Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
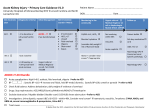
Neonatal Acute Kidney Injury David T. Selewski, MD, MSa, Jennifer R. Charlton, MD, MSb, Jennifer G. Jetton, MDc, Ronnie Guillet, MD, PhDd, Maroun J. Mhanna, MD, MPHe, David J. Askenazi, MD, MPHf, Alison L. Kent, BMBS, FRACP, MDg In recent years, there have been significant advancements in our understanding of acute kidney injury (AKI) and its impact on outcomes across medicine. Research based on single-center cohorts suggests that neonatal AKI is very common and associated with poor outcomes. In this state-of-the-art review on neonatal AKI, we highlight the unique aspects of neonatal renal physiology, definition, risk factors, epidemiology, outcomes, evaluation, and management of AKI in neonates. The changes in renal function with gestational and chronologic age are described. We put forth and describe the neonatal modified Kidney Diseases: Improving Global Outcomes AKI criteria and provide the rationale for its use as the standardized definition of neonatal AKI. We discuss risk factors for neonatal AKI and suggest which patient populations may warrant closer surveillance, including neonates ,1500 g, infants who experience perinatal asphyxia, near term/ term infants with low Apgar scores, those treated with extracorporeal membrane oxygenation, and those requiring cardiac surgery. We provide recommendations for the evaluation and treatment of these patients, including medications and renal replacement therapies. We discuss the need for long-term follow-up of neonates with AKI to identify those children who will go on to develop chronic kidney disease. This review highlights the deficits in our understanding of neonatal AKI that require further investigation. In an effort to begin to address these needs, the Neonatal Kidney Collaborative was formed in 2014 with the goal of better understanding neonatal AKI, beginning to answer critical questions, and improving outcomes in these vulnerable populations. Over the past 15 years, there have been significant advancements in the study of acute kidney injury (AKI) regarding the diagnosis, recognition, intervention, and impact of AKI on morbidity and mortality in critically ill children.1–4 It has become apparent that children who survive an episode of AKI are at increased risk for chronic kidney disease (CKD) and warrant long-term follow-up.5,6 Neonatal AKI studies have begun to show similar conclusions: AKI is common and is associated with poor outcomes.7–12 These studies remain limited to small single-center cohorts using varying definitions of AKI, making generalization difficult. Although progress has been made in our understanding of neonatal AKI, PEDIATRICS Volume 136, number 2, August 2015 a tremendous amount of work is needed to optimize our ability to detect and intervene in newborns with AKI. To advance the field, the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) sponsored a workshop dedicated to neonatal AKI in April 2013. An important result of this meeting was the recognition that collaboration between neonatologists and nephrologists is imperative to advance the study of neonatal AKI and to improve outcomes in these vulnerable patients. In this state-ofthe-art review, we examine aspects of neonatal AKI, including neonatal renal physiology, definitions, risk factors, epidemiology and outcomes, and evaluation and management of AKI. Downloaded from by guest on August 11, 2017 abstract a Division of Nephrology, Department of Pediatrics and Communicable Diseases, C.S. Mott Children’s Hospital, University of Michigan, Ann Arbor, Michigan; bDivision of Nephrology, Department of Pediatrics, University of Virginia, Charlottesville, Virginia; cDivision of Nephrology, Dialysis and Transplantation, Stead Family Department of Pediatrics, University of Iowa Children’s Hospital, Iowa City, Iowa; dDivision of Neonatology, Department of Pediatrics, University of Rochester Medical Center, Rochester, New York; eDivision of Neonatology, Department of Pediatrics, Case Western Reserve University at MetroHealth Medical Center, Cleveland, Ohio; fDivision of Nephrology, Department of Pediatrics, University of Alabama at Birmingham, Birmingham, Alabama; and gDepartment of Neonatology, Centenary Hospital for Women and Children, Canberra Hospital, Australian Capital Territory, Australia Dr Selewski conceptualized and designed the outline of the manuscript, and reviewed and revised the manuscript; Drs Charlton, Jetton, and Kent provided substantial acquisition and assimilation of the data, drafted sections of the manuscript, and critically revised the manuscript; Drs Guillet, Mhanna, and Askenazi critically revised the manuscript; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2014-3819 DOI: 10.1542/peds.2014-3819 Accepted for publication Mar 16, 2015 Address correspondence to Jennifer R. Charlton MD, MS, Department of Pediatrics, University of Virginia, Box 800386, Charlottesville, VA 22908. E-mail: jrc6n@ hscmail.mcc.virginia.edu PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: Dr Askenazi is a speaker for the AKI Foundation; the other authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: No external funding. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. STATE-OF-THE-ART REVIEW ARTICLE NEONATAL RENAL PHYSIOLOGY Although a detailed discussion of renal development is outside the scope of this review, there are a number of features of neonatal renal physiology that are pertinent to AKI in neonates, including the duration of nephrogenesis, renal blood flow, glomerular filtration rate (GFR), and tubular immaturity. Nephrogenesis begins at the fifth week of gestation and continues until 34 to 36 weeks,13 yielding the adult complement of 200 000 to 2.7 million nephrons.14,15 The impact of prematurity, intrauterine growth restriction, and AKI on nephrogenesis has not been fully delineated, but small studies suggest that the extrauterine environment and AKI are detrimental to optimal nephrogenesis.16–19 There are significant changes in neonatal renal blood flow after birth that are relevant to the study of AKI in neonates. In comparison with the 20% to 25% of cardiac output received by the adult kidney, at birth the kidneys receive 2.5% to 4.0% of the cardiac output. Over time, this increases to 6% at 24 hours of life, 10% at 1 week, and 15% to 18% at 6 weeks of age.20–23 The changes in renal blood flow after birth result from increased renal perfusion pressure, increased systemic arteriolar resistance, and decreased renal vascular resistance due to neurohumoral changes with angiotensin II and prostaglandins playing major roles.24 In the fetal and neonatal period, the renin-angiotensin system is critical to normal renal development and blood flow. Angiotensin II, the effector molecule of the renin-angiotensin system, causes vasoconstriction at the afferent and efferent arterioles with the greatest impact at the efferent arteriole.25,26 Prostaglandins represent the most important counter-regulatory