Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
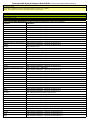
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
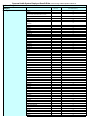
Quantity Limit List
Category
Analgesics
Anti-Emetic Products
Antineoplastic Agents
Antipsychotic Agents
Beta agonist inhalant and nebulizing
agents
Medication *
Stadol Nasal Spray
Ultram tablets
Anzemet 50mg & 100mg tabs
Emend 40mg (non-preferred)
Emend 80mg
Emend 125mg
Zolinza
Zydis / Zyprexa
All products (e.g. albuterol, metaproterenol)
Duoneb
Levalbuterol
Adderall XR 5mg, 10mg, 15mg (preferred)
Adderall XR 20mg, 25mg, 30mg (preferred)
Concerta all strengths except 36mg (preferred)
Concerta 36mg strength ONLY (preferred)
Central Nervous System (CNS)
Stimulants (effective 8-1-04)
Metadate CD all strengths (non-preferred)
Provigil all strengths (non-preferred)
Ritalin LA 20mg & 40mg (non-preferred)
Ritalin LA 30 mg (non-peferred)
Strattera 10mg, 18mg, 25mg, 40mg (Preferred)
Strattera 60mg, 80mg, 100mg (Preferred)
Vyvanse (all strengths) (non-preferred)
COX-2 Sparing Agents
Celebrex 50mg, 100mg & 200mg tabs
(non-preferred)
Estrogen patches
Granulocyte Colony-Stimulating Factor
HMG-CoA Reductase Inhibitors
Insulin
Narcotic Analgesics
(added per P& T action 1-6-04)
Nasal steroid inhalers
NSAIDS
68 capsules / month
34 capsules / month
34 capsules / month
68 capsules / month
Oxycontin 10mg and 20mg strengths
68 tablets / month
5 tablets / month
5 tablets / month
5 tablets / month
5 tablets / month
90 day supply for 1 copay
5 doses per chemo cycle
5 doses per chemo cycle
5 doses per chemo cycle
34 tablets / month
34 tablets / month
3 vials or 2 boxes of pens / copay
90 Oralets / month
68 capsules / month
11 patches per strength per month
84 tablets
136 capsules / month
204 tablets / month
204 tablets / month
136 tablets / month
180 tablets / month
All products (e.g. beclomethasone, flunisolide)
1 inhaler / month
Mobic 7.5mg & 15mg tabs (non-preferred)
Erectile Dysfunction Agents
Quantity Limit
5mL (2 bottles) / month
240 tablets / month
12 tablets / copay - 2 fills per month
5 capsules month
2 caps per month
1 cap per month
120 capsules per month
34 tablets per month
2 inhalers or bottles of solution / month
360 ml / month (120 vials)
288 ml / month (96 vials)
34 capsules per month
68 capsules per month
34 tablets per month
68 tablets per month
34 tablets per month
68 capsules per month (prior notification required)
34 capsules per month
68 capsules / month
Cialis (all strengths)
Levitra (all strengths)
Stendra (all strengths)
Viagra (all strengths)
Generic products
Granix
Neupogen
Neulasta
Caduet (all strengths) (non-preferred)
Crestor (all strengths) (non-preferred)
All products
Actiq (all strengths)
Avinza (all strengths)
Duragesic patches (all strengths)
Fentora
Kadian (all strengths)
MS Contin (all strengths)
Oramorph (all strengths)
Oxycontin (EXCEPT 10MG and 20MG)
Clarinex 5mg & Clarinex D 24 hr (non-preferred)
34 tablets per month
Clarinex D 12 hour
Xyzal 5mg (non-preferred)
Toradol 10mg tablets
68 tablets per month
34 tablets per month
20 tablets / month
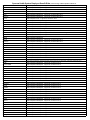
