Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
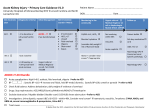
policy forum http://www.kidney-international.org & 2013 International Society of Nephrology Acute kidney injury: global health alert Philip Kam Tao Li1, Emmanuel A. Burdmann2 and Ravindra L. Mehta3, for the World Kidney Day Steering Committee 20134 1 Department of Medicine and Therapeutics, Prince of Wales Hospital, Chinese University of Hong Kong, Shatin, Hong Kong; Department of Medicine, University of Sao Paulo Medical School, Sao Paulo, Brazil and 3Department of Medicine, University of California, San Diego, San Diego, California, USA 2 Acute kidney injury (AKI) is increasingly prevalent in developing and developed countries and is associated with severe morbidity and mortality. Most etiologies of AKI can be prevented by interventions at the individual, community, regional, and in-hospital levels. Effective measures must include community-wide efforts to increase an awareness of the devastating effects of AKI and provide guidance on preventive strategies, as well as early recognition and management. Efforts should be focused on minimizing causes of AKI, increasing awareness of the importance of serial measurements of serum creatinine in high-risk patients, and documenting urine volume in acutely ill people to achieve early diagnosis; there is as yet no definitive role for alternative biomarkers. Protocols need to be developed to systematically manage prerenal conditions and specific infections. More accurate data about the true incidence and clinical impact of AKI will help to raise the importance of the disease in the community, increase awareness of AKI by governments, the public, general and family physicians, and other health-care professionals to help prevent the disease. Prevention is the key to avoid the heavy burden of mortality and morbidity associated with AKI. Kidney International (2013) 83, 372–376; doi:10.1038/ki.2012.427; published online 9 January 2013 KEYWORDS: acute kidney injury; World Kidney Day Correspondence: Sara Martin, World Kidney Day Global Operations Center, Rue du Luxembourg 22–24, Brussels 1000, Belgium. E-mail: [email protected] 4 World Kidney Day (WKD) is a joint initiative of the International Society of Nephrology and the International Federations of Kidney Foundations. WKD Steering Committee members: Miguel Riella (Brazil, co-chair), John Feehally (UK, co-chair), Timur Erk (Turkey), Paul Beerkens (The Netherlands), Guillermo Garcia-Garcia (Mexico), Philip KT Li (Hong Kong), William G. Couser (USA), Georgi Abraham (India), Luca Segantini (Belgium), Sara Martin (Belgium) Received 26 November 2012; accepted 29 November 2012; published online 9 January 2013 372 On 14 March 2013, the 8th World Kidney Day (WKD) will be celebrated. WKD is an annual event jointly organized by the International Society of Nephrology and the International Federation of Kidney Foundations. This year, we aim to alert the public to the global increase in acute kidney injury (AKI) in both developing and developed countries. AKI is a syndrome of abrupt loss of kidney function, often with oliguria, which is strongly associated with increased early and long-term patient morbidity and mortality, as well as the subsequent development of chronic kidney disease (CKD). There is an urgent need for a global health strategy to reduce the enormous growing burden of AKI and its consequences. We advocate that efforts focused on preventing AKI be coupled with early detection and treatment, and adequate follow-up to reduce mortality and the long-term burden of AKI-induced CKD. EPIDEMIOLOGY OF AKI WORLDWIDE The KDIGO (Kidney Disease Improving Global Outcome) Clinical Practice Guideline for AKI defines AKI as any of the following: increase in serum creatinine by X0.3 mg/dl (X26.5 mmol/l) within 48 hours, increase in serum creatinine to X1.5 times baseline, which is known or presumed to have occurred within the prior 7 days, or urine volume o0.5 ml/ kg/h for 6 h.1 An epidemiological study in Scotland showed that the incidence of AKI was 2147 per million population per year (pmp),2 and in a community study in Northern California the annual incidence of non-dialysis-requiring and dialysis-requiring AKI were, respectively, 3841 and 244 p.m.p.;3 this incidence increased over time and was consistently higher in men and in the elderly.3 Unfortunately, there are still no comprehensive studies on the incidence of AKI in the community in the developing world. Recent hospital studies in the developed world report AKI in 