molecules in the neonatal period and lead to afferent arteriole dilatation.27 The importance e464 of each of these systems is seen in the exacerbated response that critically ill neonates have to inhibition of these systems by medications when oliguria and/or AKI develops after exposure. GFR represents the most recognized measure of kidney function. In term infants, the GFR improves from 10 to 20 mL/min/1.73 m2 during the first days of life to 30 to 40 mL/min/1.73 m2 by 2 weeks of life. In premature infants, the GFR at birth is even lower and increases slower than in term infants. The GFR improves steadily over the first few months of life, reaching the adult GFR by 2 years of age.28–30 The dynamic nature of the neonatal GFR has implications for the care of neonates particularly with regard to drug exposures, dosing, and susceptibility to the development of AKI. The term neonate has more mature renal tubular function, which can appropriately respond to homeostatic needs. The tubular function is immature in premature infants, with a decreased ability to reabsorb electrolytes and protein and to concentrate urine. This has important implications for the management and diagnosis of AKI in premature infants, who rely on the clinician to appropriately prescribe fluids and replace electrolyte losses. The immaturity of these mechanisms in the neonatal kidneys explains some of the subtleties of urinary findings (fractional excretion of sodium) in neonatal AKI that differ from that in older children. DEFINITION OF NEONATAL AKI AKI is classically defined as a sudden decline in kidney function resulting in derangements in fluid balance, electrolytes, and waste products.31 Currently, the diagnosis of AKI is dependent on a rise in serum creatinine (SCr) or decrease in urine output. Unfortunately, SCr is a suboptimal biomarker as it is a marker of kidney function, not Downloaded from by guest on August 11, 2017 damage. As a result, there is a significant delay in the rise of SCr after an insult (48–72 hours) and a significant amount of function has to be lost before SCr will rise (.50% of the GFR). SCr also has unique challenges in the neonatal population, including the presence of maternal creatinine, varying degrees of creatinine reabsorption in the proximal tubules, overall lower GFRs, and maturational differences.32–35 As a result, there has been a significant amount of research to identify novel biomarkers of damage to allow for the earlier identification of neonates with AKI (up to 48 hours before SCr rise). These novel biomarkers include urine neutrophil gelatinaseassociated lipocalin, cystatin-c, kidney injury molecule-1, and others.36–42 By detecting earlier stages of kidney injury, these biomarkers may allow for prevention of or early intervention in AKI in neonates. Although these biomarkers continue to show promise, currently SCr is the standard used for the diagnosis of AKI in all populations. In 2005, an empirical definition for AKI was introduced into the adult and pediatric literature that recognized stages of severity based on a decrease in GFR and/or urine output. This definition was developed based on evidence that even small changes in SCr were associated with increased morbidity and mortality. Current definitions have demonstrated that even small degrees of AKI are associated with increased morbidity and mortality in children and adults.1,3,43 This empirical definition has evolved based on observational data from millions of patients and hundreds of studies into the Kidney Diseases: Improving Global Outcomes (KDIGO) AKI definition published in 2013, maintaining a 3-tiered categorical staging model depicting mild, moderate, and severe stages of AKI.44 The use of standardized definitions of AKI has allowed comparison between studies and was a fundamental first step that has been SELEWSKI et al integral to the study of AKI in medicine. Before 2008, most neonatal AKI studies used arbitrary definitions of AKI frequently defined by an absolute SCr $1.5 mg/dL. In response to the trends in the diagnosis of AKI, a number of neonatal studies were performed by using the Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease (RIFLE) and Acute Kidney Injury Network (AKIN) definitions of AKI.8,45 One such standardized definition of AKI described in detail by Jetton and Askenazi is based on a modification of the KDIGO definition termed the neonatal modified KDIGO criteria (Table 1). This definition stages AKI based on an absolute rise in SCr from a previous trough and should be used in children ,120 days of age. In April 2013, neonatologists and pediatric nephrologists participating in the NIDDK workshop carefully scrutinized this definition. They concluded that, at this time, this definition offers a reasonable starting point and would allow for consistency throughout studies. As this definition is empirical, large multicenter studies are greatly needed to validate this definition and address all aspects of the definitions, including the degree of SCr rise, age of utilization, and how to deal with a rise in SCr from 0.2 to 0.3 mg/dL, which technically represents a 1.5-fold increase and would qualify as AKI. Some have suggested that the SCr should rise to an absolute value of .0.5 mg/dL and meet the previous criteria to qualify as AKI.1,12 RISK FACTOR FOR NEONATAL AKI Sepsis The change in renal function that defines AKI should be thought of as the result of a combination of susceptibility factors and exposures.44 Although neonates are subject to the same risk factors present in critically ill children of all ages, special consideration must be made to risk factors inherent to neonatal renal development and physiology. Therefore, we will review perinatal and postnatal risk factors associated with AKI, including perinatal events/exposures, sepsis, and nephrotoxic medication exposure that may identify neonates who require enhanced vigilance (Table 2). Sepsis is a cause of significant morbidity and mortality in neonates. Sepsis has been consistently shown to be a risk factor for the development of AKI across neonatal populations, contributing to up to 78% of the cases of AKI.51–54 Mathur et al55 described 200 term neonates with sepsis of whom 52 developed AKI. Those who developed AKI had a lower birth weight and were more likely to have meningitis, disseminated intravascular coagulation, and septic shock. Neonates who develop sepsis are classically thought to be predisposed to AKI secondary to the hypotension associated with systemic inflammation, but there also appears to be a direct impact on the kidneys.56 Furthermore, AKI may develop despite the maintenance of systemic blood pressures and renal blood flow, suggesting that sepsis may directly damage the kidney by effects on microvasculature.56–59 Perinatal Exposures and Events As a result of the unique neonatal renal physiology, a number of maternal exposures and perinatal events can lead to neonatal AKI. For example, maternal exposure to nonsteroidal anti-inflammatory drugs predisposes