Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
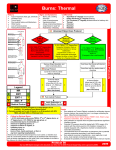
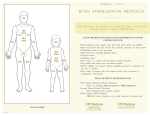
Estimating Percentage of Total Body Surface Area Exclude erythema The Lund-Browder chart is the most accurate method for estimating burn extent, and must be used in the evaluation of all pediatric patients. LUND-BROWDER CHART Relative Percentage of Body Surface Area Affected by Growth Age in years A-head (back or front) B-1 thigh (back or front) C-1 leg (back or front) 0 9½ 2¾ 2½ 1 8½ 3¼ 2½ If you lose this book, use the “Rule of Nines” for adults: 5 6½ 4 2¾ 10 5½ 4¼ 3 15 4½ 4½ 3¼ Adult 3½ 4¾ 3½ Palm trick- Use the patient’s palm size to represent approximately 1% TBSA. Imagine a rectangle the width and length of your entire hand (from wrist to fingertips) and that is the size of “one palm.” Estimation of Burn Depth Burns are classified as either first, second or third degree. Superficial Burns First DegreeInjury involving only the outer epidermis layer. Erythema and mild discomfort. Resolves in 48-72 hours with comfort measures. Healing is uneventful. Superficial Second DegreeThe entire epidermis and upper third of the dermis are destroyed. Vessels leak plasma which lifts off the epidermis, causing blister formation. Wounds are pink, wet, and very painful. Heals within two weeks via repopulation of epithelial cells present in skin appendages and the deep dermis. Deep Burns Deep Second DegreeThe injury extends into the dermis, leaving few viable epidermal cells. Reepithelialization is very slow. Wounds require months to heal. Blisters do not form because the dead tissue layer is thick and does not easily lift off the surface. Wounds are red with scattered deeper white areas throughout. The marked decrease in blood flow makes the wound very prone to conversion to a third degree wound. Dermal necrosis with coagulated proteins turns the wound a white to yellow color (called coagulum). Topical antibiotics can add to this color change and make the wound difficult to differentiate from a third degree burn. Wound breakdown is common since the rete pegs have been destroyed; thus, what little epidermis is left is thin and not well adherent. Dense scarring is seen if the wound heals primarily. Third DegreeA full thickness burn. The entire epidermis and dermis are destroyed. No epidermal cells present for reepithelialization. Initially, wound appears waxy and white, unless burn extends into the fat, in which case a leathery brown or black appearance is seen along with coagulated subcutaneous veins. The wound is painless and will not heal unless very small (smaller than 2 X 2cm). Other Burn Injuries Chemical Burns These burns cause progressive tissue damage until inactivated or flushed with water. Acids cause protein coagulation, limiting further penetration., whereas alkali burns combine with cutaneous lipids causing tissue saponification, which continues to injure the skin. Until proven otherwise, chemical burns should be considered deep. Electrical burns Electrical injuries are of three major types which may occur in combination: 1) true electrical injury exists when electricity passes through the body. An entrance and exit wound is produced, along with significant deep-tissue destruction. The quantity of heat produced is expressed in Joule’s Law: J=I2RT, where (J) is the heat produced, I is the current, R is resistance, and T the duration of contact. Therefore when performing the history and physical examination, record the voltage and duration of contact with the source. 2) arc burns occur when electrical current jumps from one part of the body to another, producing scattered spots of injury which may be deep 3) flame burns are caused by sparks sufficient to ignite clothing High-voltage, high-current source electrical injuries (>1000 volts and >5000mA) cause significant soft tissue damage. Low voltage, low current (<1000volts and 5-60mA) cause less soft tissue damage but are noted to more commonly cause cardiac fibrillation. Complications of electrical injuries include tetanic muscle contractions with resulting muscle fractures and dislocations, or falls with crush injuries. Intraperitoneal damage occurs, perhaps due to the low-resistance mesenteric vascular system. Cardiac dysfunction may be seen initially in as many as one third of electrically injured patients, and ECG changes may be present,[i] including RBBB, SVT, and other focal ectopic dysrhythmias.[ii] Electrical injuries may also cause delayed neurologic changes and cataract formation.