3.2–9.6% of admissions, with overall in-hospital mortality around 20%, and up to 50% in ICU patients.4,5 There is also increased long-term mortality in those with AKI surviving hospitalization, with adjusted mortality risk of 1.4, which augmented with increasing severity of AKI.5 AKI requiring renal replacement therapy (RRT) occurs in 5–6% of ICU patients, with an extremely high in-hospital mortality rate of 60%.6 It is estimated that about 2 million people die of AKI Kidney International (2013) 83, 372–376 policy forum PKT Li et al. : Acute kidney injury every year.6,7 Those who survive AKI have a higher risk for later development of CKD.8 AKI IN THE DEVELOPING WORLD Eighty-six per cent of the world’s population lives in low- and middle-income countries, which have many contrasts and inequalities. Sophisticated tertiary hospitals coexist with inadequate primary care and poor health system infrastructure in the same country and even in the same city. In such countries, AKI has a peculiar bimodal presentation. In modern, large, urban centers, the pattern of AKI is very similar to that found in the developed world; it is predominantly a hospital-acquired disease occurring mostly in older, critically ill multiorgan failure patients with substantial comorbidity. The main cause for AKI in this population is renal ischemia, principally due to sepsis, and is often associated with nephrotoxic drugs.9 At the same time, in rural areas or smaller cities in the countryside, AKI will usually be a community-acquired disease, affecting younger and previously healthy individuals. In this population, specific causes of AKI include diarrheal diseases with dehydration, infectious diseases (malaria, dengue, yellow-fever, leptospirosis, tetanus, and human immunodeficiency virus), animal venoms (snakes, bees, Loxosceles spiders, Lonomia caterpillars), septic abortion, dyes, and natural medicines.10–12 Most of these factors triggering AKI are associated with poverty and affect vulnerable populations because of poor sanitation and water hygiene (diarrheal diseases), a lack of education and access to an adequate urban infrastructure, and difficulty in having access to the health-care system (septic abortions, snakebite, natural medicines, tetanus) and breaking of an ecological balance from uncontrolled and unplanned urbanization (leptospirosis, yellow-fever, Africanized bees, and Lonomia caterpillar accidents).10–13 In the developing world, the same ICU may have a typical bacterial sepsis–induced AKI patient side by side with a patient suffering from dengue or tetanus-induced AKI. Increasingly, these causes of AKI may be exported from developing to developed countries because of immigration, business travel, tourism, and world warming. AKI IN THE DEVELOPED WORLD The availability of standardized criteria for diagnosis and staging of AKI has made clear that the prevalence of AKI in the developed world has increased in the past decade.14,15 AKI is now encountered in 45% of patients admitted to the ICU and 20% of hospitalized patients.16,17 This increased prevalence likely reflects an aging population burdened by multiple comorbidities, which is often managed with multiple drugs.18,19 AKI is a multifactorial entity. Etiological factors include prerenal injury contributing to reduced renal perfusion; however, the precipitating events are often iatrogenic, e.g., hypotension during anesthesia and surgery, or profound diarrhea secondary to C. difficile infection resulting from aggressive antibiotic therapy.20 Kidney International (2013) 83, 372–376 Drug-induced kidney injury is recognized as a major factor in about 20% of cases, whereas hospital-acquired infections, sepsis, complex surgery, and diagnostic procedures requiring intravenous contrast continue to be significant risk factors for the development of AKI.21–23 Patients in the ICU are dying of AKI and not just simply with AKI. Experimental and small observational studies have shown that AKI negatively affects immunity and is associated with higher rates of infection.24 AKI patients frequently develop a vicious cycle of immune dysfunction, sepsis, and multiorgan failure. Indeed, severe sepsis is currently the major cause of AKI in the United States.25 The host response to sepsis involves an inflammatory response that activates innate immunity. If this persists, the immune response will lead to a release of a multitude of proinflammatory products, which frequently cause organ dysfunction, including kidney failure.26 A key issue in the developed world is that patients are