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Quantity Limit List
Category
Oral Contraceptives
Oral Steroid Inhalers
Proton Pump Inhibitors
Sedative / Hypnotic Agents
Medication
All products
All products
Dexilant all strengths (non-preferred PA
required)
Ambien all strengths (preferred
Ambien CR all strengths (non-preferred)
Lunesta all strengths (preferred)
Rozerem all strengths (non-preferred)
Sonata all strengths (preferred)
Amerge 1mg & 2.5mg tabs
Axert 6.26mg & 12.5mg tabs
Frova tabs (all strengths)
Imitrex Syringe
Imitrex 25mg, 50mg, and 100mg tabs
Imitrex Nasal Spray 5mg & 20mg
Selective Serotonin Receptor Agonist Imitrex Vials
Maxalt 5mg & 10mg tablets &
disintegrating tabs
Relpax 20mg & 40mg tablets
Zomig 2.5mg tablets
Zomig Nasal Spray
Zomig 5mg tablets & Zomig ZMT 5mg
Citalopram 40mg tablets (preferred)
fluoxetine 10mg (preferred)
fluoxetine 20mg (preferred)
fluoxetine 40mg (non-preferred)
Luvox and fluvoxamine 25mg tab
(non-preferred)
Luvox and fluvoxamine 50mg tab
(nonpreferred)
Luvox and fluvoxamine 100mg tab
(non-preferred)
Luvox CR 100mg & 150mg
Selective Serotonin Reuptake Inhibitor
Paxil 10mg tablets (non-preferred)
Medicaion Class / Antipsychotics
Paxil 20mg, 30mg, & 40mg tablets
(nonpreferred)
Paroxetine 20mg, 30mg, & 40mg tablets
(preferred)
Paxil CR 12.5mg, 25mg, & 37.5mg
(non-preferred)
(effective 2-1-06)
Smoking Cessation Products
* Generic products are subject to quantity limits
Quantity Limit
3 month supply / 3 copays
2 inhalers / month
34 capsules / month
34 capsules / month
34 capsules / month
34 capsules / month
34 capsules / month
34 capsules / month
9 tablets / Rx; 18 tablets / month
6 tablets / Rx; 12 tablets / month
9 tablets / Rx; 18 tablets / month
1 Kit (2 syringes) / Rx; 2 fills per month
9 tablets (each strength) / Rx; 18 tablets month
6 spray bottles (1 box) / month
5 vials (1 pack) per Rx; 10 vials/ per month
12 tablets / Rx; 24 tablets / month
6 tablets per fill / 12 tablets per month
6 tablets / 12 month
1 box of 6 UD sprays per month
3 tablets / month
45 tablets / month
34 tablets / month
90 capsules / month
68 tablets / month
34 tablets / month
68 tablets / month
102 tablets / month
34 tablets / month
34 tablets / month
68 tablets / month
68 tablets / month
68 tablets / month
Prozac 10mg tab/cap (non-preferred)
34 tablets / month
Prozac 20mg caps (non-preferred)
90 capsules / month
Prozac 40mg caps (non-preferred)
34 capsules / month
4 capsules / month
Prozac 90mg caps (non-preferred)
Symbyax all strengths (non-preferred)
Chantix (preferred)
34 capsules / month
up to 6 months per calendar year
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
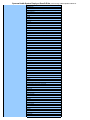
Preferred Drug List
Preferred
(Tier 1 or 2)
Category
SSRI's
Central Nervous System (CNS)
Stimulants
Congestive Heart Failure Agents
Diabetic Agents
HMG-CoA Reductase Agents
(Including combination products)
and the fenofibrate Agents
fluoxetine 10mg & 20mg
citalopram
sertraline
paroxetine
Celexa
Lexapro
Luvox
Paxil
Paxil CR
Prozac
Sarafem
Symbyax
Viibryd (PA REQUIRED)
methylphenidate
methylphenidate SR
amphetamine salts and Adderall XR
Strattera
Concerta (effective 6-1-05)
Daytrana
Focalin
Metadate CD
