Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
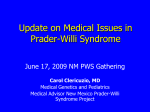
Therapies In PWS Jennifer Miller, MD Pediatric Endocrinology University of Florida Agenda • • • • Growth hormone treatment Provigil N-acetylcysteine New research into hyperphagia treatments Growth Hormone Treatment • GH treatment has benefits at any age on body composition, metabolism, cognitive function GH deficiency – effects on brain and cognition • Compared with controls, children with isolated GH deficiency (mean age 8.8 yrs) had lower Full-Scale IQ, Verbal Comprehension, Processing Speed, and Movement-Assessment Battery for Children. • Verbal Comprehension Index scores correlated significantly with insulin-like growth factor-1 and insulin-like growth factor binding protein-3 standard deviation scores in isolated GH deficiency. • Children with isolated GH deficiency had smaller splenium of the corpus callosum, left globus pallidum, thalamus and hippocampus . Growth Hormone for infants with PWS • Data suggests that GH deficiency that is untreated prior to childhood may result in abnormalities in brain structure and cognition. • Standard recommended starting dose is 1 mg/m2/day. • On standard starting dose of 1 mg/2/day fat mass declines initially, but then increases after 2 yrs of treatment. Whereas on a higher dose of 1.5 mg/m2/day the fat mass continues to decline over time, indicating that higher doses may be more beneficial for infants over time. GH in infants • GH treated infants had improved mental and motor development compared to controls. • Those with lowest motor development have the most profound improvement on GH. • Hand and foot length never completely normalize compared to NL population, whereas arm span and tibia length completely normalize Why is it beneficial for infants to start GH treatment despite adequate growth? • GH decreases ghrelin (hunger hormone) which is high even in infants with PWS, so may alter the natural course of the appetite progression in PWS. • Data in PWS mice shows hypoglycemia and deficits in insulin secretion in infancy – GH increases insulin and glucose levels, which may be why it is beneficial for infants in terms of cognitive development. • GH treatment shortens the initial failure-to-thrive phase of PWS • May impact brain development as well as cognition. Other Benefits • Data from Carrel et al and Hokken-Koelega et al, shows that GH treatment for infants improves IQ and psychomotor development. • We found that individuals treated with GH before age 1 had decreased fat mass, lower BMI, and higher resting energy expenditure as they age, compared to those treated after age 1, indicating that early treatment with GH may help prevent or ameliorate the obesity associated with PWS. GH Effects on Cognition • GH treatment significantly improves abstract reasoning and visuospacial skills in children. • With no treatment there is a decline in of certain cognitive skills in adolescence with PWS, but GH treatment prevents that decline. GH in Adults with PWS • GH treatment improves muscle mass and decreases body fat in adults with PWS. • Most common side effect of adult treatment was edema. • Insulin and glucose levels increased during treatment, but no increased incidence of diabetes. • Few patients had headache and myalgia. • Contraindications to GH therapy in adults with PWS are morbid obesity, severe untreated obstructive sleep apnea. 5 years of adult GH therapy All patients had a mild increase in insulin resistance on GH. 2 developed glucose intolerance on GH 1 patient developed Type 2 diabetes (was in the non-GH treated group). Cognitive Effects – Adult GH • Improvement in mental speed and flexibility and motor performance • When GH stopped parents documented impairment in physical and social status as well as overall functioning • Parents reported improvement in self-control and both parents and patients reported increased vitality on GH. Patients reported improvement in overall quality of life. Monitoring IGF-1 levels • IGF-1 is a surrogate marker for GH. • IGF-1 increases significantly over years of treatment and is above the normal range in the great majority of individuals with PWS after 2 years of treatment. • Reducing GH dose causes increases in body fat and decreases in muscle mass, so it is suggested to reduce the dose only if the IGF-1 levels are >2 standard deviations above the mean. • We recommend monitoring IGF-1 levels every 3-6 months in infants and children and every 6-12 months in adults. GH and sudden death • In 2003 a series of deaths on children who had recently started GH treatment was reported. • Several other reports of sudden death occurring in sleep within 1-3 months after starting GH treatment followed this initial report – the majority of individuals were obese males. • Martin Ritzen suggested the cause may be GH causing increased IGF-1 levels, resulting in lymphoid tissue growth (tonsils/adenoids) which would lead to obstructive sleep apnea. • We and others looked at this issue and did find some association between high IGF-1 levels and tonsil/adenoid hypertrophy, but no worsening of sleep apnea with GH treatment. So….is it risky to start GH? • There are no difference in the causes of death between those who are treated with GH vs. those who are not. • Major causes of mortality in PWS include: respiratory insufficiency or infection (61% of children), cardiac arrest, sudden unexplained death, infections, choking (5-8%), ruptured/necrotic stomach. • Premature mortality peaks in newborn/early infancy and adulthood, increased in males – obesity is a factor in most. • Therefore, we do need to be cautious when starting GH in infants and adults, to monitor closely especially during respiratory infections. Other Treatments Provigil (Modafinil) • Most typical stimulants cause adverse effects in individual with PWS (skin-picking, tics) • Provigil works well and thus far, has been safe and effective in this population. • Has shown significant benefit when given prior to therapies and also helping with cognition in school. • Can robustly activate fronto-cortical areas involved in higher cognitive functions and a network of pro-arousing areas • Risk of severe allergic reaction/rash in young children. Modafinil • Double-blind placebo controlled studies indicate that