increasingly cared for by multiple providers, often in different health-care systems, with infrequent or minimal data sharing between providers and across health-care systems. This lack of knowledge often results in overdosing of nephrotoxic medications, for example, a dentist might prescribe large doses of nonsteroidal anti-inflammatory drugs for pain management after dental surgery without the knowledge of a patient’s underlying CKD, thus contributing to development of AKI superimposed on the CKD. As kidney disease is generally silent, unless it is severe enough to reduce urine output or lead to complications, it can often go unrecognized.27 A recent national audit of the care provided to patients who died with a diagnosis of AKI in United Kingdom hospitals revealed several shortcomings. AKI was often diagnosed late in the course, the initial severity was underestimated, and diagnostic and therapeutic interventions were often incomplete or delayed.28 This audit illustrates the urgent need for improving awareness of AKI and has prompted the medical community in the UK to implement specific measures to facilitate early recognition, timely diagnosis, and appropriate management and follow-up of AKI patients.29 AKI IN CHILDREN The epidemiology of pediatric AKI has shifted in the past decades from intrinsic kidney diseases such as hemolytic uremic syndrome and glomerulonephritis to ischemia, nephrotoxins, and sepsis in critically ill children.17 Estimates of the incidence of AKI in children vary depending on the definition used and the population assessed, but it is clearly increasing. A pediatric-modified RIFLE (risk, injury, failure, loss, and end-stage kidney) criterion was developed and validated in 2007. The major difference with the original RIFLE definition is the use of changes in estimated creatinine clearance calculated by Schwartz formula rather than serum creatinine, in view of the large variation in body mass in children.17 Development of AKI has been consistently demonstrated as an independent risk factor for death in children, from neonates to 373 policy forum adolescents. Recently, the concept of ‘renal angina’ was proposed as a tool to the early identification of kidney injury together with early adoption of preventive measures in children at high risk for the development of AKI.30 One of the strongest indicators of ‘renal angina’ and risk of further development of AKI in children is fluid overload.17,30 As in adults, AKI carries a significant risk for late development of CKD in surviving children.17,31 OTHER CONSEQUENCES OF AKI Apart from the high mortality associated with AKI, there are other major consequences. Patients with AKI utilize more resources and have longer hospital lengths of stay partly because of the effect of AKI on other organ functions. For instance, AKI patients have more difficulty being weaned off ventilators.32 AKI patients are more prone to fluid overload, with a resultant increase in mortality and impaired renal recovery.33 When patients leave the hospital, they generally require prolonged recuperation often in skilled nursing facilities and may not recover kidney function.34 In a study of over 4000 type 2 diabetic patients in the Veterans Affairs health-care system in the USA, approximately half required one or more hospitalizations, and among those requiring hospitalization 29% experienced at least one episode of AKI.35 CKD is now recognized as a major noncommunicable disease, and data in the same study of type 2 diabetics showed that AKI was an important independent risk factor for stage 4 CKD (hazard ratio 3.56), with each AKI episode doubling that risk. There is other consistent and increasing evidence that AKI contributes to CKD development and may result in dialysis dependency.8,36 Collectively, these data demonstrate the high personal and community costs of an episode of AKI and stress the pressing need to address this problem in an effective way.37 IS AKI PREVENTABLE AND TREATABLE? A central tenet of the WKD message since 2006 has been that ‘kidney disease is common, harmful, and treatable’. Similar to CKD, AKI is common, harmful, and treatable, and is also largely preventable. The heterogeneity of patients and the broad range of situations where AKI is encountered make it challenging to standardize an approach for evaluating and managing patients with this syndrome. The recent KDIGO guidelines for management of AKI provide a useful reference to assist clinicians for managing AKI; however, the successful implementation of guidelines and their application