Nuvigil (not covered)
Provigil (requires prior notification)
Ritalin LA
Vyvanse
Agents except BiDil
BiDil
glimepiride
Avandia
Avandaryl
Exubera (Prior notification approval required)
Glumetza
Kombiglyze XR
Prandimet (ind. Products are preferred)
Insulin
Symlin
Bydureon (Prior notification & step edit)
Byetta (Prior Notification Required)
Victoza (not a covered benefit)
fenofibrate generic products
Pravachol
lovastatin
Lipitor 40mg & 80mg
Vytorin
Zetia
Zocor(simvastatin) (effective 5-1-05)
Advicor
Antara (step edit required generic fenofibrate)
Caduet
Crestor
Lescol
Lipitor 10mg & 20mg (step edit - simvastatin)
Livalo (not a covered benefit)
Mevacor
Pravigard PAC
Simcor
Tricor (step edit requires generic fenofibrate)
Trilipix (step edit requires generic fenofibrate)
Non Preferred (Tier 3)
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
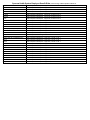
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
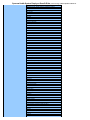
Preferred Drug List
Category
Preferred
(Tier 1 or 2)
Fluticasone propionate
Flunisolide
Beconase AQ (Step edit - use of generic product)
Flonase (Step edit - use of generic product)
Nasacort AQ (Step edit - use of generic product)
Nasonex (Step edit - use of generic product)
Rhinocoft Aqua (Step edit - use of generic product)
Omnaris (Step edit - use of generic product)
Veramyst (Step edit - use of generic product)
Acetic Acid Agents (indomethacin capsule,
sulindac, diclofenac delayed release tablet,
tolmetin)
X
X
X
X
X
X
X
Fenemates (meclofenamate)
Oxicams (piroxicam)
Proprionic Acid Agents (flurbiprofen,
ibuprofen, naprosyn sodium tablet, fenoprofen,
ketoprofen)
Pyranocarboxylic Acid (etodolac tablet)
Misc (nabumetone)
Celebrex
Clarinex
Clarinex D 12 hour and 24 hour
Xyzal
X
X
Leukotriene Receptor Antagonist (step
Advair (available at tier 1 copay)
X
edit for class =use of nasal steroid inhaler OR other
asthma medication within previous 12 months)
Zyflo
X
Antiviral Agents
Acyclovir
Famvir- Step Edit - acyclovir first line therapy
Valtrex - Step Edit - acyclovir first line therapy
Epivir
Baraclude
Inhaled Nasal Steroids
Step edit requires use of generic product prior
to using a brand name agent.
NSAID Agents
Non-Sedating Antihistamine
(note the step edit for nasal steroid
inhalers {fluticasone or flunisolide} is
use of one generic nasal steroid
inhaler before using a brand name
product)
Hepatitis B Agents
Non Preferred (Tier 3)
X
X
X
X
X
X
X
X
X
X
Zyflo CR
X
X
X
X
X
X
(Tier 2 if patient had a 60 trial of Epivir within the previous 90
days)
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
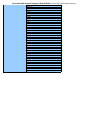
Preferred Drug List
Category
Sedative Hypnotics - Non
Barbiturate
Combination Products
Preferred
(Tier 1 or 2)
Flurazepam
Temazepam
Triazolam
Sonata
Ambien
Ambien CR
Lunesta
Rozerem
ibuprofen and oxycodone individually
X
metformin and glipizide
X
pravastatin and aspirin
X
X
X
X
Combunox (ibuprofen/oxycodone)
X
Exforge (amlodipine / valsartan)
X
Metaglip (metformin and glipizide)
X
Pravigard PAC (pravastatin and aspirin)
Antispasmodic Agents
X
Ditropan & Ditropan XL
Detrol & Detrol LA
X
Enablex
X
X
Sanctura & Sanctura XR
