics
The structure of the maxillofacial
region, the blood and nerve supply
Histological structure of the oral
mucous cavity. The mechanism of
development
and
phase
of
inflammation
Know the features of a child's body.
Know the basic diseases of
importance
in
conducting
the
diagnosis of major dental diseases
4. Task for independent work during preparation to
employment.
4.1. List of basic terms, parameters, descriptions which
a student must master at preparation to employment :
Term
Determination
1. Impaired functions
of the joint
Results from dislocation –intra arthral cause ,or from
contracture of various origin-extra arthral cause
2.Dystrophic
degenerative process
Disgnated as sclerongenic or deforming arthrosis can be
primary or secondry
3.Mount peaks
Causing dramatic impairment of movement of the jaw
possiblity resulting incomplete dysfunction
4.2. Theoretical questions to employment:
1. Anatomo-physiologic features of TMJ
2.advantage and disadvantages of contemporary classifications of TMJ disorders
3.clinical signs and methods of treatment of acute and chronic arthritis of TMJ
4.pecular development and types of arthrosis of TMJ
5.main manifestation of dysfunctions of TMJ, views concerning their origin and
development
6.main methods of diffrential diagnosis of inflammatory, inflammatory-dystrophic
diseases and dysfunction of TMJ
4.3 Practical works (tasks)
To conduct the different types of the local anaesthetizing on phantoms.
5. A plan and organizational structure of lesson in
discipline.
№
1.
1.11.1
1.2
1.3
2.
3.
3.1.
3.2.
3.3
Stages of
Distribution Types of
Facilities of studies
employment
of time
control
15 min
practical
Text-books, methodical
Preparatory
tasks,
recommendations.
stage
situatioonal
OThe
tasks,
organizational
verbal
questions.
crossForming
of
examination
motivation.
at standart
Control of
list
of
initial level of
questions.
preparation.
Basic
55 min
stage.
Final stage
20 min
Control
of
eventual level
of preparation.
General
estimation of
studing
activity
of
student.
Informing of
students
about
the
theme of next
employment.
test tasks
Maintenance of theme
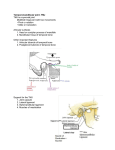
Anatomy
The temporomandibular joint (TMJ), also known as She craniomandibular
joint/articulation is peculiar to mammals. It is the articulation between the squamous
parto: the temporal bone and the head of the mandibular condyle. The mandibular
articulation is labelled as a bilateral diaithroidial or freely movable joint. It is also
considered as complex joint, because it involves two separate synovial joints (right
and left), in which there is a presence of intracapsular disc Viscus and both the joints
have to function in coordination. The TMJ articulation consists of a mandibular or
glenoid fossa, an articular eminence or tubercle, condyle, a separating disc, a joint
fibrous capsule and an extracapsular check ligaments.
Articulatory System
The articulatory system comprises of the following:
a.
Temporomandibular joint (TMJ)
b.
Masticatory and accessory muscles.
c.
Occlusion of the teeth.
The function is governed by sensory and motor branches of the third division of the
trigeminal nerve (mandibular nerve) and a few fibers of the facial nerve. The occlusion
of the teeth plays an important role in the function of the TMJ. Normally, the greatest
part of the force of mastication is borne by the dentition of the
jaws, but in case of occlusal disharmony, a great deal of force can be shifted to the
joint itself.
Mandibular (Glenoid) Fossa (Cranial Component)
Anteriorly, the articular eminence or tubercle, and posteriorly, a small conical
postglenoid tubercle.
Articular eminence It is a small prominence on the zygomatic arch. It is strongly
convex ant crop osteriorly and somewhat concave medio laterally.
Postglenoid tubercle It separates the articular surface of the fossa laterally from the
tympanic plate. And the tympanic plate separates the TMJ from the bony part of the
external auditory canal.
Glenoid fossa it has an anterior articular area formed by the inferior aspect of temporal
squama. Its surface is smooth, oval and deeply hollowed out and the bone is very thin
at the depth of the fossa. This roof of the glenoid fossa creates a partition between
middle cranial fossa and tire joint. The fossa is lined by a dense avascular fibroca
tillage. In cross section, the fossa and the eminence form S' posteroanteriorly.