[iii] Radiation burns Accidents involving ionizing radiation are not common. Most frequently they are the result of a local accident (laboratory), from an industrial accident (Chernobyl, Russia in 1986), or from the detonation of a nuclear device. Whole-body exposure of more than 100 rads causes acute radiation syndrome, marked by nausea, vomiting, diarrhea, fever, fatigue, and headache within hours of exposure. This is followed by a latent period, and then by hemopoietic, GI, and vascular complications. [i] Esses SI, Peters WJ: Electrical burns: pathophysiology and complication. Cand J Surg 24:11-14, 1981. [ii] Robson MC, Smith DJ: Care of the thermally injured patient. In Jurkiewicz MJ, Krizek TJ, Mathes SJ, Ariyan S (eds): Plastic surgery: principles and practice, St. Louis, 1990. Mosby. [iii] Christensen JA, Sherman RT, Balis GA, Waumett JD: Delayed neurologic injury secondary to high voltage currents with recovery, J Trauma 20:166-168, 1980. There are many ways that you can be burned as well as there being more than one way to make an estimation in regard to the percentage of burn injury from thermal or chemical burns. This discussion reviews the depth of burn and the three methods for determining the extent of burn injury using percentages. TCSS, Mike from Santa Barbara First Degree Burn Second Degree Burn Third Degree Burn The Rule of Nines The rule of nines is an anatomical and graphical tool that divides the total body surface area (TBSA) into segments that are multiples of 9%. The percentages used for each body part are different between adults and children. This is the easiest method to use for adults and children older than 10yrs. Adult Rule of Nines Chart Child Rule of Nines Chart Infant Rule of Nines Chart Lund & Browder Chart The Lund & Browder chart is considered the most accurate of all the methods as it assigns a specific number to each body part. This method is most often used to measure burns in infants and young children because it allows for developmental changes in percentages of body surface area. Lund & Browder Chart 5yrs - Adult: Palm Method The palm method is a tool whereby the size of the patients palm is used as an indicator for specific percentage of TBSA. The surface area of a patients palm equals approximately 1% of TBSA. This method is particularly useful where the burn has an irregular shape or has a scattered distribution. 1. STAY SAFE! Do not let the rescuer get burned trying to save the victim. Follow universal precautions and wear personal protective equipment if you have it. 2. Burn treatment begins with stopping the burning process. Cool the burned area with cool running water for several minutes. If an ambulance is coming, continue running water over the burned area until the ambulance arrives. 3. Look for blistering, sloughing, or charred (blackened) skin. Blistering or sloughing (skin coming off) means the top layer of skin is completely damaged and complications are likely. Charring indicates even deeper damage to all three layers of skin (see illustration). If the damaged area is bigger than one entire arm or the whole abdomen, call 911 or take the victim to the emergency department immediately. 4. Victims with burns to the following areas need emergency medical assistance (call 911): o face o hands o feet o genitalia 5. Mild burns with reddened skin and no blisters may be treated with a topical burn ointment or spray to reduce pain. Cool water (not cold or warm) may also help with pain. DO NOT APPLY BUTTER OR OIL TO ANY BURN! 6. Over the counter pain relievers like ibuprofen or acetaminophen can be used for the pain of a mild burn (typically redness only). If stronger pain relief is needed, contact a physician or go to the emergency department. Tips: 1. Burns cause swelling. Burns of the face and neck can sometimes swell enough to cause difficulty breathing (see illustration). If that happens, call 911 immediately. 2. Burns that completely circle the hands or feet may cause such severe swelling that blood flow is restricted. If swollen or tight hands and feet become numb and tingly, blue, cold, or "fall asleep," then call 911 immediately. 3. While the burn is healing, wear loose natural clothing like silks or light cottons. Harsher fabrics will irritate the skin even more. 4. Burns destroy skin and the loss of skin can lead to infection, dehydration and hypothermia (loss of body heat). Make sure that burn victims get emergency medical help if experiencing any of the following: o dizziness or confusion o weakness o fever or chills o shivering o cold sweats