neonates to oliguria and AKI.47 The multiple roles of the reninangiotensin system in renal development prenatally, as well as the maintenance of renal blood flow postnatally, can lead to a broad range of outcomes in the newborns exposed to angiotensin-converting enzyme inhibitors ranging from renal agenesis to AKI, depending on the timing and duration of exposure. Perinatal risk factors associated with the development of AKI are outlined in Table 2 and include low Apgar scores, intubation, low cord pH, and asystole.8–10,12,45,47–50 TABLE 1 Neonatal AKI KDIGO Classification Stage SCr 0 1 No change in SCr or rise ,0.3 mg/dL SCr rise $ 0.3 mg/dL within 48 h or SCr rise $1.5–1.9 3 reference SCra within 7 d SCr rise $2.0–2.9 3 reference SCra SCr rise $3 3 reference SCra or SCr $2.5 mg/dLb or Receipt of dialysis 2 3 Urine Output $ 0.5 mL/kg/h ,0.5 mL/kg/h for 6 to 12 h ,0.5 mL/kg/h for $ 12 h ,0.3 mL/kg/h for $24 h or anuria for $12 h Differences between the proposed neonatal AKI definition and KDIGO include the following: a Reference SCr will be defined as the lowest previous SCr value. b SCr value of 2.5 mg/dL represents ,10 mL/min/1.73m2 . PEDIATRICS Volume 136, number 2, August 2015 Downloaded from by guest on August 11, 2017 Nephrotoxic Medications Nephrotoxic medications are known to be a cause of AKI across the spectrum of critically ill and hospitalized children.60,61 Exposure to nephrotoxic medications is also associated with AKI in neonates and may represent a modifiable risk factor.47,48,62 Table 3 provides a description of common nephrotoxic medications used in the NICU. In 2013, Rhone et al62 evaluated the epidemiology and impact of nephrotoxic medication exposure in 107 very low birth weight (VLBW) infants. In this study, 87% of neonates were exposed to at least 1 nephrotoxic medication and on average these neonates were exposed to 14 days of nephrotoxic medications during their NICU stay. Although this study represents an important step, the epidemiology of exposure to nephrotoxic medications in general NICU populations remains unstudied. e465 TABLE 2 Risk Factors for AKI in Neonates Study Size Risk Factors Associated With AKI Cataldi et al 200548 Study Premature infants Population 172 Cuzzolin et al 200647 Premature infants 246 Koralkar et al 201110 VLBW 229 Viswanathan et al 201265 ELBW 472 Mathur et al 200655 Selewski et al 201312 Neonates with sepsis Asphyxiated neonates undergoing therapeutic hypothermia 200 96 Bruel et al 2013103 Premature infants (,33 wk) 1461 Gadepalli et al 20118 Bolat et al 201354 Congenital diaphragmatic hernia General NICU 68 1992 Askenazi et al 201363 Birth weight .2000 g, gestational age .34 wk, 5-min Apgar ,7 Low Apgar scores, exposure to ampicillin, ceftazidime, ibuprofen Maternal nonsteroidal anti-inflammatory drugs during pregnancy, intubation at birth, low Apgar scores, ibuprofen administration to infant Lower birth weight, lower gestational age, lower Apgar scores, UAC, mechanical ventilation, inotrope support High mean airway pressures, lower mean arterial pressures, higher exposure to cefotaxime Lower birth weight, meningitis, DIC, and shock Asystole at the time of birth, clinical seizures before cooling, persistent pulmonary hypertension, elevated gentamicin or vancomycin levels, pressor support, transfusions Serum sodium variation, PDA, catecholamine treatment, nosocomial infections, BPD, cerebral lesions, neonatal surgery Lower 5-min Apgar score, AKI correlated with left-sided CDH Pregnancy-induced hypertension, PPROM, antenatal corticosteroids, SGA, birth weight ,1500 g, endotracheal intubation, UVC, ibuprofen therapy for PDA closure, sepsis Lower birth weight, male, lower Apgar scores at 5 min, lower cord pH, mechanical ventilation 58 BPD, bronchopulmonary dysplasia; CDH-congenital diaphragmatic hernia; DIC, disseminated intravascular coagulation; PPROM, preterm premature rupture of membranes; UAC, umbilical artery catheter; UVC, umbilical venous catheter. poor outcomes (Table 4).8–12,45,62–64 Here we review AKI studies in some exemplar patient populations. EPIDEMIOLOGY AND OUTCOMES OF NEONATAL AKI There have been a number of singlecenter studies that have evaluated the impact of AKI in VLBW neonates, extremely low birth weight (ELBW) neonates, sick near-term/term neonates, neonates on extracorporeal membrane oxygenation (ECMO), and asphyxiated newborns showing that AKI is common and associated with VLBW and ELBW Neonates There have been 3 large singlecenter studies to date that have evaluated AKI in VLBW neonates (500–1500 g).10,65,66 In 2011, Koralkar et al10 reported on 229 VLBW infants followed prospectively from birth TABLE 3 Common Nephrotoxic Medications in NICU Drug Acyclovir Angiotensin-converting enzyme inhibitors Aminoglycosides Amphotericin B Nonsteroidal antiinflammatory drugs Radiocontrast agents Vancomycin e466 Mechanism Urinary precipitation, especially with low flow and hypovolemia, with renal tubular obstruction and damage and decreased GFR. May cause direct tubular toxicity (metabolites). Decreased angiotensin II production inhibiting compensatory constriction of the efferent arteriole to maintain GFR. Toxic to the proximal tubules (transport in the tubule, accumulate in lysosome, intracellular rise in reactive oxygen species and phospholipidosis, cell death); intrarenal vasoconstriction and local glomerular/mesangial cell contraction. Distal tubular toxicity, vasoconstriction, and decreased GFR. Decreased afferent arteriole dilatation as a result of inhibiting prostaglandin production resulting in reduced GFR. Renal tubular toxicity secondary to increase in reactive oxygen species; intrarenal vasoconstriction may play a role. Mechanism of AKI unclear, possible mechanism includes proximal tubular injury with generation of reactive oxygen species. Downloaded from by guest on August 11, 2017 until 36 weeks postmenstrual age. The incidence of AKI, by using the neonatal modified KDIGO criteria, was 18%. The mortality in infants with AKI was significantly higher than those without AKI (42% vs 5%, P , .001). After adjusting for potential confounders, those with AKI had a significantly higher chance of death (hazard ratio 2.4, 95% confidence interval [CI] 0.95–6.0; P , .06). Viswanathan et al65 reported similar findings in a retrospective singlecenter study, where 12.5% (59/472) of all ELBW infants developed AKI and mortality among those with AKI was significantly higher than controls (70% vs 22%, respectively). In a large retrospective study of VLBW infants, Carmody et al66 examined 455 VLBW infants and found an AKI incidence of 39.8%. In this study, AKI was independently associated with increased mortality (odds ratio 4.0, 95% CI 1.4–11.5) and length of stay (11.7 hospital days, 95% CI 5.1–18.4). Perinatal Asphyxia Infants with perinatal asphyxia have been recognized as a group that is at high risk of AKI. Recently there have SELEWSKI et al TABLE 4 Neonatal AKI Studies Study Population Definition Askenazi et al 200945 VLBW infants (n = 195) AKIN criteria Gadepalli et al 20118 