Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
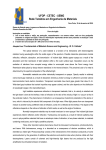
Refraction Patient Acknowledgement Form This form will be retained by your optician and added to your patient health record. A copy of this form will be provided by your optician to the College of Opticians of Ontario for statistical purposes. The information that you provide will be held in the strictest confidence. A. Patient Information—to be completed by the patient Family Name First Name Date of Birth (yyyy/mm/dd) Apartment Number Middle Name Home Telephone Number Work Telephone Number Street Name and Number City Province Postal Code Occupation B. Patient History—to be completed by the patient Have you ever had a complete eye exam? Yes No Do you wear corrective lenses? Yes No Is this your first time receiving a refraction from an optician? Yes No Do you recall the date of that exam? Yes No Date of last complete eye exam: Year Month Day C. Contraindications to Refraction (where No is checked for any of the following)—to be completed by the optician in conjunction with the patient No The patient’s personal health history is clear of diabetes? Yes Yes No The patient has a history of being cataract-free: Yes The patient’s personal health history is clear of glaucoma: Yes No The patient has a history of being free from age-related macular degeneration: Yes The patient’s personal health history is clear of strabismus? Yes No Yes The patient’s visual acuity is correctable to 20/40 in each eye: Patient is over 19 and under 65 years of age: Yes Preliminary evaluation suggests good eye health: No No No No If this review indicates a No to any of the above questions, then the patient MUST be immediately referred to a physician or optometrist for a complete eye exam. This form is two (2) pages and requires that you complete BOTH pages. Version 2.0 Page 1 of 2 This consultation is solely intended to determine your suitability to receive a refraction for the purpose of obtaining corrective lenses by a registered optician. Please be reminded that refraction does not diagnose the health of your eye. A copy of this form will be provided to the College of Opticians of Ontario (COO), where the information contained herein will be used by the COO purely for statistical purposes. The COO understands the importance of protecting personal information, and as such all information listed will be treated by the COO in strict confidence. Signature of patient or guardian: __________________ Date: ___________________ Signature of optician: __________________C#:_______ Date: ___________________ This form is two (2) pages and requires that you complete BOTH pages. Version 1.0 Page 2 of 2