to individual patients can be slow and requires concerted efforts.1,38 Prevention of AKI starts in the community with prompt assessment of those at risk, for example, in taking prompt action following effective evaluation of the severity of fluid depletion in acute diarrhea. Regular drug therapy can compound that risk, and the many older people taking nonsteroidal anti-inflammatory drugs or renin–angiotensin system blockers should be educated to discontinue them 374 PKT Li et al. : Acute kidney injury temporarily in the face of acute intercurrent illness, a socalled ‘medication holiday’. In the developed world, the growing adoption of electronic medical records provides several opportunities for managing patients through the continuum of outpatient and in-hospital care. Several studies have now shown that active surveillance for changes in creatinine can automate alerts to guide drug dosing and reduce the incidence of druginduced kidney injury.39,40 An ‘AKI sniffer system’ embedded in the electronic medical record to warn physicians of changing renal function has been shown to increase the number and timeliness of early therapeutic interventions.41 The emerging field of kidney-specific biomarkers of damage will additionally offer opportunities to improve care.42 Several studies have now shown the ability of various biomarkers alone or in combination to facilitate earlier diagnosis and improve differential diagnosis of AKI. However, biomarker-guided interventions have not as yet been shown to be of benefit,43 and currently serum creatinine and urinary volume remain the clinical pointers to AKI diagnosis. Given advances in medical informatics, biomarker development and interpretation, and therapeutic interventions, it is now imperative that we leverage these advances to educate physicians and care providers about AKI and provide them with the tools to manage these patients timely and effectively. In the hospital setting, AKI preventive measures continue to be adequate hemodynamic control, hydration, hematocrit and oxygen profiling, and avoidance of nephrotoxic drugs; other preventive maneuvers should be implemented for particular diseases or conditions causing AKI. In the developing world, awareness of the specific infectious or venomous organisms in certain areas will allow environmental protection, vaccines, pharmacological prophylaxis, and early administration of anti-venom. Early and adequate anti-venom administration is a valuable preventive maneuver for snakebite and caterpillar venom–induced AKI, reducing its morbidity and lethality.10,13 Prompt diagnosis, timely hemodialysis, and adequate supportive therapy are associated with improved outcome in tropical infectious disease– associated AKI, such as leptospirosis and malaria.10,44,45 As always, the early diagnosis of AKI is the key to minimize further insults. Prevention for AKI is clearly the key to avoid the heavy burden of mortality and morbidity associated with this syndrome (Table 1), and this will only come about through increasing awareness of the true incidence and clinical impact of AKI among governments, the public, general and family physicians, and other health-care professionals. Most etiologies of AKI can be prevented by interventions at the individual, community, regional, and in-hospital levels. Effective measures must include community-wide efforts to increase an awareness of the devastating effects of this illness and provide guidance on preventive strategies and for early recognition and management. Efforts should be focused on minimizing AKI causes, increasing awareness of the Kidney International (2013) 83, 372–376 policy forum PKT Li et al. : Acute kidney injury Table 1 | Strategies for preventing AKI Government Funding support for acute kidney injury (AKI) research in hospital and community on AKI incidence, outcome, and mortality Funding support for setting up AKI registries Recognition of natural hazards for AKI: water sanitation, flooding, venomous animals Recognition of AKI in common infections: malaria, dengue, leptospirosis, HIV, postinfectious hemolytic uremic syndrome Better obstetric care Collaboration with health-care professionals on educating the public about AKI prevention protecting the kidneys from this lethal syndrome is an important health strategy for the patient and the community. The effective implementation of such strategies will only come when both the general public and the renal community work together to convince health authorities of the pressing need to do this. Government and health