RIFLE criteria Kaur et al 20119 Congenital diaphragmatic hernia on ECMO (n = 68) Perinatal asphyxia (n = 36) Koralkar et al 201110 VLBW infants (n = 229) Askenazi et al 201363 Alabbas et al 201364 AKIN criteria Neonatal Modified KDIGO criteria Sick near-term neonates (n = 58) Neonatal Modified KDIGO criteria Cardiac surgery ,28 d (n = 122) AKIN criteria Selewski et al 201311,12 Perinatal asphyxia (n = 96) Neonatal Modified KDIGO criteria Zwiers et al 201369 ECMO ,28 d (n = 242) RIFLE criteria Rhone et al 201362 VLBW infants (n = 107) Carmody et al 201466 VLBW infants (n = 455) Neonatal Modified KDIGO criteria Neonatal Modified KDIGO criteria been 2 single-center studies that have looked at the incidence of AKI by using modern AKI definitions. Kaur et al9 reported an incidence of AKI of 41.7%. Selewski et al12 evaluated newborns undergoing therapeutic hypothermia for perinatal asphyxia and found that 36 (38%) of 96 had AKI. Even after controlling for important potential confounders, children with AKI on average were ventilated 4 days longer (P , .001) and hospitalized 3.4 days longer (P = .023). In addition, these investigators also showed that AKI during therapeutic hypothermia was associated with abnormal brain MRI findings at 7 to 10 days of life, implicating AKI as a potential marker for neurologic outcomes.11 ECMO Neonates supported with ECMO represent a unique patient population that is particularly prone to AKI based on the severity of their illness and the inflammatory response that accompanies exposure to the extracorporeal circuit.67,68 Zwiers et al69 evaluated AKI in 242 neonates on ECMO over a 14-year period showing an AKI incidence of 64% and PEDIATRICS Volume 136, number 2, August 2015 Incidence of AKI, % Findings Matched case-control AKI is associated with increased mortality study after adjustment for confounders 71.0 Increased risk of mortality at highest level of AKI (Failure) 41.7 Modern staging systems (AKIN) capture AKI previously missed by previous standard of SCr .1.5 mg/dL 18.0 Adjusting for severity of illness, AKI was associated with increased mortality 15.6 AKI associated with increased mortality and positive fluid balance 62.0 Severe AKI (Stage III) was associated with increased mortality and length of stay after adjusting for severity of illness. 38.0 AKI predicted prolonged mechanical ventilation, length of stay, and abnormal brain MRI findings at 7–10 d of life 64.0 Increased risk of mortality at highest level of AKI (Failure) 26.2 AKI is associated with nephrotoxic medication exposure 39.8 AKI associated with increased mortality and length of stay adjusted for severity of illness a mortality of 65% when AKI progressed to the highest stage. These mirror the findings of Gadepalli et al8 in neonates with congenital diaphragmatic hernia on ECMO where AKI occurred in 71% of neonates, and those with the highest stage of AKI had a mortality of 73%. Neonatal Cardiac Surgery The association of AKI with cardiac surgery in older children has been well studied and the association of AKI with increased mortality is clear. Alabbas et al64 published a retrospective study of 122 neonates (,28 days) showing that AKI occurred in 62% of the neonates. The highest stage of AKI was associated with increased mortality and increased ICU length of stay. These findings are similar to the findings reported by Blinder et al7 in 430 infants (,90 days) undergoing cardiac surgery. EVALUATION AND MANAGEMENT OF NEONATAL AKI The evaluation of a neonate who develops AKI requires a systematic approach, which frequently involves Downloaded from by guest on August 11, 2017 evaluating prerenal, intrinsic, and postrenal causes. We highlight important aspects of the evaluation. A detailed clinical history should include assessment of gestational age, antenatal (ultrasounds), maternal (nephrotoxic medication), birth (fetal heart rate monitoring and resuscitation), and postnatal (nephrotoxic medications, hypotension) events. The physical examination should focus on volume status and vital signs. A thorough evaluation of volume status also requires assessment of serum electrolytes, fluid balance, and, importantly, body weight. Utilization of these 3 measurements can assist in determining both hypovolemia from insensible losses, as well as hypervolemia from fluid overload. Assessment of fractional excretion of sodium can help to differentiate the prerenal (hypovolemia) from intrinsic (acute tubular necrosis) causes of AKI, although in premature infants this metric may not be as helpful. Finally, to evaluate potential postrenal (obstruction) causes of AKI, an ultrasound should be obtained. After the diagnosis of AKI, it becomes important to prevent the e467 development of sequelae. Daily evaluation of medications and the participation of a pharmacist are paramount in the management of the critically ill neonate to monitor drug levels and avoid nephrotoxic exposures when clinically feasible. Strict documentation of all fluid input and output, serum electrolytes, and weight is essential to optimize fluid status. Tracking cumulative fluid overload provides a global assessment of fluid status. Hypervolemia may dictate intervention and nephrology consultation. There are sparse data documenting interventions that can prevent AKI in at-risk patients or ameliorate AKI once it is established. In neonates with perinatal asphyxia, adenosine receptor antagonists (theophylline) may prevent AKI by inhibiting the adenosine-induced vasoconstriction. Several independent randomized studies in asphyxiated infants have shown that prophylactic theophylline, given early after birth, was associated with better kidney function.70–73 As a result, the KDIGO guidelines recommend a single dose of theophylline for asphyxiated infants at risk for AKI.44 Caution must be taken, as theophylline has some potentially harmful neurologic effects.74 Other drugs that have been studied to prevent the development of AKI and improve renal blood flow include dopaminergic agonists (dopamine and fenoldopam).75–77 Although each of these agents has shown promise in the prevention of AKI, the clinical studies have been mixed, and firm recommendations on their use cannot be made. Diuretics are frequently used in patients with AKI in attempts to maintain urine output. Studies in critically ill patient populations have not demonstrated a beneficial effect of diuretics on outcomes and have occasionally demonstrated worse outcomes in patients with AKI treated e468 with diuretics. For example, in a retrospective case-control study, bumetanide was shown to improve the urine output of ELBW infants with AKI at the expense of increasing their SCr.78 In another study, bumetanide was also shown to increase significantly the urine output, in premature infants with oliguric AKI, but at the expense of a transient increase in SCr.79 Despite the lack of evidence in neonates, a trial of diuretics in oliguric neonates with AKI is warranted given the complexity of renal replacement therapy. Large-scale multicenter