modafinil improves visuospacial memory accuracy and problem solving ability. • Improves mood and improves responsiveness to SSRI’s for patients with depression. • Improves planning and decision making. • Improves enjoyment of task performance. • May help impulse control. Modafinil • The memory enhancing properties might be the result of glutamatergic and dopaminergic increased neuronal activation in the hippocampus and in the prefrontal cortex respectively. • Other neurotransmitters are also activated by modafinil in various limbic brain areas, suggesting that the drug acts on these brain regions to influence emotional responses. Modafinil • Needs research to determine if these effects exist in PWS and if they may be amplified or attenuated in children with PWS. N-acetylcysteine • Through its role as a modulator of the glutamatergic system, cysteine influences the reward-reinforcement pathway. • Because of these functions, NAC may exert a therapeutic effect on psychiatric disorders allegedly related to oxidative stress (e.g., schizophrenia, bipolar disorder) as well as psychiatric syndromes characterized by impulsive/compulsive symptoms (e.g., trichotillomania, pathological nail biting, gambling, substance misuse). N-acetylcysteine NAC • More research needs to be done to determine if it will increase BDNF in PWS. • Other info: NAC can be oxidized easily, so if it smells bad it means it has been oxidized and is not as effective. • Pharma-NAC comes in individually sealed packets, so won’t be oxidized prior to use. Before and After New research into hyperphagia treatments Hyperphagia Conference • Much discussion about how to define hyperphagia and what tests to use to determine if medications are decreasing hyperphagia. • Mouse models are good to use to start with for treatments, but not always representative of what will happen in humans. FDA-approved medications • There are some already approved medications that may help with hyperphagia in PWS: – Metformin – Diazoxide Metformin Effects on interest in food Changes in hyperphagia questionnaire in children with PWS before and after metformin 3.5 3 Amount of change 2.5 Pt 1 Pt 3 2 Pt 5 Pt 6 1.5 Pt 8 Pt 9 1 Pt 10 Pt 12 0.5 Pt 13 0 Becomes upset when denied food Time thinking Time talking about Anxiety about Leaving food on about food food meals/eating plate Questions with the most change before and after metformin Feeling full Metformin – other effects • Decreases Alzheimer’s disease risk in obese mice with leptin resistance. • Reduces risk of some cancers. • Prevents ghrelin signaling pathway in hypothalamus. Diazoxide • The molecular endpoint of the leptin signaling pathway in hypothalamic neurons seems to be the K+-ATP channel. • Loss of Magel-2 gene appears to disrupt the leptin signaling pathway, which leads the body to believe that it’s in a constant state of starvation and contributes to: – – – – – hyperphagia, increased rate of adipose tissue deposition, decreased metabolic rate, abnormalities of the autonomic nervous system, growth hormone deficiency. Diazoxide • Diazoxide is a K+-ATP channel agonist, so may bypass the signaling defect in PWS and compensate for the absent leptin signal in the hypothalamus. • In studies of rats and chickens diazoxide treatment decreased hyperphagia significantly. Hypoglycemia • Hypoglycemia appears to play a role in the appetite and weight issues in PWS • Recent study indicates that 12% of infants had severe hypoglycemia (Blood Glucose <40 mg/dL) in newborn period • Those who had hypoglycemia seem to have a more difficult time with weight control and possibly behaviors as they get older. • Diazoxide increases blood glucose levels Diazoxide – other effects • K+-ATP channels in the plasma membrane and inner mitochondrial membrane play important roles in modulating neuronal excitability, cell survival, and cerebral vascular tone, so diazoxide may ameliorate effects of Alzheimer’s disease. • Individuals with PWS may be at higher risk for premature dementia/Alzheimer’s. White matter lesions in PWS Other Medications • Several potentially promising medications for hyperphagia including oxytocin, carbetocin, and other newer medications. • Some of these medications lower ghrelin which may work in conjunction with GH (which lowers ghrelin) to decrease hyperphagia in PWS. • Others may work more on body weight and have a secondary effect of decreasing hyperphagia by increasing signals of satiety to the brain. Medications for hyperphagia • Some medications may be able to be used in certain circumstances to reduce appetite but may have undesirable side effects if used long term. Oxytocin • Preliminary studies in adults suggest that OT may decrease appetite, as well as decreasing depressive symptoms and tantrums while increasing trust. • In infants OT may help decrease high ghrelin levels which may be beneficial in preventing hyperphagia later in life • Dosing regimen still uncertain – some doses appear to be ineffective • Studies of 5-10 year olds starting soon through the RDCRN Oxytocin Update • We have been working since April 2012 to start this trial, hoping to start March-June 2013 depending on paperwork progress/IRB. • For example: oxytocin could potentially cause low sodium levels (seizures). Also, medications from compounding pharmacies could be contaminated and dangerous. Carbetocin • Safer than oxytocin in terms of potential side effects. • Ferring Pharmaceuticals in interested in trial in PWS. • Will need to start with adults in phase 3. • Working on FDA-approval for trial in PWS. Beloranib • IND application and orphan-drug application for PWS pending. • Plans for study at UF to begin in March 2013. • Adults with obesity and hyperphagia who are able to be seen weekly in Gainesville for 12 week study. • Plan to enroll 20 adults for trial. Other Medications • Lorcaserin: selective serotonin 2C receptor agonist • Qnexa: phenteramine and topiramate • Contrave: buproprion and naltrexone • Exenatide: Delays gastric emptying, causes improvement in hypothalamic perception of satiety. Current Projects at UF • Natural History study on effects of GH (infantsadults) • Oxytocin (ages 5-10) • Hypoglycemia and Diazoxide (infants – adults) • Metabolomics in PWS vs. Siblings (infants – adults) • Ketogenic diet (ages 5-30) • Orexin (infants – adults)