Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
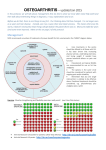
8/15/2012 CASE: DEGENERATIVE JOINT DISEASE A 66-year-old woman who is overweight reports bilateral knee pain of gradual onset during the past several months that increasingly has limited her activities. Last week, when walking down the stairs, she nearly fell when her knee gave way. She does not recall having injured her knee, and she has no morning stiffness and no pain in other joints. She has tried taking up to eight extra-strength (500 mg each) acetaminophen tablets daily without success and has never had ulcers or stomach bleeding. OSTEOARTHRITIS OF THE KNEE DIFFERENTIAL DIAGNOSIS Trauma: ligamentous sprains Meniscal injury Osteoarthritis Patellofemoral pain syndrome Pes anserine bursitis Inflammatory: rheumatoid arthritis, Reiter syndrome Septic arthritis Midlumbar radiculopathy Crystal-induced inflammatory arthropathy: gout, pseudogout Popliteal cyst WHY ME? Risk Factors: • Obesity • Age > 55 yrs • Female • Prior injury/Sports Activities (wrestling, cycling, recreational parachuting, soccer, football) • Muscle weakness • Skeletal asymmetry/malalignment (valgus or varus deformities) Tumor CLINICAL PRESENTATION • Joint pain (medial > lateral) associated with activity (climbing stairs, walking distances, going from seated to standing position) • Decreased range of motion • Morning stiffness that lasts < 30 minutes • Weakness or instability • Crepitus • Effusion THE KNEE EXAM HTTP://WWW.YOUTUBE.COM/WATCH?V=FNUGYNYVHQE Inspection: gait, varus or valgus alignment, swelling, erythema Palpation: joint line tenderness, swelling, warmth, crepitus Specific Testing: Lachman’s: http://www.youtube.com/watch?v=htJiomxxJ7Q&feature=fvw rel McMurry’s: http://www.youtube.com/watch?v=uKvQ_6C3U_o&feature=rel mfu Anterior and Posterior Drawer tests, Valgus and Varus Stress tests, patellar apprehension test. 1 8/15/2012 PATHOPHYSIOLOGY PHYSIOLOGIC CHANGES Two theories of how OA starts: 1. Injury to cartilage, either single event or repetitive microtrauma, that initiates inappropriate repair response. 2. Fundamental defect in cartilage – example type II collagen gene defect. Injury > activation of protease, collagenase, and cytokines > cartilage degradation. • Hyaline articular cartilage is lost > Joint space narrowing. • Capsular stretching • Bone remodeling (subchondral bone cysts and osteophytes) • Synovitis is present in some cases. • Ligamentous laxity also occurs. • Malalignment of joint • Weakness of periarticular muscles DIAGNOSIS CRITERIA FOR OA OF THE KNEE: Presence of knee pain, plus at least 3 of 6 characteristics - Greater than 50 years of age - Morning stiffness for < 30 minutes - Crepitus on active ROM of knee - Boney Tenderness - Boney Enlargement - No palpable warmth Sensitivity 95% and Specificity 69% *American College of Rheumatology DIAGNOSIS CRITERIA EXPANDED: ESR< 40 Rheumatoid Factor Titer < 1:40 Synovial Fluid consistent with OA: clear color, WBC < 2000 Sens 92% and spec 75% Imaging: Indicated if pain is nocturnal or is at rest or doesn’t improve with conventional therapy. Findings do not correlate well with symptoms of OA. 2 8/15/2012 NONPHARM TX NONPHARM TX •ACR Strongly Recommends •ACR Conditionally Recommends • Participate in aerobic and/or resistance land-based exercise • Participate in aquatic exercise • Lose weight (for persons who are overweight) • • • • • • • • • • • WEIGHT LOSS Participate in self-management programs Receive manual therapy in combination with supervised exercise Receive psychosocial interventions Use medially directed patellar taping Wear medially wedged insoles if they have lateral compartment OA Wear laterally wedged subtalar strapped insoles if they have medial compartment OA Be instructed in the use of thermal agents Receive walking aids, as needed Participate in tai chi programs Be treated with traditional Chinese acupuncture Be instructed in the use of transcutaneous electrical stimulation EXERCISE AND DIETARY WEIGHT LOSS IN OVERWEIGHT AND OBESE OLDER ADULTS WITH