trials of these medications in neonates are greatly needed. Because of the lack of successful strategies to prevent or ameliorate AKI, the primary therapy for severe cases of AKI is renal replacement therapy. Indications for renal replacement therapy in neonates include refractory acidosis, uremia, electrolyte abnormalities, inability to provide adequate nutrition, and fluid overload. The association between fluid overload and mortality in critically ill patients is one of the hottest topics in acute care nephrology and warrants special mention. Pediatricians have been at the forefront of identifying fluid overload as a risk factor for mortality in critically ill patients.80 This is highlighted by the findings of the prospective pediatric continuous renal replacement therapy (CRRT) registry. Sutherland et al81 showed in a prospective registry of 227 children who were on CRRT that those with a percentage fluid overload ,20% at initiation of renal replacement therapy had improved rates of survival compared with those with a cumulative fluid balance .20% (46% vs 68%, P , .01). These findings have since been verified in a number of different pediatric patient populations highlighting the importance of fluid overload and the timing of renal replacement therapy in critically ill children.82–85 Downloaded from by guest on August 11, 2017 Recent data extend these findings to critically ill children and adults independent of renal replacement therapy.86–88 The impact of fluid overload is highlighted in the practice guidelines proposed by the American College of Critical Care Medicine for pediatric and neonatal septic shock, which recommend that interventions to address fluid balance are warranted when critically ill children amass 10% volume overload.89 Limited data are available on fluid overload in neonates. Askenazi et al63 showed that sick late preterm neonates with AKI had a higher median fluid overload at day of life 3 than those without AKI (+8.2% vs –4%, P , .001). As fluid overload is a potentially modifiable risk factor for mortality, research into its impact on neonatal outcomes is critical to provide information to clinicians about fluid provision and the timing of renal replacement therapy. Throughout adult and pediatric intensive care medicine, renal replacement therapy has transitioned from being a “last-ditch effort” to an early therapy directed at supporting the critically ill patient by maintaining electrolyte homeostasis, allowing for provision of adequate nutrition, and preventing/reducing hypervolemia. This mindset of early intervention has not fully reached the neonatal population, possibly because of the added risk of dialysis machines, ethical considerations, and a lack of studies that illustrate the role of fluid overload on poor outcomes in these patients. Renal replacement therapy poses particular challenges in the neonate, as most equipment was designed for older children. Currently, peritoneal dialysis (PD) is the modality of choice in infants. PD is technically easier, as there is no need for vascular access or an extracorporeal blood circuit.90 If peritoneal dialysis is felt to be a short-term requirement, a temporary catheter can be placed. Several studies describe successful peritoneal dialysis by several SELEWSKI et al different techniques in critically ill neonates as small as 830 g.91–95 When PD is technically difficult because of abdominal wall defects, skin infections, communication to the pleural space, or high ultrafiltration needs, CRRT can be performed. CRRT is performed with a hemodialysis catheter placed in a central location and either regional or systemic anticoagulation. The volume of the extracorporeal circuit is particularly critical in the neonatal population and often these neonates will require that the CRRT machine be primed with blood if the circuit volume exceeds 10% to 15% of the total blood volume.96 In the United States, current CRRT machines are approved only for those weighing .20 kg, but these machines have been used offlabel in children ,5 kg.97 There are a number of considerations when evaluating CRRT in a neonate, including center expertise, prescription, and error rates of current machines, which has been recognized and led to the development of neonatal CRRT machines.98 CRRT systems, such as CARPEDIEM99 (Bellco, Mirandola, Italy) and Nidus,100 are being used in countries outside the United States in neonates. These machines show promise, as they have smaller extracorporeal volumes and are highly accurate. Despite these recent advances, the evidence on the practice of renal replacement therapy in neonates is limited to single-center case series with a complete lack of multicenter data. CONSEQUENCES AND FOLLOW-UP OF NEONATAL AKI Previously, it was assumed that those who survived an episode of AKI would recover kidney function without long-term effects. Recent data from animals,101 critically ill children,5,6 and adults102 with AKI suggest that survivors are at risk for the development of CKD. Mammen et al5 reported that 10% of children who developed AKI in the PICU had PEDIATRICS Volume 136, number 2, August 2015 GFR ,60 mL/min/1.73 m2, 1 to 3 years later. Perhaps even more alarming was the finding that nearly 50% of this cohort was found to be “at risk” for CKD. The role that AKI plays in the development of CKD in the neonatal population is unknown. Several case reports document that CKD occurs in infants who had AKI; however, these studies are small, single-center retrospective reports. Recognizing the long-term implications of AKI, the most recent KDIGO practice guidelines recommend that all patients who experience AKI be evaluated after 3 months for new onset or worsening of CKD.44 They caution that even if CKD is not present at that time, those with AKI are considered to have increased risk for CKD long-term. Although these recommendations are likely pertinent to infants, currently there is not enough firm evidence to make formal follow-up recommendations after episodes of neonatal AKI. General pediatricians should consider neonates who have suffered AKI at increased risk and monitor blood pressure with consideration of further testing on a case-by-case basis. Large longitudinal multicenter studies designed to follow neonates after critical illness are greatly needed to define the most appropriate surveillance protocols, as well as identify those most at risk. CONCLUSIONS Neonatal AKI represents a rapidly evolving area in clinical research, but a significant amount of work remains to improve the outcomes in these patients. An important first step moving forward is the development of a standardized definition of AKI. Initially, the neonatal modified KDIGO AKI definition will be used as common nomenclature to unify and compare research in neonatal AKI. Although this definition represents the best available, it remains limited in that it has not been systematically Downloaded from by guest on August 11, 2017 studied in a multicenter manner evaluating the association of AKI with