X
Toviaz
X
Bisphosphonates -
alendronate
(Bone resorption suppression agents)
risedronate
X
Forteo (PA required)
X
X
Atelvia
not a covered benefit
Boniva
Neuropathic Pain Agents (effective 9-
Non Preferred (Tier 3)
X
X
X
X
X
Neurontin
15-05)
X
X
X
Lyrica
(Tier 2 if patient has had a 60 day trial of Neurontin (gabapentin)
in the last 90 days)
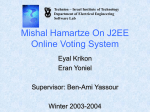
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Preferred Drug List
Preferred
(Tier 1 or 2)
Category
Misc Agents
Actoplus Met XR
Altabax
Alvesco HFA Inhaler / Alvesco Inhaler (step edit trial of all formulary inhaled steroid asthma products)
Non Preferred (Tier 3)
X
X
X
Amturnide
Antara
Apriso
X
X
X
Astragraf XL (step edit = immediate release
tacrilimus
X
Azilect
Azor
B-Nexa
Breo Ellipta
Bepreve
Brovana
Calafol RX
Centany
Citranatal Products
Clarifoam EF
Cleeravue -M
Clobeta + Plus
Coartem
Combigan
Coreg CR
Cosopt PF
Dificid (Step edit - course of oral Vancomycin)
Dulera
Dutoprol
Edarbi
Epidou
Equetro
Exalgo
Fexmid
Gelnique
Horizant
Jentadueto
Keppra XR
Kombiglyze XR
Lamictal XR
Lavoclen-4 and Lavoclen-8
Lovaza
Maxaron Forte
Metrogel Combo Package
Metvixia
Moviprep
Multaq
Nesina
Nicomide
Omnaris
Omontys
Onglyza
Onsolis
Otosporin
Ostiva
Otosporin
Oxandrin
Patanase Nasal Spray
Prepopik
Pristiq
Profera OB
Pyrlex and Pyrlex PD
Rapaflo
Remesense
Renvela
Requip XL
Rosac
Saphris
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Brand Name Products available at
the Generic Tier 1 ($7.00) Copay
Rate
Excluded Products
Savella (step edit)
Seradex
Seroquel XR
Servira
Signafor
X
Sklice (step edit - use of Lindane or permethrin)
Somatuline Depot
Sprycel
Stavzor
Supervite EC
Symbicort
Taclonex
Tasigna
Tribenzor
Trilpix
Tudorza Pressair
Twynsta
Udamin
Ultram ER
Vascepa
Veramyst
Voltaren Gel
Xerese
Xeljanz (step edit - MTX)
Ziana
Zioptan
Zymine XR and DXR
Zyclara
Accolate
Advair Diskus
Alphagan P 5mL botlle ONLY (Quantity limit of 2 bottles / copay)
Aricept
Atacand
Auvi-Q Auto-Injector
Copaxone 20mg (Copaxone 40mg is not a covered benefit)
EpiPen and EpiPen Jr (Quantity limit of 2 pens / copay)
Flovent
Nexium (caps tier 1, susp tier 2)
Novolin R, N and 70/30 Vials ONLY
Accuhist products
Ala-Hist products
Alcortin A
Aldex products
Allfen products
Allerx products
Aldex products
Alodox
Aloquin
Ambifed Products
Amrix
Analpram P and Advanced
Aplenzin
Aquoral
Asmalpred Plus
Atelvia
Avidoxy DK
Bifillin G
Biomed
Brisdelle
Brovex Products
Bystolic
Capcof
Carbaphen
Cardiotek Products
Centratex
Cleanse and Treat products
Clindareach
X
X
X
X
x
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
CNL 8 topical
Codiclear DH
Comfort PAC - Meloxicam
Copaxone 40mg (Copaxone 20mg is covered on the tier 1)
Cotab products
Coraz
Corvite FE
Corzall
Dallergy products
Desonil + Plus
Desowen
Dexall
Dexodryl
Dailyvite 5000
Neudexta
Dexilant
Diclegis
Differin products for members > 29 yrs of age. Tier 3 for all others
Digex NF
Doryx
Duac CS
Duet DHA Stuartnatal
Duexis
Duovit DHA
Dytan CD
Egrifta
Embeda
Endal CD
Endometrin
Entereg
Entex
Epiceram
Evamist
Extendryl products
Fanapt
Ferralet 90
Flector Patch
Folbee Plus
Fosteum
Fovex
Fulyzaq
Gattex
Gralise
Hemangeol
Hetlioz