KNEE OSTEOARTHRITIS: THE ARTHRITIS, DIET, AND ACTIVITY PROMOTION TRIAL Strong associations • Framingham: men 1.5, women 2.1 ADAPT study • • • • • N=316 over 18 mths Healthy lifestyle vs Diet, Exercise, D+E Aerobic + Resistance Exercise 1 hr, 3x/wk Diet – 4.9%, D+E 5.7%, Cont 1.2% 5.7%=11.5 lbs Arthritis & Rheumatism Volume 50, Issue 5, pages 1501-1510, 6 MAY 2004 DOI: 10.1002/art.20256 http://onlinelibrary.wiley.com/doi/10.1002/art.20256/full#fig2 EXERCISE 2006 meta-analysis • 16 studies • Modest, yet clinically important influence on wellbeing EXERCISE Weakness of quadriceps muscle Improve stability of joints Improve pain High/low intensity aerobic 2009 meta-analysis • 32 studies • Land-based exercise has short-term benefits Water vs Land Tai Chi 3 8/15/2012 MALALIGNMENT Medial knee more common • Genu varum Unloader brace Neoprene sleeve 1999 study $350 vs $30 Mean aggregate absolute scores on the WOMAC MALALIGNMENT Mean absolute scores for pain on the thirty-second stair-climbing test. PHARM PHRIENDLY Wedged insoles • Thicker laterally • Decreases medial load RCT showed no reduction in pain PHARM TX PHARM TX ACR strongly recommends ACR conditionally recommends NOT to use • • • • • Acetaminophen Oral NSAIDs Topical NSAIDs Tramadol Intraarticular corticosteroid injections • Chondroitin sulfate • Glucosamine • Topical capsaicin ACR has NO recommendations • Intraarticular hyaluronates • Duloxetine • Opioid analgesics 4 8/15/2012 NSAIDS VS ACETAMINOPHEN 2009 Cochrane meta-analysis, 15 RCTs • • • • • • • • 4000 mg Tyl vs various NSAIDs Tylenol better than placebo… barely NSAIDs better than Tylenol… barely GI adverse effects: NSAID 19%, Tyl 13% Withdrawal due to GI: RR 2.0 GI AE: RR 1.47 COX2 no GI probs No difference in serious GI, renal, CV AEs Overall Pain: Tyl vs Placebo • But mean study length was 6.6 weeks WOMAC: Tyl vs Placebo ACETAMINOPHEN GI EFFECTS 2011, 13 week study Overall Pain: Tyl vs 1200 mg Ibu,var NSAIDs • 3 g Tyl vs 1200 mg Ibuprofen, mono and combo • Similar drop in HGB at end • Worse in combination UTD: ≥2 g/day Overall Pain: Tyl vs 2400 mg Ibu,var NSAIDs HX OF GI BLEED GUIDELINES ANYONE? Still desire NSAID… American College of Rheumatology ACR says… • Mild OA: Tyl > NSAIDs • Mod/Sev OA: consider NSAIDs European League Against Rheumatism GI ulcer but no bleed in 1 year • COX-2 or NSAID + PPI GI bleed in last year • COX-2 + PPI • Tyl primary. NSAIDs for Tyl failure Canadian Consensus Guidelines • Mod/Sev: NSAIDs • Mild: may consider Tyl No NSAID preference 5 8/15/2012 INJECTIONS GLUCOCORTICOID INJECTIONS •Steroids 2004 meta analysis, 10 studies •Roosters (farm friendly) Improvement up to 2 weeks • NNT 1.3 to 3.5 No significance at 16-24 wks • But RR 2.09, NNT 4.4 1 study – no difference in joint space, 2 yrs 50 mg Pred equiv or 20 mg triamcinolone INTRAARTICULAR HYALURONAN 2005 meta-analysis, 22 studies $500/injection • Decr rest pain at 2 to 6 wks • Decr pain at 10 to 14 and 22 to 30 wks • Poorly designed or industry sponsored • Not recommended 2006 Cochrane, 28 studies Cash only Series of 3 to 5 shots • Same as IA steroids at 1 to 4 wks • Slower in onset • Better at 5 to 13 wks SMALLER NEEDLES, DIFFERENT JUICE ACUPUNCTURE 2007 meta-analysis, 11 RCTs Vs sham • Statistically sig difference vs sham • “no or minimally clinical relevant effects” Vs wait list or usual care • Significant and “Marked clinically relevant effects” • Sustained at 6 mths 6 8/15/2012 ACUPUNCTURE GLUCOSAMINE/CHONDROITIN Same authors Glucosamine: 2010 Cochrane An amino sugar which is converted into cartilage proteoglycans that stimulate chondrocyte metabolism and may slow progression of disease process. Vs sham • Significant but not clinically relevant Vs waiting list • Significant and clinically relevant • Gotta be placebo Dose: 500mg TID Chondroitin: A glycosaminoglycan that inhibits action of degradative enzymes. Dose: 1000 – 1200mg daily GLUCOSAMINE/CHONDROITIN OPIOIDS 2006 - Glucosamine/chondroitin Arthritis Intervention Trial (GAIT) - 24 wk, randomized, double-blind trial ACR says… Participants: 1583 > 40yrs with knee pain for > 6 months and radiologic evidence of OA IF Five Groups: No other Tx response and… 1. 