Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
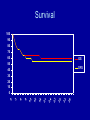
Blood and Marrow Transplantation Francisco F. Lopez, MD Hematology and Medical Oncology Bone Marrow Transplantation 1st BMT Reunion (January 2004) Outline • • • • • • • History Definition Rationale Procedure Indications Our data Summary History of Blood and Marrow Transplantation in the Philippines 1990 1st marrow transplant at the NKTI 2001 1st peripheral blood stem cell transplant at NKTI 2002 St Luke’s Medical Center (SLMC) 2002 Asian Hospital Medical Center (AHMC) 2005 1st autologous stem cell transplant at AHMC 2005 1st cord blood transplant at SLMC The transfusion of the immature progenitor stem cells derived from a donor to the recipient (allogeneic); OR stem cells previously harvested from the patient (autologous). It is NOT an operation / surgical procedure. “Let’s crack your bones wide open!” Stem cells • Young immature cells that make up 0.5% to 5% of the marrow cells. • Express CD34+ • Progenitor cells: self-renew and divide to become red and white cells, and platelets. Stem cells Bone marrow 2 to 5 x 108 TNC/kg weight of recipient with the maximum volume dictated by the weight of the donor (20ml BM aspirate/kg) can be stored at room temperature for up to 24hrs until infusion into the recipient or cryopreserved Peripheral blood 2.0 to 5.0 x 106 CD34+ cells/kg for auto/allo transplants can be stored at 4 C overnight or cryopreserved with dimethyl sulfoxide (DSMO) Umbilical cord 3.7 x 106 TNC/kg recipient body weight can be stored at 4 C or 25 C for up to three days or cryopreserved with DSMO Rationale Two kinds • Allogeneic: Donor – Matched or partially mismatched sibling – Unrelated – Cord blood • Autologous: No donor – Stem cells are harvested from patient Allogeneic transplant • involves the transfer of stem cells from donor to recipient to permanently replace all hematopoietic cells • eradicate malignant cells with high dose chemotherapy +/- radiotherapy • sufficient immunosuppression of the host to allow growth of the allograft • immune mediated graft vs leukemia/lymphoma or graft vs tumor effect Human Leukocyte Antigen (HLA) typing Autologous transplant • Increasing the dose of some chemotherapeutic agents may result in large increase in tumor cell kill • Transfusing previously harvested stem cells of the patient will guarantee bone marrow recovery Procedure Allogeneic transplant Schema -8 admit to hospital -7 Total body Irradiation -6 Total body Irradiation -5 Total body Irradiation -4 Total body Irradiation; Donor starts GCSF -3 Cytoxan (60mg/kg) -2 Cytoxan (60mg/kg) -1 Rest day and start cyclosporine IV 0 Harvest and infusion of stem cells +1 Methotrexate 15mg/mm +3 Methotrexate 10mg/mm +6 Methotrexate 10mg/mm +11 Methotrexate 10mg/mm WBC from day of transplant to recovery 5 4.5 4 3.5 3 2.5 WBC 2 1.5 1 0.5 0 -11 -9 -7 -5 -3 -1 0 1 3 5 7 9 11 13 15 17 Procedure Autologous transplant Procedure: The Harvest D –10 Cyclophosphamide 1.5gm/mm D – 7 Start GCSF 10mcg/kg D–6 D–5 D–4 D–3 D–2 D–1 D 0 Harvest using apheresis machine (collect 2.5 x 106 / kgBW CD 34+ cells) The transplant • • • • • • • • • • • Day Day Day Day Day Day Day Day Day Day Day -8 admit -7 Total body irradiation -6 Total Body irradiation -5 Total body irradiation -4 etoposide 60mg/kg IV -3 rest -2 cytoxan 100mg/kg IV -1 rest 0 infusion of stem cells +5 begin GSCF 5mg/kg/day +10 marrow recovery or engraftment Transfusion of stem cells Indications and Timing of Transplant Allogeneic Transplant Malignant • Acute and chronic leukemias – AML, ALL, CML • • • • Myelodysplastic syndrome (MDS) Lymphomas (failed chemotherapy) Multiple myeloma Myeloproliferative diseases Allogeneic Transplant Non malignant • • • • Aplastic anemia Thalassemia Immune disorders Paroxysmal nocturnal hemoglobinuria (PNH) Autologous Transplant • • • • • Multiple Myeloma Non-Hodgkins Lymphoma Hodgkins Disease Solid Tumors