HC Guai
Hyaltopic
Hydrocortisone /Lidocaine in Coleus Kit
Ibudone
IC400; IC 800
Intermezzo
Iprivask
J-Coff DHC
J-Max Products
J-Tan D HC
Jalyn
Juvisync
Juxtapid
Kapidex / Dexilant
Kerol Products
Lazanda
LidoCort KIT
Limbrel
Livalo
Lycelle
M-End Max
Manuvit SP
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Maxichlor PSE DM
Maxifed products / Maxiflu products / Maxiphen products
Medent-DMI
Mi-Omega NF
Minocin Kits
Momexin
Momexin
Moxatag
Myalept
Nalfrx
Nasofed / Nasotuss
Nasohist products
Natelle Plus
Neo HC
Neutrahist Products
Niravam
Notuss product line
Nucynta / Nucynta ER
Nuvigil
Nutridox
Nutrestore
Obagi - C
Omeclamox-Pak
Optinate
Oraxyl
Orenitram
Ortho-Nesic
Papfyll
Pediatex TDM
Pedipirox-4
Pennsaid Topical
Peranex HC
PhenFlu products
Physician Therapeutics products
Polytussin DHC
Pramine FQ
Prefera-OB
Prenate products
Prenatal vitamins with DHA supplements
Probarimin QT
Prolinia
Protect Cardio / Protect CMB2/Ceramide/Protect Iron/ Protect Bone
Pryflex
Pylera
Quinzyme
Radigel
Rayos
Re Dualvit products
Relcof DN PE
Renatabs with Iron
Reocyte Plus
Respi-tann products
Rezyst IM
Rhinahist
Rinnovi
Rosadan
Rosula products
Rowasa KITS
Rybix ODT
Ryzolt (tramadol preferred; Ultram ER tier 3)
Salex
Salvax Duo products
Samsca
Scalacort DK
Solaraze Gel
Solotuss
Strovite Advance + D
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Subsys
Sudates-G
Sumadan / Sumaxin CP
Sympak products
Tachosil
Tandem DHA
Tear Again
Terbinex
Tersi Foam
Tirosint
Tozal
Treximet
Trital SR
Tussicaps
Tizanidine (Comfort Pac)
Ultravate PAC
Uloric
Umecta
Vanacof products
Vanoxide HC Kit
V-Hist / V-Cof
Velphoro
Vimizim
Vimovo
Viravan products
Vitamax
Vitaphil
Viva DHA
Xolegel DUO and Corepak
Xyralid products
Zamicet
Zenieva
Z-Care
Zinotic
Zinx
Zotex-D
Z Tuss 2
Zypram
Zytaze
Zytopic
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Benefit Exclusions
Compounded Products
Cosmetic Agents - Medications used for cosmetic purposes are not covered. (e.g. Propecia)
Vitamins - OTC Vitamins are not covered - Prescription vitamins may be covered
SPHN covers the following Over-the-Counter Medications ($5.00 Copay for a 28-34 days supply, depending on package size)
Nicotine Patches, Lozenges, and Gum (quantity limit of 2 boxes per fill)
OTC Prilosec and OTC omeprazole
loratadine tablets and liquid
Prior Notification Medications (all Specialty Pharmacy Medications require prior notification)
Medication
Abstral
Actemra
Adempas
Adcirca
Afinitor
Ampyra
Arcalyst
Aplenzin
Information
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to MedImpact. If approved, covered on Tier 2
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to MedImpact. If approved, covered on Tier 2
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to MedImpact. If approved, covered on Tier 3
Astagraf XL (step edit - generic tacrolimus)
Submit request to MedImpact. If approved, covered on Tier 3
Aubagio
Benlysta
Bosulif
Brilinta
Brintellix
Submit request to MedImpact. If approved, covered on Tier 3
Brovana
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to PHP
Submit request to MedImpact. If approved, covered on Tier 3
Submit request to Plan. If approved, covered on Tier 3