500 mg of glucosamine hydrochloride three times daily Does not desire or… 2. 400 mg of sodium chondroitin sulfate three times daily 3. 500 mg of glucosamine plus 400 mg of chondroitin sulfate three times daily 4. 200 mg of celecoxib (Celebrex, Pfizer) daily 5. Placebo Is not a candidate for orthoplasty… THEN Follow APS/AAPM recs Results: Not clinically significant relief from glucosamine and chondroitin as compared to placebo. Outcome measured was % decrease in pain. 2009 – Cochrane Review: 25 RCT of 4963 participants. No statistical significance in reduction of pain, stiffness, or function. OUR PATIENT • • • • • • • Failed trial of Acetaminophen NSAIDs PRN, with food PPI? PT for quad strengthening Weight loss & Exercise Neoprene sleeve > brace Intraarticular corticosteroids REFERENCES Up To Date: “Pharmacologic therapy of osteoarthritis” Last updated 10/16/11. Up To Date: “Nonpharmacologic therapy of osteoarthritis” Last updated 10/20/11. Clinical Practice, N Engl J Med 2006:354;841 – 848 Ringdahl E, Pandit S. Treatment of Knee Osteoarthritis. Am Fam Physician. 2011 Jun 1;83(11):1287-1292. Messier SP, Loeser RF, Miller GD, et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial. Arthritis Rheum. 2004;50(5):1501. Devos-Comby L, Cronan T, Roesch SC. Do exercise and self-management interventions benefit patients with osteoarthritis of the knee? A metaanalytic review. J Rheumatol. 2006;33(4):744. Fransen M, McConnell S. Land-based exercise for osteoarthritis of the knee: a metaanalysis of randomized controlled trials. J Rheumatol. 2009;36(6):1109. Baker K, Goggins J, Xie H, Szumowski K, LaValley M, Hunter DJ, Felson DT. A randomized crossover trial of a wedged insole for treatment of knee osteoarthritis. Arthritis Rheum. 2007;56(4):1198. Kirkley A, Webster-Bogaert S, Litchfield R, et al. The effect of bracing on varus gonarthrosis. J Bone Joint Surg Am 1999;81:539-48. T.E. Towheed, L. Maxwell, M.G. Judd et al. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev (1) (2006) CD004257 Doherty M, Hawkey C, Goulder M, Gibb I, Hill N, Aspley S, Reader S. A randomised controlled trial of ibuprofen, paracetamol or a combination tablet of ibuprofen/paracetamol in community-derived people with knee pain. Ann Rheum Dis. 2011;70(9):1534. Arroll B, Goodyear-Smith F. Corticosteroid injections for osteoarthritis of the knee: meta-analysis. BMJ. 2004;328(7444):869. Arrich J, Piribauer F, Mad P, Schmid D, Klaushofer K, Müllner M. Intra-articular hyaluronic acid for the treatment of osteoarthritis of the knee: systematic review and meta-analysis. CMAJ. 2005;172(8):1039. Bellamy N, Campbell J, Welch V, Gee TL, Bourne R, Wells GA. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD005321. DOI: 10.1002/14651858.CD005321.pub2. Manheimer E, Cheng K, Linde K, Lao L, Yoo J, Wieland S, van der Windt DAWM, Berman BM, Bouter LM. Acupuncture for peripheral joint osteoarthritis. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD001977. DOI: 10.1002/14651858.CD001977.pub2. Manheimer E, Linde K, Lao L, Bouter LM,Berman BM. Meta-analysis: acupuncture for osteoarthritis of the knee. Ann Intern Med. 2007;146(12):868-877. 7 8/15/2012 REFERENCES http://ohsusportsmedicine.blogspot.com/2009/01/knee.html New England Journal of Medicine. Osteoarthritis of the Knee. 2006. New England Journal of Medicine. Glucosamine, Chondroitin Sulfate, and the Two in Combination for Painful Knee Osteoarthritis. 2006. American Family Physician. Treatment of Knee Osteoarthritis. June 2011. http://www.fammed.wisc.edu/integrative/modules/osteoarthritis UpToDate. Diagnosis and Classification of Osteoarthritis. Updated April 2012. UpToDate. Clinical Manifestations of Osteoarthrits. Updated March 2012. Towheed T, Maxwell L, Anastassiades TP, Shea B, Houpt JB, Welch V, Hochberg MC, Wells GA. Glucosamine therapy for treating osteoarthritis. Cochrane Database of Systematic Reviews 2005, Issue 2. Art. No.: CD002946. DOI: 10.1002/14651858.CD002946.pub2. 8