Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Challenges in
cost-utility analysis
in the critical care setting
{
Ville Pettilä MD, PhD, A/P
Helsinki University Hospital
SFAI- veckan / Kalmar
CCM 2006
CCM 2006
- only 19 papers
- max $958,423/ QALY
-$1,150 - $575,000 / life-year
- many < $50,000 /QALY
-
41 studies in critical/intensive care
quality assessed as poor to
moderate
Boston- CEA RegistryQuality of cost-utility analyses
{ .. In the ideal world
Sintonen 1994
{
ARDS N=200
Angus D AMJRCCM 2001
Quality-adjusted survival
Angus DC et al. CCM 2006
Challenge No 1:
Inter-patient variability
{
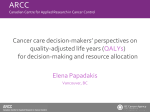
Costs and QALYs – the real world in the ICU
Cost-effectiveness planes
for a treatment
Räsänen P et al. HQLO 2006
Crit Care Med 2003
Challenge No 2:
Inter-diagnoses variability
{
Challenge No 3:
How to adjust for non-survivors?
{
Angus D et al. CCM 2006
Challenge No 4:
Which instrument to use for
quality of life (QOL)?
{
{
SF- (RAND- 36)
EQ-5D
Nottingham Health Profile (NPH)
SIP
etc.
(1) What is an OPTIMAL
QOL measure ?
EQ-5D
*simple
*ESICM recommendation
*one number between 0 and 1
* enables QALY calculations
{
(2) QOL – target
population ?
{
selected vs. unselected
defined vs. all
trauma ?, sepsis? ARDS?
timing of measurement 6(-12) months
post/ICU ?
a cohort or an RCT?
(3) QOL- missing data
Proportion of missing data - < 10%?
How to handle missing data ?
Comparison of patients with missing data
to those with available data !
Adequate sample size !
{
(4) QOL- follow-up and
adjustment ?
{
Were all patients followed ?
What is the optimal time for QOL
measurement ?
Dowdy et al ICM 2006
- 8894 references
- 111 studies
- 21 different patient populations
- 21 studies included
- Different instruments, patient
populations
Dowdy et al. ICM 2005
Challenge No 5:
How to calculate/ estimate quality
of life (QOL)?
{
Challenge No 6:
{
How accurate are the costs?
Indirect costs ?
Costs after hospital discharge?
Challenge No 7:
{
What is the time-frame?
Should it be life-time?
Kaarlola A, Tallgren M, Pettilä V CCM 2006
QALYs after critical care [N=2873]
Kaarlola et al. CCM 2006
Cost-utility after intensive care [N=2873]
Kaarlola et al. CCM 2006
Cost per QALY in severe sepsis (Finnsepsis study) N=480
Key finding: The estimated life-time cost-utility using
QOL at 2 years
after discharge is very reasonable (median 1720€/QALY)
{
Karlsson et al CCM 2009
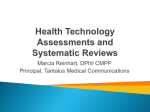
Cost per QALY in acute respiratory failure (FINNALI study) N=958
Cost (euro)
QALY (year)
40000
50
35000
45
40
30000
35
25000
30
20000
25
15000
20
cost, mean
15
10000
10
5000
5
0
0
1624
2534
3544
4554
5564
6574
cost/QALY, mean
QALY, mean
74- >81
80
Age groups
Mean of costs, costs/QALYs and estimated QALYs with 95% CIs
in different age groups for acute respiratory failure patients.
FINNALI, Linko et al. Critical Care 2010
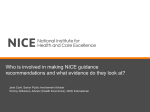
Cost-utility – acute respiratory failure – life-time scale –FINNALI -2007
n
Gained
survival
(yrs)
QALYs (yrs)
Cost/hospital
survivor
Cost/QALY
mean
(SD)
mean (SD)
€
€
Age (yrs)
≤51
252
36 (19)
25 (16)
19195
670
52-63
236
17 (11)
11 (8)
21069
1582
64-74
251
9 (8)
6 (6)
21499
2620
≥75
219
4 (5)
3 (3)
21737
5263
≤31
253
28 (18)
20 (15)
15187
726
32-43
246
18 (16)
11 (12)
22545
1656
44-55
222
13 (15)
8 (11)
23565
2026
≥56
237
8 (13)
5 (9)
24760
2560
Elective
133
16 (14)
12 (12)
17273
1283
Emergency
821
17 (18)
11 (13)
21462
1410
NIV only
105
15 (17)
11 (14)
13154
956
Invasive ventilation only
775
17 (17)
12 (13)
20065
1313
NIV and invasive ventilation before 6 hours
43
11 (16)
6 (9)
42625
3733
NIV and invasive ventilation after 6 hours
35
13 (17)
8 (11)
44971
3499
Sepsis
136
14 (15)
9 (12)
37219
2599
Cardiac insufficiency
192
9 (12)
6 (8)
27322
2779
Pneumonia
114
14 (16)
9 (12)
26368
2106
Post-operative with ventilatory support<1
day
132
17 (15)
12 (12)
11025
836
SAPS II (points)
Admission type
Ventilatory support
ARF risk factors 48 hours before
Linko et al Critical Care 2010
Challenge No 8:
Discount for costs and QALYs included
in the calculations?
{
Challenge No 9
How to present willingness to pay and
probabilities?
{
Challenge No 9:
How to present willingness to pay and
probabilities?
CEACcost effectiveness acceptability curve
{
Cost-effectiveness acceptability
curves-CEACs
Subgroups of patients
according to
gained QALYs
Conclusions
Cost utility studies in critical care lack
scientific validity and robustness
Conclusions
Cost utility studies in critical care lack
scientific validity and robustness
No consensus regarding utility instrument
, calculations, adjustment for missing
data, and representation of data exist
Conclusions
Cost utility studies in critical care lack
scientific validity and robustness
No consensus regarding utility instrument ,
calculations, adjustment for missing data,
and representation of data exists
At their best the available cost utility
studies in critical care may be seen as
clinically valuable estimations of benefit/
harm of the treatment
Conclusion
Cost-utility –studies….
…..the gold standard
1. Representative non-selected population
2. Defined diagnostic group
3. Standardized utility instrument
4. Life-time scale for QALYs gained
5. Preferably all hospital costs/reliable estimate
6. Discount rate
7. Sensitivity analysis regarding different age and
severity of disease
8. Cost-effectivenss plane
9. CEA-curve