Submit request to Plan. If approved, covered on Tier 3
Bydureon
Submit request to MedImpact. If approved, covered on Tier 3
Butrans
Submit request to MedImpact. If approved, covered on Tier 3
Byetta
Submit request to MedImpact. If approved, covered on Tier 3
Carbaglu
Submit request to MedImpact. If approved, covered on Tier 3
Castagon
Submit request to MedImpact. If approved, covered on Tier 3
Chemotherapy oral brand name agents
Submit request to PHP - Health Helps
Cimzia
Submit request to MedImpact. If approved, covered on Tier 2
Compounded Prescriptions
Not a covered beneft with the exception of oral liquids, which may be covered.
Cometriq
Submit request to MedImpact. If approved, covered on Tier 3
Daliresp
Submit request to MedImpact. If approved, covered on Tier 3
Dificid
Submit request to MedImpact. If approved, covered on Tier 3 (requires tx with oral vanco first)
Duavee
Submit request to MedImpact. If approved, covered on Tier 3
Egrifta
Submit request to MedImpact. If approved, covered on Tier 2
Emend 40mg
Submit request to MedImpact. If approved, covered on Tier 3
Emsam
Submit request to MedImpact. If approved, covered under Tier 3. Oral seligiline is preferred
Enbrel
Submit request to MedImpact. If approved, covered on Tier 2
Erivedge
Submit request to MedImpact. If approved, covered on Tier 3
ESA Agents
Prior Authorization Required. Submit request to Plan
Exalago
Submit request to MedImpact. If approved, covered on Tier 3
Famvir
Submit request to MedImpact. If approved, covered on Tier 3.
Fentora
Submit request to MedImpact. If approved, covered under Tier 3.
Fetzima
Submit request to MedImpact. If approved, covered under Tier 3.
Firazyr
Submit request to MedImpact. If approved, covered under Tier 3.
Flolan
Submit request to MedImpact. If approved, covered on Tier 2
Forteo
Submit request to MedImpact. If approved, covered on Tier 2
Fortesta
Submit request to MedImpact. If approved, covered under Tier 3.
Fycompa
Submit request to MedImpact. If approved, covered under Tier 3.
Gilenya
Submit request to MedImpact. If approved, covered under Tier 3.
Gilotrig
Submit request to MedImpact. If approved, covered under Tier 3.
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Grastek
Submit request to MedImpact. If approved, covered under Tier 3.
Growth Hormones
Submit request to MedImpact. If approved, covered under Tier 3.
Hizentra
Submit request to MedImpact. If approved, covered on Tier 2
Humira
Submit request to MedImpact. If approved, covered on Tier 2
Iclusig
Submit request to MedImpact. If approved, covered under Tier 3.
Imbruvica
Submit request to MedImpact. If approved, covered under Tier 3.
Incivek
Submit request to Plan. If approved, covered on Tier 2
Inlyta
Submit request to MedImpact. If approved, covered under Tier 3.
Isentress
Submit request to MedImpact. If approved, covered under Tier 3.
Jakafi
Submit request to MedImpact. If approved, covered under Tier 3.
Jublia
Submit request to MedImpact. If approved, covered under Tier 3.
Kalbitor
Submit request to the Plan. If approved it is covered under the medical side.
Kalydeco
Submit request to MedImpact. If approved, covered under Tier 3.