Autoimmune diseases (multiple sclerosis) Allogeneic BMT in Pediatric AML Indications: All except Down’s syndrome t(8;21) t(15;17) inv 16 80 70 60 50 40 30 20 10 0 chemo 1st CR > 1st CR Allogneic BMT in Pediatric ALL Indications: t(9;22) t(4,11) 3rd CR or higher relapse on therapy or w/in 12 months of end of therapy May be offered: > 28 days to achieve CR 2nd CR, relapse > 12 months of end of therapy 90 80 70 chemo good risk 1st CR high risk 60 50 chemo high risk 40 30 2nd CR 20 10 > 2nd CR 0 chemo Severe Aplastic Anemia 80 70 60 50 IST BMT 40 30 20 10 0 OS >40y/o <40y/o Allogneic BMT in adult ALL Poor risk features • WBC > 25,000 • T(9;22) t(8;14) t(4;11) • Age > 30y/o • Extramedullary disease • Requiring more than 4 weeks to achieve a CR 60 50 40 30 20 10 0 chemo 1st CR > 1st CR Allogeneic BMT in adult AML Prognostic indicators that predict outcome of standard chemotherapy based on cytogenetic abnormalities. favorable: t(8;21) t(15;17) inv 16 Intermediate: del y; normal karyotype; 11q23 Poor: all others 70 chemo 60 50 1st CR 40 30 20 10 0 1st relapse/ 2nd CR induct fail/ >2nd relapse 2nd BMT Reunion (January 2005) Complications During BMT • • • • • • • • • • • • • Nausea and Vomiting Nutrition Mouth Sores Diarrhea Infection Renal complications Veno-Occlusive disease of the liver (VOD) Pancytopenia Graft Rejection Acute Graft vs Host Disease Rash Pulmonary complications Death • Nausea and Vomiting – More common during the early part of transplant – Round the clock anti emetic medications – During the recovery phase, nausea / vomiting / abdominal pain (cramps) / diarrhea, the patient may have graft vs host disease (GVHD). • Nutrition – Low bacteria diet: no fresh fruit and vegetables; served hot; no left over; tray should be clean; – Appetite diminishes after chemotherapy – Total parenteral nutrition until patient can eat. • Mouth Sores – Mouth wash (nystatin and biotene) – Morphine pushes or drip when severe (face will be swollen) – Thrush • Diarrhea – Chemotherapy induced (Cuclophosphamide) – Infection: Clostridium Defficile – GVHD (graft vs host disease) – Food induced (avoid creamy, milk, oily food) • Bacterial Infections – Gram negative – Gram positive (central line or skin); patient should shower or sponge bath daily. – Antibiotics: third generation cephalosporin and vancomycin • Fungal – Pulmonary (aspergillus) – Yeast – Amphoteric B prophylaxis • Viral – Herpes zoster – Acyclovir IV Prevention • • • • Isolation room : positive pressure Strict hand washing Mask No need for gown or gloves unless patient is positive for clostridum defficile • Renal Complications – Renal insufficiency – Drugs: cyclosporine, vancomycin, amphotericin B) – Monitor I & 0 accurately every 12 hours. Balance fluid I & 0. lasix IV given prn. • Liver Complications – Veno-Occlusive disease of the liver (VOD) • Water retention • Tender liver • Elevated bilirubin • Elevation in bilirubin and SGPT and SGOT – Medications: cyclosporine, TPN – GVHD • Pancytopenia – Blood and platelet transfusion – Platelet apheresis is always used – Blood and platelets should always be available, filtered and irradiated. • Graft rejection – Engraftment occurs between two to three weeks after transfusion of stem cells – Recipient develops antibodies against the HLA antigen of the donor. – Incidence increases in heavily transfused patients. – Prior transfusions without filter and random donor platelets used • Graft versus host disease – Occurs when donor stem cells recognizes the body of the recipient as foreign and attacks the body. – Acute GVHD occurs during engraftment: diarrhea, elevated bilirubin and rash – GVHD prophylaxis: cyclosporine IV, methotrexate IV • Rash – Drug – GVHD – infection • Pulmonary complications – Pneumonia – Pulmonary congestion • Total fluid per day 3L to 4L – Engraftment syndrome • Mortality – Infection – GVHD – Relapse 3rd BMT Reunion (January 2006) Bone Marrow Transplant Data BMT