outcomes. Further work in neonatal AKI needs to focus on defining risk factors, the implications of fluid balance, renal replacement therapy, and the long-term outcomes, including the development of CKD in this susceptible population. After the NIDDK-sponsored workshop on neonatal AKI, an international, multi-institutional, multidisciplinary group, the Neonatal Kidney Collaborative, was formed. This group aims to answer some of the questions surrounding neonatal AKI with the goal of improving outcome and optimizing care for these vulnerable patients. ABBREVIATIONS AKI: acute kidney injury CRRT: continuous renal replacement therapy CKD: chronic kidney disease ECMO: extracorporeal membrane oxygenation ELBW: extremely low birth weight GFR: glomerular filtration rate KDIGO: Kidney Diseases: Improving Global Outcomes NIDDK: National Institute of Diabetes and Digestive and Kidney Diseases PD: peritoneal dialysis SCr: serum creatinine VLBW: very low birth weight infants REFERENCES 1. Selewski DT, Cornell TT, Heung M, et al. Validation of the KDIGO acute kidney injury criteria in a pediatric critical care population. Intensive Care Med. 2014;40(10):1481–1488 2. Sutherland SM, Ji J, Sheikhi FH, et al. AKI in hospitalized children: epidemiology and clinical associations in a national cohort. Clin J Am Soc Nephrol. 2013;8(10):1661–1669 e469 3. Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL. Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int. 2007;71(10):1028–1035 4. Alkandari O, Eddington KA, Hyder A, et al. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care. 2011;15(3):R146 5. Mammen C, Al Abbas A, Skippen P, et al. Long-term risk of CKD in children surviving episodes of acute kidney injury in the intensive care unit: a prospective cohort study. Am J Kidney Dis. 2012;59(4):523–530 6. Askenazi DJ, Feig DI, Graham NM, Hui-Stickle S, Goldstein SL. 3–5 year longitudinal follow-up of pediatric patients after acute renal failure. Kidney Int. 2006;69(1):184–189 7. Blinder JJ, Goldstein SL, Lee VV, et al. Congenital heart surgery in infants: effects of acute kidney injury on outcomes. J Thorac Cardiovasc Surg. 2012;143(2):368–374 8. Gadepalli SK, Selewski DT, Drongowski RA, Mychaliska GB. Acute kidney injury in congenital diaphragmatic hernia requiring extracorporeal life support: an insidious problem. J Pediatr Surg. 2011;46(4):630–635 9. Kaur S, Jain S, Saha A, et al. Evaluation of glomerular and tubular renal function in neonates with birth asphyxia. Ann Trop Paediatr. 2011;31(2): 129–134 10. Koralkar R, Ambalavanan N, Levitan EB, McGwin G, Goldstein S, Askenazi D. Acute kidney injury reduces survival in very low birth weight infants. Pediatr Res. 2011;69(4):354–358 11. Sarkar S, Askenazi DJ, Jordan BK, et al. Relationship between acute kidney injury and brain MRI findings in asphyxiated newborns after therapeutic hypothermia. Pediatr Res. 2014;75(3):431–435 12. Selewski DT, Jordan BK, Askenazi DJ, Dechert RE, Sarkar S. Acute kidney injury in asphyxiated newborns treated with therapeutic hypothermia. J Pediatr. 2013;162(4):725–729.e1 13. Hinchliffe SA, Sargent PH, Howard CV, Chan YF, van Velzen D. Human e470 intrauterine renal growth expressed in absolute number of glomeruli assessed by the disector method and Cavalieri principle. Lab Invest. 1991;64(6): 777–784 14. Abrahamson DR. Glomerulogenesis in the developing kidney. Semin Nephrol. 1991;11(4):375–389 15. Bertram JF, Douglas-Denton RN, Diouf B, Hughson MD, Hoy WE. Human nephron number: implications for health and disease. Pediatr Nephrol. 2011;26(9): 1529–1533 16. Rodriguez MM, Gomez AH, Abitbol CL, Chandar JJ, Duara S, Zilleruelo GE. Histomorphometric analysis of postnatal glomerulogenesis in extremely preterm infants. Pediatr Dev Pathol. 2004;7(1):17–25 17. Faa G, Gerosa C, Fanni D, et al. Marked interindividual variability in renal maturation of preterm infants: lessons from autopsy. J Matern Fetal Neonatal Med. 2010;23(suppl 3): 129–133 18. Sutherland MR, Gubhaju L, Moore L, et al. Accelerated maturation and abnormal morphology in the preterm neonatal kidney. J Am Soc Nephrol. 2011;22(7):1365–1374 19. Carmody JB, Charlton JR. Short-term gestation, long-term risk: prematurity and chronic kidney disease. Pediatrics. 2013;131(6):1168–1179 20. Rudolph AM, Heymann MA, Teramo KAW, Barrett CT, Raiha NCR. Studies on the circulation of the previable fetus. Pediatr Res. 1971;5:452–465 21. Jose PA, Fildes RD, Gomez RA, Chevalier RL, Robillard JE. Neonatal renal function and physiology. Curr Opin Pediatr. 1994;6(2):172–177 22. Paton JB, Fisher DE, DeLannoy CW, Behrman RE. Umbilical blood flow, cardiac output, and organ blood flow in the immature baboon fetus. Am J Obstet Gynecol. 1973;117(4): 560–566 23. Yao LP, Jose PA. Developmental renal hemodynamics. Pediatr Nephrol. 1995; 9(5):632–637 24. Saint-Faust M, Boubred F, Simeoni U. Renal development and neonatal adaptation. Am J Perinatol. 2014;31(9): 773–780 25. Wolf G. Angiotensin II and tubular development. Nephrol Dial Transplant. 2002;17(suppl 9):48–51 Downloaded from by guest on August 11, 2017 26. Yosipiv IV, El-Dahr SS. Developmental biology of angiotensin-converting enzyme. Pediatr Nephrol. 1998;12(1): 72–79 27. Gleason CA. Prostaglandins and the developing kidney. Semin Perinatol. 1987;11(1):12–21 28. Brion LP, Fleischman AR, McCarton C, Schwartz GJ. A simple estimate of glomerular filtration rate in low birth weight infants during the first year of life: noninvasive assessment of body composition and growth. J Pediatr. 1986;109(4): 698–707 29. Vieux R, Hascoet JM, Merdariu D, Fresson J, Guillemin F. Glomerular filtration rate reference values in very preterm infants. Pediatrics. 2010;125(5). Available at: www. pediatrics.org/cgi/content/full/125/ 5/e1186 30. Abitbol CL, Seeherunvong W, Galarza MG, et al. Neonatal kidney size and function in preterm infants: what is a true estimate of glomerular filtration rate? J Pediatr. 2014;164(5): 1026–1031.e2 31. Jetton JG, Askenazi DJ. Acute kidney injury in the neonate. Clin Perinatol. 2014;41(3):487–502 32. Drukker A, Guignard JP. Renal aspects of the term and preterm infant: a selective update. Curr Opin Pediatr. 2002;14(2):175–182 33. Miall LS, Henderson MJ, Turner AJ, et al. Plasma creatinine rises dramatically in the first 48 hours of life in preterm infants. Pediatrics. 1999;104(6). Available at: www.pediatrics.org/cgi/ content/full/104/6/e76 34. Guignard JP, Drukker A. Why do newborn infants have a high plasma creatinine? Pediatrics. 1999;103(4). Available at: www.pediatrics.org/cgi/ content/full/103/4/e49 35. Auron A, Mhanna MJ. Serum creatinine in very low birth weight infants during their first days of life. J Perinatol. 2006; 26(12):755–760 36. Sarafidis K, Tsepkentzi E, Diamanti E, et al. Urine neutrophil gelatinaseassociated lipocalin to predict acute kidney injury in preterm neonates. A pilot study. Pediatr Nephrol. 2014;29(2): 305–310 SELEWSKI et al 37. Tabel Y, Elmas A, Ipek S, Karadag A, Elmas O, Ozyalin F. Urinary neutrophil gelatinase-associated lipocalin as an early biomarker for prediction of acute kidney injury in preterm infants. Am J Perinatol. 