Squamo-tympanic fissure separates it from tympanic plate, which forms a posterior
wall of the glenoid fossa.
Mandibular Component Mandibular Condyle
The articular part of the mandible is an ovoid condylar process (head) with narrow
mandibular neck. 11 is broad laterally and narrower medially. The medtolate-ral
dimension varies between 13 to 25 mm and anteroposterior width varies between 5.5
to 16 mm. The majority of human condyles {58%) are slightly convex superiorly, with
a radius of curvature greater than the distance from the medial to lateral poles.
Twenty-five per cent of condyles may be flat superiorly and approximately 12 per cent
are pointed or angular in shape and 3 per cent are bulbous or rounded in shape. The
surface of the articular eminence that most closely approximates the condyle is
consistently congruent with the surface of the condyle. The two condyles of a patient
may be asymmetric. A combination of flat condyle on one side with a convex condyle
on the other side is most common. The articular part of the condyle is covered by
fibrocartilaginous tissue and not with hyaline cartilage, as in most other joints in the
human body.
TMJ Capsule
TMJ capsule is a thin sleeve of fibrous tissue investing the joint completely. It is a
funnel-shaped capsule, which blends with the periosteum of the mandibular neck and
it envelops the meniscus. Tt is attached above anteriorly to the anterior border of the
articular eminence and posteriorly to the lip of the squamo-tympanic fissure and to the
anterior surface of the postglenoid process and also to the circumference of the cranial
articulating surface and bolow to the neck of the condyle, on the lateral as well as on
the medial aspect. Tnside this fibrous tissue capsule, there is a lining of silky synovial
membrane.
Ligaments
Lateral or Temporomandibular Ligament
TMJ capsule is reinforced by this main stabilising l igament. Tt extends downward and
backward from the articular eminence to the external and posterior side of the
condylar neck. Its posterior fibers are united with the capsular fibers. This ligament is
composed of collagenous fibers that have specific length and poor
ability to stretch, hence it maintains the integrity and limits the movement of TMJ. It
mainly Limits the anterior excursion of the jaw as well as prevents posterior
dislocation, hence it is called as 'check ligament' of TMJ. But in certain situations, if
the joint movements consistently function against ligament, then the ligament
elongates and diis can create change in the joint biomechanics and can lead to certain
pathologic changes.
Accessory ligaments make no contribution to joint activity.
Sphenomandibular ligament A flat band arising from the sphenoid spine and the
petrotympanic fissure, runs downward and medial to the TMJ capsule and gets inserted
on the lingula of the mandible. It is a remnant tif Meckel's cartilage.
Sphenomandibular ligament is mi important landmark during surgery, as internal
maxillary artery and auriculotemporal nerve lies between it and the mandibular neck.
Tlie stylomandibular ligament It is dense, thick band of the deep cervical fascia
extending from the styloid process to the mandibular angle.
Articular Disc or Meniscus
The TMJ is a diarthroidial synovial paired joint. This means that there are two joint
movements, which occur in separate compartments of this synovial joint and that one
joint cannot operate without the other.
The meniscus or an intervening disc divides the articular space into two compartments:
1. The hivcr or inferior compartment—condyiodiscal complex between tlie condyle and
the disc.
2. Thv upper (temporodiscnl) or superior compartment between the disc and the temporal
bone or glenoid fossa.
The disc is biconcave in the sagittal section. The superior surface is ennravoconvex to
match the anatomy of the glenoid fossa and inferior surface is concave to fit over the
condylar head. A detailed study by Rees in 1954 reported that the shape of the arriadar
disc or meniscus is like a school boy's or jockey's cap which overlaps the condylar head
.
Temporomandibular Joint (TMJ) Disorders
Classification
i. Intra-articular origin or intrinsic disorders.
ii. Extra-articular origin or extrinsic disorders. Extrinsic factors are those not directly
associated with the TMJ, whereas intrinsic factors relate to those conditions existing
within the confines of the capsule of the joint-Disorders due to Extrinsic Factors
Masticatory muscle disorders
a. Protective muscle splinting.
b. Masticatory muscle spasm (MPD syndrome).
c. Masticatory muscle inflammation (myositis).