Kuvan
Submit request to MedImpact. If approved covered on Tier 3. Need diagnosis verification
Latuda
Submit request to MedImpact. If approved, covered under Tier 3.
Letairis
Submit request to MedImpact.
Lipichol
Submit request to MedImpact. If approved, covered under Tier 3.
Mervasco
Submit request to MedImpact. If approved, covered under Tier 3.
Myrbetriq
Submit request to MedImpact. If approved, covered under Tier 3.
Neupogen
Submit request to MedImpact. If approved, covered on Tier 2
Neulasta
Submit request to MedImpact. If approved, covered on Tier 2
NPlate
Submit request to PHP
Olysio
Submit request to MedImpact. If approved, covered under Tier 3.
Onfi
Submit request to MedImpact. If approved, covered under Tier 3.
Onsolis
Submit request to MedImpact. If approved, covered on Tier 3
Opana
Submit request to MedImpact, include documentation showing superiority over other opioids. If approved, covered under Tier 3.
Opsumit
Submit request to MedImpact, include documentation showing superiority over other opioids. If approved, covered under Tier 3.
Oralair
Submit request to MedImpact. If approved, covered on Tier 3
Orencia SUBQ
Submit request to MedImpact. If approved, covered on Tier 3
Otezla
Submit request to MedImpact. If approved, covered on Tier 3
Otrexup
Submit request to MedImpact. If approved, covered on Tier 3
Pertzye
Submit request to MedImpact. If approved, covered on Tier 3
Picato
Submit request to MedImpact. If approved, covered on Tier 3
Potiga
Submit request to MedImpact. If approved, covered on Tier 3
Prilosec
Submit request to MedImpact. If approved, covered on Tier 3
Procysbi
Submit request to MedImpact. If approved, covered on Tier 3
Promacta
Submit request to PHP
Promalyst
Submit request to MedImpact. If approved, covered on Tier 3
Provigil
Submit request to MedImpact. If approved, covered on Tier 3
Ragwitek
Submit request to MedImpact. If approved, covered on Tier 3
Ranexa
Submit request to MedImpact. If approved, covered on Tier 3
Ravicti
Submit request to MedImpact. If approved, covered on Tier 3
Relistor
Submit request to MedImpact. If approved, covered on Tier 3
Remodulin
Submit request to MedImpact. If approved, covered on Tier 2
Revatio
Submit request to MedImpact. If approved, covered on Tier 2
Samsca
Submit request to MedImpact. If approved, covered on Tier 3
Sancuso
Submit request to MedImpact. If approved, covered on Tier 3
Simponi
Submit request to MedImpact. If approved, covered on Tier 2
Signifor
Submit request to MedImpact. If approved, covered on Tier 3
Sirturo
Submit request to MedImpact. If approved, covered on Tier 3
Sovaldi
Submit request to MedImpact. If approved, covered on Tier 3
Stelara
Submit request to MedImpact. If approved, covered on Tier 3
Stivarga
Submit request to MedImpact. If approved, covered on Tier 3
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Suboxone
Submit request to MedImpact. If approved, covered on Tier 2
Synalar TS
Submit request to MedImpact. If approved, covered on Tier 3
Tafinlar
Submit request to MedImpact. If approved, covered on Tier 3
Tanzeum
Submit request to MedImpact. If approved, covered on Tier 3
Tecfidera
Submit request to MedImpact. If approved, covered on Tier 3
Thalomid
Submit request to MedImpact. If approved, covered on Tier 3
Thelin
Submit request to MedImpact. If approved, covered on Tier 2