2014;31(2):167–174 48. Cataldi L, Leone R, Moretti U, et al. Potential risk factors for the development of acute renal failure in preterm newborn infants: a casecontrol study. Arch Dis Child Fetal Neonatal Ed. 2005;90(6):F514–F519 38. Genc G, Ozkaya O, Avci B, Aygun C, Kucukoduk S. Kidney injury molecule-1 as a promising biomarker for acute kidney injury in premature babies. Am J Perinatol. 2013;30(3):245–252 49. Aggarwal A, Kumar P, Chowdhary G, Majumdar S, Narang A. Evaluation of renal functions in asphyxiated newborns. J Trop Pediatr. 2005;51(5): 295–299 39. Sarafidis K, Tsepkentzi E, Agakidou E, et al. Serum and urine acute kidney injury biomarkers in asphyxiated neonates. Pediatr Nephrol. 2012;27(9): 1575–1582 50. Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr. 2005;42(9): 928–934 61. Menon S, Kirkendall ES, Nguyen H, Goldstein SL. Acute kidney injury associated with high nephrotoxic medication exposure leads to chronic kidney disease after 6 months. J Pediatr. 2014;165(3):522–527.e2 51. Stojanovic V, Barisic N, Milanovic B, Doronjski A. Acute kidney injury in preterm infants admitted to a neonatal intensive care unit. Pediatr Nephrol. 2014;29(11):2213–2220 62. Rhone ET, Carmody JB, Swanson JR, Charlton JR. Nephrotoxic medication exposure in very low birth weight infants. J Matern Fetal Neonatal Med. 2014;27(14):1485–1490 52. Momtaz HE, Sabzehei MK, Rasuli B, Torabian S. The main etiologies of acute kidney injury in the newborns hospitalized in the neonatal intensive care unit. J Clin Neonatol. 2014;3(2): 99–102 63. Askenazi DJ, Koralkar R, Hundley HE, Montesanti A, Patil N, Ambalavanan N. Fluid overload and mortality are associated with acute kidney injury in sick near-term/term neonate. Pediatr Nephrol. 2013;28(4):661–666 53. Vachvanichsanong P, McNeil E, Dissaneevate S, Dissaneewate P, Chanvitan P, Janjindamai W. Neonatal acute kidney injury in a tertiary center in a developing country. Nephrol Dial Transplant. 2012;27(3):973–977 64. Alabbas A, Campbell A, Skippen P, Human D, Matsell D, Mammen C. Epidemiology of cardiac surgeryassociated acute kidney injury in neonates: a retrospective study. Pediatr Nephrol. 2013;28(7):1127–1134 54. Bolat F, Comert S, Bolat G, et al. Acute kidney injury in a single neonatal intensive care unit in Turkey. World J Pediatr. 2013;9(4):323–329 65. Viswanathan S, Manyam B, Azhibekov T, Mhanna MJ. Risk factors associated with acute kidney injury in extremely low birth weight (ELBW) infants. Pediatr Nephrol. 2012;27(2):303–311 40. Askenazi DJ, Koralkar R, Hundley HE, et al. Urine biomarkers predict acute kidney injury in newborns. J Pediatr. 2012;161(2):270–275.e1 41. Askenazi DJ, Montesanti A, Hunley H, et al. Urine biomarkers predict acute kidney injury and mortality in very low birth weight infants. J Pediatr. 2011;159 (6):907–912.e1 42. Askenazi DJ, Koralkar R, Levitan EB, et al. Baseline values of candidate urine acute kidney injury biomarkers vary by gestational age in premature infants. Pediatr Res. 2011;70(3):302–306 43. Schneider J, Khemani R, Grushkin C, Bart R. Serum creatinine as stratified in the RIFLE score for acute kidney injury is associated with mortality and length of stay for children in the pediatric intensive care unit. Crit Care Med. 2010; 38(3):933–939 44. Kidney Disease; Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):1–138 45. Askenazi DJ, Griffin R, McGwin G, Carlo W, Ambalavanan N. Acute kidney injury is independently associated with mortality in very low birthweight infants: a matched case-control analysis. Pediatr Nephrol. 2009;24(5):991–997 46. Jetton JG, Askenazi DJ. Update on acute kidney injury in the neonate. Curr Opin Pediatr. 2012;24(2):191–196 47. Cuzzolin L, Fanos V, Pinna B, et al. Postnatal renal function in preterm newborns: a role of diseases, drugs and therapeutic interventions. Pediatr Nephrol. 2006;21(7):931–938 PEDIATRICS Volume 136, number 2, August 2015 55. Mathur NB, Agarwal HS, Maria A. Acute renal failure in neonatal sepsis. Indian J Pediatr. 2006;73(6):499–502 56. Blatt NB, Srinivasan S, Mottes T, Shanley MM, Shanley TP. Biology of sepsis: its relevance to pediatric nephrology. Pediatr Nephrol. 2014;29(12):2273–2287 57. Sakr Y, Dubois MJ, De Backer D, Creteur J, Vincent JL. Persistent microcirculatory alterations are associated with organ failure and death in patients with septic shock. Crit Care Med. 2004;32(9):1825–1831 comes of age. Kidney Int. 2012;81(4): 338–340 60. Goldstein SL, Kirkendall E, Nguyen H, et al. Electronic health record identification of nephrotoxin exposure and associated acute kidney injury. Pediatrics. 2013;132(3). Available at: www.pediatrics.org/cgi/content/full/ 132/3/e756 66. Carmody JB, Swanson JR, Rhone ET, Charlton JR. Recognition and reporting of AKI in very low birth weight infants. Clin J Am Soc Nephrol. 2014;9(12): 2036–2043 67. Mildner RJ, Taub N, Vyas JR, et al. Cytokine imbalance in infants receiving extracorporeal membrane oxygenation for respiratory failure. Biol Neonate. 2005;88(4):321–327 58. Vincent JL, De Backer D. Microvascular dysfunction as a cause of organ dysfunction in severe sepsis. Crit Care. 2005;9(suppl 4):S9–S12 68. Kurundkar AR, Killingsworth CR, McIlwain RB, et al. Extracorporeal membrane oxygenation causes loss of intestinal epithelial barrier in the newborn piglet. Pediatr Res. 2010;68(2): 128–133 59. Venkatachalam MA, Weinberg JM. The tubule pathology of septic acute kidney injury: a neglected area of research 69. Zwiers AJ, de Wildt SN, Hop WC, et al. Acute kidney injury is a frequent complication in critically ill neonates Downloaded from by guest on August 11, 2017 e471 receiving extracorporeal membrane oxygenation: a 14-year cohort study. Crit Care. 2013;17(4):R151 70. Eslami Z, Shajari A, Kheirandish M, Heidary A. Theophylline for prevention of kidney dysfunction in neonates with severe asphyxia. Iran J Kidney Dis. 2009; 3(4):222–226 71. Cattarelli D, Spandrio M, Gasparoni A, Bottino R, Offer C, Chirico G. A randomised, double blind, placebo controlled trial of the effect of theophylline in prevention of vasomotor nephropathy in very preterm neonates with respiratory distress syndrome. Arch Dis Child Fetal Neonatal Ed. 2006; 91(2):F80–F84 72. Bakr AF. Prophylactic theophylline to prevent renal dysfunction in newborns exposed to perinatal asphyxia—a study in a developing country. Pediatr Nephrol. 2005;20(9):1249–1252 73. Jenik AG, Ceriani Cernadas JM, Gorenstein A, et al. A randomized, double-blind, placebo-controlled trial of the effects of prophylactic theophylline on renal function in term neonates with perinatal asphyxia. Pediatrics. 2000; 105(4). Available at: www.pediatrics. org/cgi/content/full/105/4/E45 74. Al-Wassia H, Alshaikh B, Sauve R. Prophylactic theophylline for the prevention of severe renal dysfunction in term and post-term neonates with perinatal asphyxia: a systematic review and meta-analysis of randomized controlled trials. J Perinatol. 