Problems that result from extrinsic trauma
a. Traumatic arthritis
b. Fracture
i . Internal disc derangement
d. Myositis, myospasm
c. Tendonitis
f. Contracture of elevator muscle—myofibrotic contractures.
Because of these ex tra-articular factors the function of the TMJ may be hampered.
Whenever, there is a restriction of normal oral opening or inability to open the mouth
fully, the term trismus is used. Trismus is brought about by extraarticular causes and it
is also labeled as false ankylosis,Trismus is also defined as a condition in which muscle
spasm or contracture prevents opening of the mouth (due to infection or other
conditions which alter muscle structure).
Causes of trismus
1. Due to infection Orofacial infections around the joint area can bring about trismus or
limitation of oral opening. Odontogenic acute infections like pericoronitis, Ludwig's
angina, submasseteric and infratemporal abscess, etc. Chronic infections affecting the
jawrs also can bring about trismus. Tuberculous osteomyelitis of ramus and/or body
mandible, etc.
2. Trauma Fracture of the zygomatic arch may impinge on the coronoid process and
restrict the oral opening. Fracture of the mandible also can bring about trismus, because
of pain and tenderness or muscle spasm.
7
3. Inflammation Myositis or muscular atrophy can bring about trismus.
4. Myositis ossificans Following trauma, a haema-loma can be formed, within the fibers of
the masticatory group of muscles, especially in the masseter, which can progress into
ossification and the muscle stiffness. Clinical and radiographic examination will
confirm the presence of these changes.
5. Tetany Typical carpopedal spasm along with trismus can be seen due to hypocalcacmia.
6. Tetanus Following acute infection by Clostridium tetani, the typical lockjaw symptom
can be seen associated with other symptoms, because of persistent tome muscle spasm.
7: Neurological disorders Epilepsy, brain tumour, bulbar paralysis, embolic haemorrhage
in medulla oblongata can bring about trismus.
8. Psychosomatic trismus It is also known as trismus hystericus. Due to extreme fear,
anxiety associated with hysterical (its.
9. Drug induced trismus Strycluvinc poisoning can bring about spasms leading to trismus.
10.Mechanical blockage Elongation, exostosis, osteoma, osteochondroma of coronoid
process will cause mechanical blockage and interfere with the normal mandibular
movements.
11.Extra-articular fibrosis Chronic cervicofacial sepsis, postradialion therapy, ossification
of sphenomandibular ligament, bands of scars and burns of the face and neck region,
oral submucous fibrosis will lead toward progressive trismus.
classical clinical example of trismus is seen occasionally, following the injection of the
inferior alveolar nerve block with local anaesthetic agent. Bleeding, created by needle
puncture in the medial pterygoid muscle, produces a haematoma followed by fibrosis
and subsequent trismus. In most cases the haematoma is spontaneously resolved and
normal jaw function returns within a week or two. In some of the cases, under sedation
or general anaesthesia, manipulation of the jaw, with jaw stretcher may be required to
break up the adhesions and restore the function.
Disorders due to Intrinsic Factors
1. Trauma
a. Dislocation, subluxation
b. Hacmarihrosis
c. Intracapsular fracture, extracapsular fracture
2. Disc displacement
a. Anterior disc displacement with reduction
b. Anterior disc displacement without reduction
3. Arthritis
a. Osteoarthrosis (degenerative arthritis, osteoarthritis)
b. Rheumatoid arthritis
c. Juvenile rheumatoid arthritis
d. Infectious arthritis
4. Droelopmental defects
a. Condylar agenesis or aplasia unilateral bilateral
b. Bifid condyle
c. Condylar hypoplasia
8
d. Condylar hyperplasia
5. Ankylosis
6. Neoplasms
a. Benign tumours: osteoma, osteochondroma, chondroma
b. Malignant tumours: Chondrosarcoma, fibrosarcoma, synovial sarcoma.