Data: 27 patients since December 2002 5 4.5 4 3.5 3 2.5 allogeneic 2 1.5 1 0.5 0 2002 2003 2004 2005 2006 2007 BMT Data • December 2002 to April 2007 • 27 stem cell transplants – 22 allogeneic – 5 autologous • Ages: 8 months to 66 years old • Sex: 17M and 10F • Transplant Regimen: – Chemotherapy only: 21 – Fractionated total body irradiation + chemo: 6 • GVHD prophylaxis: – CSA + Methotrexate 17 – CSA + Cellcept 5 BMT Data: Donor • Sex – Same sex: 10 – Opposite sex: 12 • HLA match – Full sibling: 21 – Mismatch: 1(HLA 4/6 from father) BMT Data • 22 allogeneic – Acute myelogenous Leukemia 10 • 1st CR 7 • 2nd CR 1 • Induction failure 2 – Acute lymphoblastic leukemia 4 • 1st CR 1 • > 1st CR 3 – – – – – Myelodysplastic syndrome 4 Chronic myelogenous leukemia 1 Severe aplastic anemia 1 Thalassemia 1 Metastatic (lung & bones) renal cell cancer 1 BMT Data • 5 Autologous – 3 multiple myeloma – 1 relapsed hodgkin’s disease – 1 acute myelogenous leukemia in 2nd CR Results Allogeneic • Harvested stem cells: mean 7 x 106 CD34+ cells / kg BW of patient • Range: 2.9 to 23.6 x 106 CD34+ cells • Days of harvest: mean 2 days • Range 1 to 4 days Autologous • Harvested stem cells: mean 5.1 x 106 CD34+ cells / kg BW of patient • Range: 3.2 to 8.1 x 106 CD34+ cells • Days of harvest: mean 2 days • Range 1 to 4 days Results • Engraftment (allo and auto) – Mean 13 days – Range: 10 to 18 days Morbidity Rejection Acute: Patient with AML 1st CR did not engraft at all. Positive antibodies against HLA. Was salvaged with a second transplant using same donor. Currently doing well and off immuno drugs Delayed: Patient with thalassemia. Graft rejection after 1 year. Autologous recovery of marrow. Transfusion dependent. Acute Graft Vs Host Disease (AGVHD) in BMT • Manifestation of alloreactivity and occurs when mature T cells are transferred to hosts expressing histocompatibility differences • Donor CD4+ and CD8+ target major tissues of the skin, liver and intestinal tract Acute Graft vs Host Disease (GVHD) n = 15/22 Grade 1 2 3 4 # of pts 5 7 2 1 Causes of GVHD Causes • HLA disparity • Conditioning regimen • Sex mismatch • Age • Parous donor • Peripheral blood vs marrow Infection • 8 had either gram (+) or gram (-) bacterial infection • 1 had recurrence of PTB during transplant. He was an auto transplant patient with relapsed hodgkin’s disease, (+) history of treated PTB • 4 had herpes zoster, months after • 1 had anal warts, months after Cytomegalovirus (CMV) • 9/14 developed (+) CMV blood culture within 100 days of transplant. • They were successfully treated with ganciclovir for six weeks. • Risks of developing CMV: – HLA mismatch – AGVHD – (+) serum CMV antibody Mortality n = 11 • Infection (Gm negative septic shock) 2 – 10 and 11 days post transplant – history of prior infections – poor performance status • Severe AGVHD of the GIT 1 • Relapse disease 8 – – – – – 2 ALL > 1st CR 3 myelodysplastic syndrome 1 AML induction failure 1 AML auto 1 multiple myeloma auto survival • • • • Allogeneic: 13/22 Autologous: 3/5 16/27 survivors 1st patient transplanted is now 4yrs and 5 months post transplant • Data may change in time – wait for 2 to 3 years Survival 100 90 80 OS 36 33 30 27 24 21 18 15 12 9 6 DFS 3 0 70 60 50 40 30 20 10 0 Improve outcome • Education and information – Can be done in our country – Dispel myths • • • • Not a surgical procedure Harvesting stem cells is not a painful procedure Maximum hospital stay 6 weeks Live a normal life • Screen candidates • Early transplant and not later on (not a last resort) Burst my bubble! Kicking leukemia away! Survival Cost Cost Factors – Age – Disease and status of disease – Weight – Complications – Regimen used Cost • Range (Php 0.8M to Php 3M) – Adult (Php 1.7M) – Pediatric (Php 1.4M) • Beyond what most Filipinos can afford • The cost of BMT abroad is more expensive – Israel US$ 100,000 – USA $250,000 to $500,000 4rd BMT Reunion (February 2007)