2013;33(4): 271–277 75. Landoni G, Biondi-Zoccai GG, Tumlin JA, et al. Beneficial impact of fenoldopam in critically ill patients with or at risk for acute renal failure: a meta-analysis of randomized clinical trials. Am J Kidney Dis. 2007;49(1):56–68 76. Kellum JA, M Decker J. Use of dopamine in acute renal failure: a meta-analysis. Crit Care Med. 2001;29(8):1526–1531 77. Bellomo R, Chapman M, Finfer S, Hickling K, Myburgh J; Australian and New Zealand Intensive Care Society (ANZICS) Clinical Trials Group. Low-dose dopamine in patients with early renal dysfunction: a placebo-controlled randomised trial. Lancet. 2000; 356(9248):2139–2143 78. Merheb RC, Kruzer KA, Mhanna MJ. The effect of bumetanide in extremely low e472 birth weight infants with acute kidney injury during their first weeks of life. Journal of Clinical Pediatric Nephrology. 2014;2(1):53–63 79. Oliveros M, Pham JT, John E, Resheidat A, Bhat R. The use of bumetanide for oliguric acute renal failure in preterm infants. Pediatr Crit Care Med. 2011;12 (2):210–214 80. Goldstein SL, Currier H, Graf CD , Cosio CC, Brewer ED, Sachdeva R. Outcome in children receiving continuous venovenous hemofiltration. Pediatrics. 2001;107(6):1309–1312 81. Sutherland SM, Zappitelli M, Alexander SR, et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: the prospective pediatric continuous renal replacement therapy registry. Am J Kidney Dis. 2010; 55(2):316–325 82. Selewski DT, Cornell TT, Lombel RM, et al. Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med. 2011;37(7):1166–1173 83. Foland JA, Fortenberry JD, Warshaw BL, et al. Fluid overload before continuous hemofiltration and survival in critically ill children: a retrospective analysis. Crit Care Med. 2004;32(8): 1771–1776 84. Gillespie RS, Seidel K, Symons JM. Effect of fluid overload and dose of replacement fluid on survival in hemofiltration. Pediatr Nephrol. 2004; 19(12):1394–1399 85. Hayes LW, Oster RA, Tofil NM, Tolwani AJ. Outcomes of critically ill children requiring continuous renal replacement therapy. J Crit Care. 2009; 24(3):394–400 86. Arikan AA, Zappitelli M, Goldstein SL, Naipaul A, Jefferson LS, Loftis LL. Fluid overload is associated with impaired oxygenation and morbidity in critically ill children. Pediatr Crit Care Med. 2012; 13(3):253–258 87. Bouchard J, Soroko SB, Chertow GM, et al; Program to Improve Care in Acute Renal Disease (PICARD) Study Group. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int. 2009;76(4):422–427 Downloaded from by guest on August 11, 2017 88. Macedo E, Bouchard J, Soroko SH, et al; Program to Improve Care in Acute Renal Disease Study. Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit Care. 2010;14(3):R82 89. Brierley J, Carcillo JA, Choong K, et al. Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine [published correction appears in Crit Care Med. 2009;37(4): 1536]. Crit Care Med. 2009;37(2): 666–688 90. Kaddourah A, Goldstein SL. Renal replacement therapy in neonates. Clin Perinatol. 2014;41(3):517–527 91. Harshman LA, Muff-Luett M, Neuberger ML, et al. Peritoneal dialysis in an extremely low-birth weight infant with acute kidney injury. Clin Kidney J. 2014; 7(6):582–585 92. Alparslan C, Yavascan O, Bal A, et al. The performance of acute peritoneal dialysis treatment in neonatal period. Ren Fail. 2012;34(8):1015–1020 93. Unal S, Bilgin L, Gunduz M, Uncu N, Azili MN, Tiryaki T. The implementation of neonatal peritoneal dialysis in a clinical setting. J Matern Fetal Neonatal Med. 2012;25(10):2111–2114 94. Oyachi N, Obana K, Kimura S, Kubo M, Naito A, Nemoto A. Use of a flexible Blake(R) silicone drains for peritoneal dialysis in the neonatal intensive care unit. Pediatr Int. 2011;53(3):417–418 95. Yu JE, Park MS, Pai KS. Acute peritoneal dialysis in very low birth weight neonates using a vascular catheter. Pediatr Nephrol. 2010;25(2):367–371 96. Bridges BC, Askenazi DJ, Smith J, Goldstein SL. Pediatric renal replacement therapy in the intensive care unit. Blood Purif. 2012;34(2): 138–148 97. Askenazi DJ, Goldstein SL, Koralkar R, et al. Continuous renal replacement therapy for children ,/=10 kg: a report from the prospective pediatric continuous renal replacement therapy registry. J Pediatr. 2013;162(3):587–592.e3 98. Ronco C, Garzotto F, Ricci Z. CA.R.PE.DI.E. M. (Cardio-Renal Pediatric Dialysis Emergency Machine): evolution of continuous renal replacement SELEWSKI et al therapies in infants. A personal journey. Pediatr Nephrol. 2012;27(8):1203–1211 99. Ronco C, Garzotto F, Brendolan A, et al. Continuous renal replacement therapy in neonates and small infants: development and first-in-human use of a miniaturised machine (CARPEDIEM). Lancet. 2014;383(9931): 1807–1813 PEDIATRICS Volume 136, number 2, August 2015 100. Hothi DK. Designing technology to meet the therapeutic demands of acute renal injury in neonates and small infants. Pediatr Nephrol. 2014;29(10): 1869–1871 101. Basile DP. The endothelial cell in ischemic acute kidney injury: implications for acute and chronic function. Kidney Int. 2007;72(2):151–156 Downloaded from by guest on August 11, 2017 102. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and metaanalysis. Kidney Int. 2012;81(5):442–448 103. Bruel A, Rozé JC, Flamant C, Simeoni U, Roussey-Kesler G, Allain-Launay E. Critical serum creatinine values in very preterm newborns. PLoS ONE. 2013; 8(12):e84892 e473 Neonatal Acute Kidney Injury David T. Selewski, Jennifer R. Charlton, Jennifer G. Jetton, Ronnie Guillet, Maroun J. Mhanna, David J. Askenazi and Alison L. Kent Pediatrics 2015;136;e463; originally published online July 13, 2015; DOI: 10.1542/peds.2014-3819 Updated Information & Services including high resolution figures, can be found at: /content/136/2/e463.full.html References This article cites 83 articles, 11 of which can be accessed free at: /content/136/2/e463.full.html#ref-list-1 Citations This article has been cited by 5 HighWire-hosted articles: /content/136/2/e463.full.html#related-urls Subspecialty Collections This article, along with others on similar topics, appears in the following collection(s): Fetus/Newborn Infant /cgi/collection/fetus:newborn_infant_sub Neonatology /cgi/collection/neonatology_sub Nephrology /cgi/collection/nephrology_sub Permissions & Licensing Information about reproducing this article in parts (figures, tables) or in its entirety can be found online at: /site/misc/Permissions.xhtml Reprints Information about ordering reprints can be found online: /site/misc/reprints.xhtml PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Downloaded from by guest on August 11, 2017 Neonatal Acute Kidney Injury David T. Selewski, Jennifer R. Charlton, Jennifer G. Jetton, Ronnie Guillet, Maroun J. Mhanna, David J. Askenazi and Alison L. Kent Pediatrics 2015;136;e463; originally published online July 13, 2015; DOI: 10.1542/peds.2014-3819 The online version of this article, along with updated information and services, is located on the World Wide Web at: /content/136/2/e463.full.html PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Downloaded from by guest on August 11, 2017