Dislocation, Subluxation, Hypermobility of TM Joint
During normal or unstrained opening of the mouth, the condylar heads translate
forward to a position under the apices of the articular eminences. If oral opening proceeds
to its maximum capacity, the condylar heads move to the anterior slope of the articular
eminences in many normal individuals. F.M ur-.ion of the condylar heads beyond these
limits maybe viewed as abnormal and termed as dislocation. In contrast to the fracture
dislocation of the condylar head, here the intact condylar head is displaced out of glenoid
fossa, much anteriorly beyond articular eminence, but still remains within the capsule of
the joint. As far back as 3000 BC in Egypt, Hippocrates first reported a dislocation of the
mandible. His method of reduction has survived the ages and is still being used in modern
times. Mandibular condylar dislocation is uncommon, compared to the other joints in the
body. Its incidence is reported to be 3.1 per cent.
The dislocation can be unilateral or bilateral.
Anterior mandibular dislocation can be classified as
1. Acute
2. Chronic recurrent (habitual) subluxation
3. Long-standing.
The term luxation is also used for acute dislocation and the terms, subluxation or
liypermobillty or habitual chronic recurrent dislocation is substituted for the term
dislocation, when it is incomplete.
Causes of Acute Dislocation
a. Extrinsic forces or iatrogenic causes
b. Intrinsic or self-induced forces
Anterior acute dislocation of the condyle occurs, in which the normal anatomic
relationships within the joint have been completely disrupted,with the condyle lixed
anterior to the articular eminence. Relocation of the condyle in its normal position in the
glenoid fossa does not occur voluntarily, it can occur as a single acute event or as chronic
recurrent episodes.
Extrinsic or iatrogenic causes Acute dislocation is common and can be brought
about by a blow on the chin, while mouth is open, injudicious use of mouth gag during
general anaesthesia or excessive pressure on the mandible, during dental extraction can
lead to acute dislocation. It can be post-traumatic, spontaneous or associated with
psychiatric illness.
Predisposing factors Laxity of ligaments, capsule and abnormality of skeletal form.
Previous injuries, occlusal disharmonies can bring about laxity of the capsule. Flattened
eminence and shallow fossa, systemic diseases like Parkinson's disease, epilepsy, Ehlers9
Danlos syndrome, etc. can be the predisposing factors. The use of antipsychotic drugs may
cause extrapyramidal reactions and dislocation.
Clinical picture o f acute dislocation Dislocation is a dramatic event. It maybe
unilateral or bilateral. 1 listory of the patient may be diagnostic.
Unilateral acute dislocation It is characterized by difficulty in mastication and
swallowing. Speaking may be difficult and profuse drooling of saliva can be present in the
early stages. A deviation of the chin toward contralateral side is seen.The deviation
produces a lateral cross and open bite on the contralateral side .
Tlie mouth is partly open and the affected condyle cannot be palpable. In obese
person, absence of condyle from the glenoid fossa may not be apparent, but in others a
definite depression will be seen and felt in front of the tragus.
Bilateral acute dislocation It is associated with pain, inability to close the month,
tense masticatory muscles, difficulty in speech, excessive salivation, protruding chin I he
mandible is postmed forward and movements are restricted. There is a gagging of the
molaT teeth with the presence of anterior open bite. Difficulty in swallowing and drooling
of saliva is seen. Patient will complain of pain in the temporal region rather than the joint
and may be extremely apprehensive. The distinct hollow-ncss can be felt in both the
preauricular regions, Associated muscle spasm contributes to the fixed position of the
condyles.
Literature.
Basic:
1.Lectures which are read on the department of pediatric dentistry.
2. Pinkham J.R. Pediatric dentistry. – 2nded.- W.B. Sounders Company. – 1994.647 p.
3. Pediatric dentistry /Ed. R.R.Welbury.- Oxford, 1997 – 584p.
Additional:
1. Колесов А.А “ Стоматологія дитячого віку “ , 1978 ,ст. 44-63.
2. Дунаевський В.А. “Хірургічна стоматологія “ , 1979 ,ст. 111118.
3. Бернадский Ю.И. «Основы хирургической стоматологии», К.,
1998
4. Евдокимова А.И. «Руководство по стом. детского возраста»,
1976
10