Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
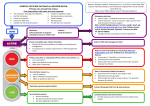
Wessex Cardiovascular Clinical Network Foot Care Quality Standards Amputation is one of the most feared complications of diabetes yet many are preventable. Amputations reduce quality and quantity of life. Reducing the number of amputations among people living with diabetes in Wessex has been a key aim of the Wessex Cardiovascular Clinical Network. The network is delighted to have supported the development of the Wessex quality standards for diabetic foot care. These standards set out the care that people with diabetes and foot disease should expect to receive and that commissioners and providers should strive to provide. The implementation of the standards across Wessex aims to reduce variation in care and improve outcomes for people with this distressing condition. Dr Hermione Price Wessex Diabetes Clinical Lead Tier 1 Primary Care Ref Quality Standard Metric Data source options P1 All practice patients with diabetes will have an annual foot check and will be classified according to risk of foot ulceration. 9 care processes QOF or local system Note: Plans for foot checks must be established irrespective of where patients live i.e residential care, prison, etc. Exclusions should be highlighted. % of patients with a record of foot exam (pulses and neuropathy testing) in last 12months and foot classified as: low; increased/moderate; high risk or ulcer present P2 Every person receiving a foot check should be informed of their foot risk status. % of patients aware of ulceration risk Local patient survey/evidence of appropriate information given P3 Every person receiving a foot check should be offered appropriate education, including written information relevant to their risk of foot ulceration. % of patients offered appropriate education Patient survey/local audit P4 All healthcare professionals undertaking foot checks should have attended a competency update within the previous 2 years. % of practices that have appropriately trained personnel Practice education plan. Education provider record P5 Every person identified as being at moderate or high risk must be referred to the Foot Protection Service (FPS). % of at risk patients referred to FPS Practice profile and/ or referral data Tier 2/3 Community Foot Protection Service (FPS) Ref Quality Standard Metric Data source options C1 Patients with diabetes who are house-bound or in residential care homes should have an equivalent level of access to foot protection. Evidence of local activity by site Provider data % of residential care residents with diabetes under the care of the FPS or Multidisciplinary Foot Service (MDFS) Local audit Those people at moderate or high risk of foot ulceration should be under the care of the FPS. % of patients at moderate/ high risk attending the FPS Provider data C3 The FPS will be coordinated by a named podiatrist who will have appropriate skills and experience. Named clinician and contact details known across pathway Pathway information and job role C4 All moderate/high risk patients should be able to access the FPS within NICE Guideline NG19 timescales*. % of patients seen within NG19 timescales Provider data C2 Local audit Local audit *NG 19 and 24hrs are guideline targets. Commissioners and providers should be working towards these and benchmark current wait times. Tier 4 Hospital Inpatient and Multidisciplinary Foot Service (MDFS) Ref Quality Standard Metric Data source options M1 A MDFS should be available for those with a foot care emergency. Evidence of commissioned service Review of local care pathway and specification M2 A named consultant should be accountable for the overall care of the MDFS. Named clinician and contact details known across pathway Pathway information and job role M3 A clear referral pathway to the MDFS should be widely available (paper and electronic). Evidence of local pathway Review of local care pathway M4 All patients who develop a foot care emergency Time between initial should be reviewed promptly by the MDFS team and assessment by HCP and review within 24hrs*. by MDFS National diabetes foot ulcer audit M5 Each hospital should have an inpatient foot care pathway for all people with diabetes. Inpatient podiatrist post Service specification Compliance with national audit and evidence of local pathway National Diabetes Inpatient Audit % of patients with hospital acquired infections and/or pressure ulcers to heels in inpatients with diabetes Local audit M6 FPS and MDFS should be able to provide patients with the evidence-based interventions recommended by the NICE CG19 guideline. % of patients with access to evidence based interventions e.g. contact casting Exception reporting M7 All patients with diabetes undergoing lower limb amputation should be reviewed both pre- and postoperatively by the specialist diabetes team. % of patients reviewed by diabetes MDT pre- and postamputation Provider data and local audit M8 For patients requiring amputation each should have an individualised plan considering their medical needs and social circumstances to maximise clinical outcomes. % of patients with post surgical personalised care plan Provider data and local audit Quality Improvement Actions required by CCGs Ref Quality Standard Metric Data source options Q1 CCGs to require providers to produce robust plans for root cause analysis (RCA) for amputations. Completed RCAs as a total number and % of all diabetes related amputations Evidence of RCA reports completed Q2 CCGs to require providers to respond to the National Diabetes Foot Care Audit and National Diabetes Inpatient Audit. Completed audit returns Evidence of submission to national audit programme Q3 CCGs to set target for reduction ambitions for the number of major and minor amputations. Number of amputations and rate per 1000 people with diabetes National diabetes foot care profiles Q4 CCGs to set targets for reduction ambitions for hospital nights stay and episodes of care associated with diabetic foot complications. Number of hospital nights stay National diabetes and episodes of care foot care profiles Bibliography and further information • P utting Feet First: Diabetes UK position on preventing amputations and improving foot care for people with diabetes; Diabetes UK, October 2015. • Diabetic Foot Problems, Prevention and Management; National Clinical Guideline 19; NICE; August 2015 • G uidance documents on prevention and management of foot problems in diabetes: development of an evidence-based global consensus; The International Working Group on the Diabetic Foot (IWGDF); 2015 • 2016/17 General Medical Services (GMS) contract Quality and Outcomes Framework (QOF), NHS England, April 2016 • Diabetes foot care activity profiles, Public Health England, August 2016 • National Diabetes Foot Care Audit, NHS Digital, March 2016 • National Diabetes Inpatient Audit, NHS Digital, June 2016 Wessex Clinical Networks: www.wessexscn.nhs.uk Clinical Senate: www.wessexsenate.nhs.uk Published: November 2016 Review date: November 2018 “Working together for lifelong quality care” CS43921 – NHS Creative – November 2016