Tivicay
Submit request to MedImpact. If approved, covered on Tier 3
Tracleer
Submit request to MedImpact. If approved, covered on Tier 2
Tykerb
Submit request to MedImpact. If approved, covered on Tier 3
Valchlor
Submit request to MedImpact. If approved, covered on Tier 2
Valtrex (step edit - acyclovir)
Submit request to MedImpact. If approved, covered on Tier 3
Vandetanib
Submit request to MedImpact. If approved, covered on Tier 2
Ventavis
Submit request to MedImpact. If approved, covered on Tier 3
Victrelis
Submit request to Plan. If approved, covered on Tier 2
Victoza (step edit - Byetta/Bydureon)
Submit request to MedImpact. If approved, covered on Tier 3
Viibryd
Submit request to MedImpact. If approved, covered on Tier 2
Vimpat
Submit request to MedImpact. If approved, covered on Tier 3
Votrient
Submit request to MedImpact. If approved, covered on Tier 2
Weight Loss Medications (Legend only)
Submit request to MedImpact
Xalkori
Submit request to MedImpact. If approved, covered on Tier 3
Xenazine
Submit request to MedImpact. If approved, covered on Tier 2
Zegerid
Submit request to MedImpact. If approved, covered on Tier 3
Zelboraf
Submit request to MedImpact. If approved, covered on Tier 3
Zithranol
Submit request to MedImpact. If approved, covered on Tier 2
Zontivity
Submit request to MedImpact. If approved, covered on Tier 3
Zykadia
Submit request to MedImpact. If approved, covered on Tier 3
Zytiga
Submit request to MedImpact. If approved, covered on Tier 3
Sparrow Health System Employee Benefit Rider (current through 7/30/2014 Updated 7/3/2014 srk
Medication Extended Supply List
Please Note:
Generic dispensed when available. Brand name in most cases only listed for name recognition.
*Asterisked agents do not currently have a generic available.
I.
100 Units or 34 days supply, whichever is greater
Antidiabetic Agents
Chlorpropamide (eg. Diabinese)
Glipizide (Glucotrol)
Glyburide (Micronase/Diabeta)
Metformin (Glucophage)
Antihypertensives
Atenolol (eg. Tenormin)
Diltiazem (Dilacor XR only)
Hydrochlorothiazide /
Triamterene (eg.Dyazide/Maxzide)
Nifedipine (Adalate CC only)
Nitroglycerine (eg. Nitrobid/Nitrostat)
Propranolol (eg. Inderal)
Verapamil (Verapamil SR only)
Cardiac Agents
Digoxin
Procainamide HCl (Procan/Pronestyl)
Quinidine
Diuretics
Bumetanide (Bumex)
Chlorthalidone (eg. Hygroton)
Chlorothiazide (eg. Diuril)
Furosemide (eg. Lasix)
Hydrochlorothiazide (eg. Hydrodiuril)
Estrogen and Hormone Therapy
Esterified Estrogens (eg. Estratab, Estrace, Ortho-est)
Conjugated Estrogens Maximum 3 packs
Anti-inflamatory agents
Ibuprofen (eg. Motrin)
Naproxen (eg. Naprosyn)
Naproxen Sodium (eg. Anaprox)
Anti-Lipid Agents
Atorvastatin (Lipitor)
Fluvastatine (Lescol)*
Gemfibrozil (Lopid)
Lovastatin (Mevacor)
Pravastatin (Pravachol)
Simvastatin (Zocor)
(eg. Premarin*, Premaphase*, Prempro*)
Medroxyprogesterone (Provera)
H2 Blockers
Cimetidine
Ranitidine
Hyperuricemia/Gout agents
Allopurinol (eg. Zyloprim)
Potassium Chloride
(eg. Kay Ciel/Slow K/K Dur/ Micro K/Klotrix)
Bronchodilators
Theophylline (eg. Theodur/Slo-bid)
II.
200 Units or 34 day supply, whichever is greater
Isoniazid (eg. INH)
Levothyroxine (eg. Levothroid/Synthroid)
Para-Aminosalicylic acid (eg. PAS)
Phenytoin (eg. Dilantin)
Primidone (eg. Mysoline)
Propylthiouricil (eg. PTU)
Thyroid (eg. Armour Thyroid)