authorities must allocate resources to manage this problem both in the developed and developing world. REFERENCES Public Awareness of the potential problems of AKI and avoid unsupervised, indiscriminate, and long-term use of nephrotoxic drugs and natural substances General practitioners and physicians Awareness of patients at risk for AKI and situations contributing to AKI Awareness of prerenal causes of AKI and of the need for early and appropriate rehydration and hemodynamic optimization in hypovolemic patients Awareness of natural and man-made nephrotoxin, nephrotoxic drugs, herbs, and indigenous medicine Judicious use of nephrotoxic drugs and awareness of potential drug interactions Early recognition of AKI and early referral to nephrologists Nephrologists Establish and implement common AKI diagnostic criteria and definitions for prevention, treatment, and research Find new diagnostic tools including inexpensive technology and biomarkers for AKI diagnosis and monitoring Adapt renal replacement therapy to regional needs, technique, and resource availability 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. importance of serial measurements of serum creatinine in high-risk patients, and observing urinary volume to achieve early diagnosis. Protocols need to be developed to systematically manage prerenal conditions and specific infections. RRT FOR AKI When AKI patients require RRT, the current KDIGO recommendations are to deliver an effluent volume of 20–25 ml/kg/h for continuous RRT or to deliver a Kt/V of 3.9 per week when using intermittent or extended RRT.1 This requires careful monitoring, as there is often a significant reduction in the dose delivered versus that prescribed.46 Peritoneal dialysis (PD) should also be considered for AKI, particularly in developing countries, because it is a simple, effective, safe, and relatively inexpensive form of RRT.47 The technical simplicity of PD and the potential to reduce costs if consumables can be made locally present an opportunity to establish cost-effective programs for managing AKI, as has been shown in a recently established PD program for managing AKI in one of the poorest countries in Africa.48 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. CONCLUSION The worldwide celebration of WKD 2013 provides an opportunity to share the message that AKI is indeed common, harmful, preventable, and treatable, and that Kidney International (2013) 83, 372–376 28. 29. KDIGO. Clinical practice guideline for acute kidney injury. Kidney Int 2012; 2(Suppl): 1–138. Ali T, Khan I, Simpson W et al. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol 2007; 18: 1292–1298. Hsu CY, McCulloch CE, Fan D et al. Community-based incidence of acute renal failure. Kidney Int 2007; 72: 208–212. Fang Y, Ding X, Zhong Y et al. Acute kidney injury in a Chinese hospitalized population. Blood Purif 2010; 30: 120–126. Lafrance JP, Miller DR. Acute kidney injury associates with increased longterm mortality. J Am Soc Nephrol 2010; 21: 345–352. Uchino S, Kellum JA, Bellomo R et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA 2005; 294: 813–818. Murugan R, Kellum JA. Acute kidney injury: what’s the prognosis? Nat Rev Nephrol 2011; 7: 209–217. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int 2012; 81: 442–448. Santos WJ, Zanetta DM, Pires AC et al. Patients with ischaemic, mixed and nephrotoxic acute tubular necrosis in the intensive care unit - a homogeneous population? Crit Care 2006; 10: R68. Lombardi R, Yu L, Younes-Ibrahim M et al. Epidemiology of acute kidney injury in Latin America. Semin Nephrol 2008; 28: 320–329. Naicker S, Aboud O, Gharbi MB. Epidemiology of acute kidney injury in Africa. Semin Nephrol 2008; 28: 348–353. Jha V, Rathi M. Natural medicines causing acute kidney injury. Semin Nephrol 2008; 28: 416–428. Abdulkader RC, Barbaro KC, Barros EJ et al. Nephrotoxicity of insect and spider venoms in Latin America. Semin Nephrol 2008; 28: 373–382. Mehta RL, Kellum JA, Shah SV et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 2007; 11: R31. Cruz DN, Ricci Z, Ronco C. Clinical review: RIFLE and AKIN–time for reappraisal. Crit Care 2009; 13: 211. Bellomo R, Kellum JA, Ronco C. Acute kidney injury. Lancet 2012; 380: 756–766. Goldstein SL. Acute kidney injury in children and its potential consequences in adulthood. Blood Purif 2012; 33: 131–137. Chronopoulos A, Cruz DN, Ronco C. Hospital-acquired acute kidney injury in the elderly. Nat Rev Nephrol 2010; 6: 141–149. Waikar SS, Liu KD, Chertow GM. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol 2008; 3: 844–861. Cerda J, Lameire N, Eggers P et al. Epidemiology of acute kidney injury. Clin J Am Soc Nephrol 2008; 3: 881–886. Perazella MA. Drug use and nephrotoxicity in the intensive care unit. Kidney Int 2012; 81: 1172–1178. Zarjou A, Agarwal A. Sepsis and acute kidney injury. J Am Soc Nephrol 2011; 22: 999–1006. Solomon R, Dauerman HL. Contrast-induced acute kidney injury. Circulation 2010; 122: 2451–2455. Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int 2012; 81: 819–825. NIDDKD NIH, Bethesda MD. USRDS 2010 Annual Data Report: Atlas of CKD and ESRD in the United States. 2010. Gonc¸alves GM, Zamboni DS, Câmara NO. The role of innate immunity in septic acute kidney injuries. Shock 2010; 34(Suppl 1): 22–26. Macedo E, Malhotra R, Bouchard J et al. Oliguria is an early predictor of higher mortality in critically ill patients. Kidney Int 2011; 80: 760–767. MacLeod A. NCEPOD report on acute kidney injury- must do better. Lancet 2009; 374: 1405–1406. Prescott AM, Lewington A, O’Donoghue D. Acute kidney injury: top ten tips. Clin Med 2012; 12: 328–332. 375 policy forum 30. 31. 32. 33. 34. 35. 36. 37. 38. 376 Basu RK, Chawla LS, Wheeler DS et al. Renal angina: an emerging paradigm to identify children at risk for acute kidney injury. Pediatr Nephrol 2012; 27: 1067–1078. Mammen C, Al Abbas A, Skippen P et al. Long-term risk of CKD in children surviving episodes of acute kidney injury in the intensive care unit: a prospective cohort study. Am J Kidney Dis 2012; 59: 523–530. Vieira JM Jr, Castro I, Curvello-Neto A et al. Effect of acute kidney injury on weaning from mechanical ventilation in critically ill patients. Crit Care Med 2007; 35: 184–191. Bouchard J, Soroko SB, Chertow GM et al. Program to Improve Care in Acute Renal Disease (PICARD) Study Group. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int 2009; 76: 422–427. Fischer MJ, Brimhall BB, Parikh CR. Uncomplicated acute renal failure and post-hospital care: a not so uncomplicated illness. Am J Nephrol 2008; 28: 523–530. Thakar CV, Christianson A, Himmelfarb J et al. Acute kidney injury episodes and chronic kidney disease risk in diabetes mellitus. Clin J Am Soc Nephrol 2011; 6: 2567–2572. Bydash JR, Ishani A. Acute kidney injury and chronic kidney disease: a work in progress. Clin J Am Soc Nephrol 2011; 6: 2555–2557. Li PK, Chow KM, Matsuo S et al. Asian Chronic Kidney Disease (CKD) Best Practice Recommendations – Positional Statements for Early Detection of CKD from Asian Forum for CKD Initiatives (AFCKDI). Nephrology 2011; 16: 633–641. Fliser D, Laville M, Covic A et al. A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guidelines on Acute Kidney Injury: Part 1: definitions, conservative management and contrast-induced PKT Li et al. : Acute kidney injury 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. nephropathy. Nephrol Dial Transplant (e-pub ahead of print 19 October 2012). Cho A, Lee JE, Yoon JY et al. Effect of an electronic alert on risk of contrast-induced acute kidney injury in hospitalized patients undergoing computed tomography. Am J Kidney Dis 2012; 60: 74–81. Cox ZL, Nelsen CL, Waitman LR et al. Effects of clinical decision support on initial dosing and monitoring of tobramycin and amikacin. Am J Health Syst Pharm 2011; 68: 624–632. Colpaert K, Hoste EA, Steurbaut K et al. Impact of real-time electronic alerting of acute kidney injury on therapeutic intervention and progression of RIFLE class. Crit Care Med 2012; 40: 1164–1170. Mehta RL. Biomarker explorations in acute kidney injury: the journey continues. Kidney Int 2011; 80: 332–334. Endre ZH, Walker RJ, Pickering JW et al. Early intervention with erythropoietin does not affect the outcome of acute kidney injury (the EARLYARF trial). Kidney Int 2010; 77: 1020–1030. Andrade L, de Francesco Daher E, Seguro AC. Leptospiral nephropathy. Semin Nephrol 2008; 28: 383–394. Cerdá J, Bagga A, Kher V et al. The contrasting characteristics of acute kidney injury in developed and developing countries. Nat Clin Pract Nephrol 2008; 4: 138–153. Claure-Del Granado R, Macedo E, Chertow GM et al. Effluent volume in continuous renal replacement therapy overestimates the delivered dose of dialysis. Clin J Am Soc Nephrol 2011; 6: 467–475. Ponce D, Berbel MN, Regina de Goes C et al. High-volume peritoneal dialysis in acute kidney injury: indications and limitations. Clin J Am Soc Nephrol 2012; 7: 887–894. Kilonzo KG, Ghosh S, Temu SA et al. Outcome of acute peritoneal dialysis in northern Tanzania. Perit Dial Int 2012; 32: 261–266. Kidney International (2013) 83, 372–376